A vaccine is any biologically derived substance that elicits a protective immune response when administered to a susceptible host. The first documented account of vaccination is attributed to a Buddhist nun who described how smallpox scabs were dried, ground, and blown into the nostrils of susceptible persons in approximately AD 1000 to protect them from disseminated disease.1 The first trial to evaluate the effects of vaccination occurred in 1796, when Edward Jenner proved that persons inoculated with cowpox were resistant to challenge with Variola virus, the etiologic agent of smallpox.
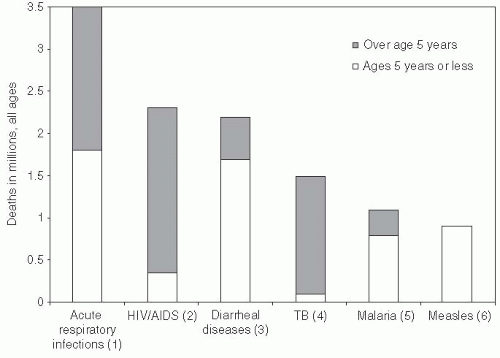
Worldwide improvements in sanitation and vaccination led to impressive declines in the incidence and mortality of many infectious diseases throughout the 1900s. Perhaps the greatest public health achievement of the modern era is the global eradication of smallpox in 1977 and the near elimination of polio. Despite these achievements, a significant proportion of the estimated 11.5 million deaths attributed to infectious and parasitic diseases in 1998 could have been prevented by existing vaccines (Figure 11-1). Barriers to achieving protective immunity in populations at the highest risk leave us far short of reaping the full potential of vaccines. In the world, 1 million children die from measles each year, 50% of whom live in Africa, despite the existence of highly effective vaccine. Furthermore, diseases such as tuberculosis may not come under control until an efficacious vaccine is developed.
Figure 11-1 Leading causes of death worldwide from infectious diseases in 1998. Adapted from World Health Organization(1999). Report on Infectious Diseases: Leading Infectious Killers. http://www.who.int/infectious-disease-report/pages/graph5.html. Accessed February 29, 2012.
This chapter describes various types of traditional and experimental vaccines, the role of vaccines in the eradication of specific infectious diseases (e.g., smallpox, polio), and recent technological advances in vaccine development. In addition, it summarizes fundamental concepts relating to vaccine efficacy and effectiveness and barriers to achieving adequate vaccine coverage.
ACTIVE VERSUS PASSIVE IMMUNIZATION
Protection from many infectious diseases can be conferred by either passive or active immunization.
Passive immunity refers to the protection conferred by the transfer of animal or human antibody (immunoglobulin), by injection, in utero transfer, or breastfeeding, to a susceptible host. Passive antibody transfer from mother to child plays an important role in preventing disease in newborns. Although maternal antibodies do not necessarily provide full protection from infection, immunization of pregnant women against tetanus has led to dramatic reductions in the incidence of neonatal tetanus.2 A disadvantage of passive immunity is that it is typically short lived. For example, protection conferred by immunoglobulin injection lasts only a few weeks; maternal antibodies can protect newborns for up to 6 months, especially if mothers continue to breastfeed.
Active immunity refers to protection produced by the host’s own immune system and relies on the ability of the host to generate an immune response following exposure to specific antigen(s). In the field of immunology, antigens are described as being self if they are from the host or person, and non-self if they come from someone or something else. Immunogenic antigens are foreign bodies—commonly proteins or polysaccharides—that are recognized by the immune system as non-self and that then elicit a response. The goal of immunization is to elicit a protective immune response that confers protective immunity against natural infection with a wild-type (i.e., pathogenic) microorganism without causing serious clinical illness. For many pathogens, the immunologic response of people who have had natural infection and survived without chronic morbidity can guide in the development of a vaccine. Features of an ideal vaccine are listed in Exhibit 11-1.
Factors that affect the host immune response include the type and dose of antigen, the route of administration (e.g., intramuscular, subcutaneous, or oral), the presence or absence of maternal antibody, host factors (e.g., age, immunosuppression, genetics), and the characteristics of the vaccine (Exhibit 11-1). Timing of immunization is another important consideration. For most vaccines, immunization must take place before natural infection occurs, with several weeks passing before the body is able to generate an adequate immune response. During some outbreaks (e.g., hepatitis A, measles), passive immunization offers effective short-term protection, especially when there is insufficient time for susceptible individuals’ bodies to mount an adequate immune response following active immunization. The extent of the host’s immune response has an important bearing on vaccine efficacy, which is discussed in detail later in this chapter.
Exhibit 11-1 Characteristics of an Ideal Vaccine
Produces a good humoral, cell-mediated, and local immune response, similar to natural infection, in a single dose.
Elicits protections against clinical disease and reinfection.
Provides protection for several years, preferably a lifetime.
Results in minimal immediate adverse effects or mild disease with no delayed effects that predispose to other diseases.
Induced immunity confers protections to multiple strains of organisms.
Can be administered simply in a form that is practically, culturally, and ethically acceptable to the target population.
Vaccine preparations do not require special handling (e.g., a cold chain).
Does not interfere significantly with the immune response to other vaccines given simultaneously.
Costs and benefits associated with receiving the vaccine clearly outweigh the costs and risks associated with natural infection.
TYPES OF VACCINES
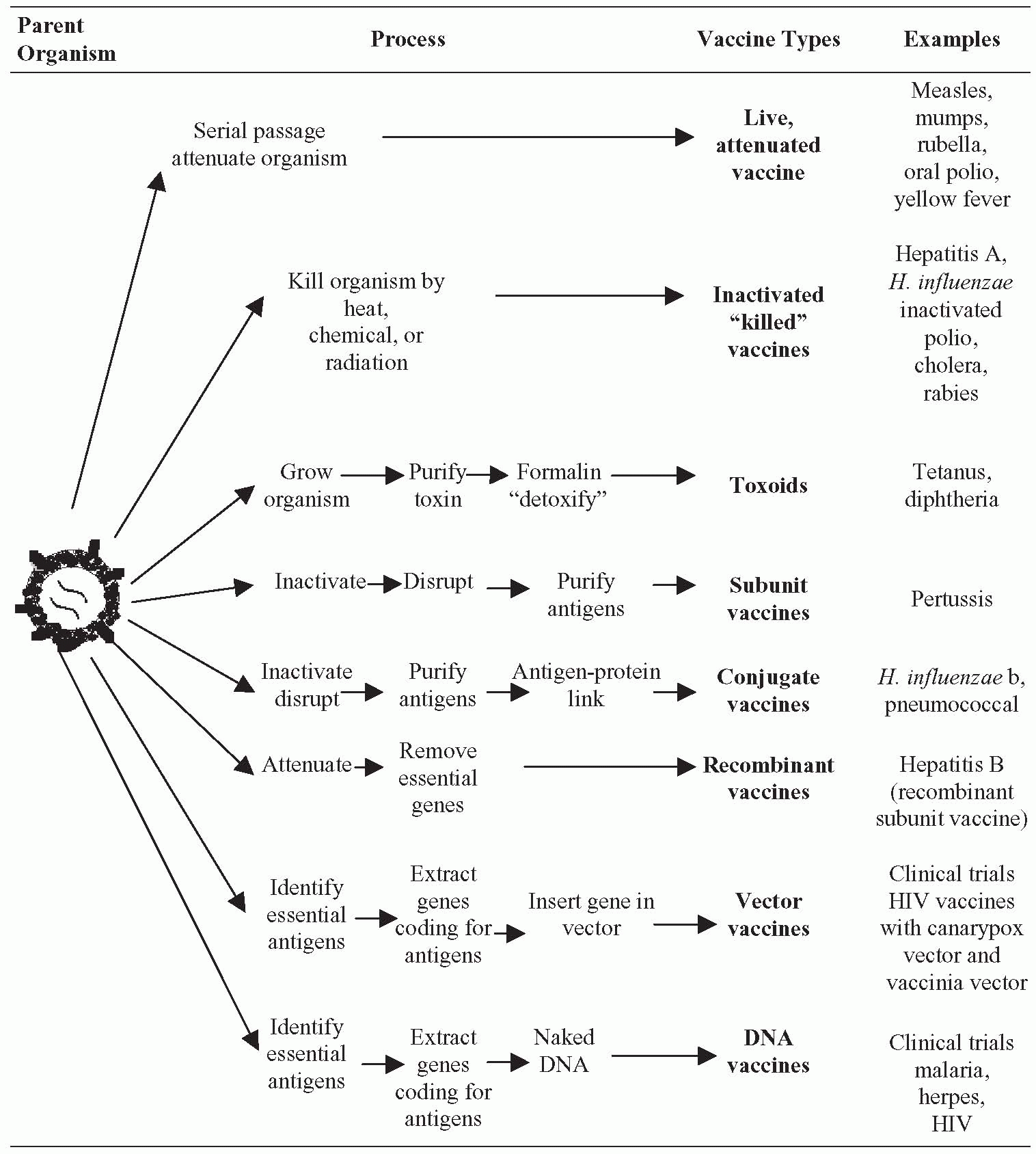
The antigenic agent used in active immunization can be (1) a live organism that has been attenuated (i.e., weakened) or (2) an inactivated form that is either whole or fractionated (e.g., protein or polysaccharide component). A third type of vaccine, recombinant vaccines, is made by genetic manipulation of the organism’s genomic material, and can be either live or inactivated. This section describes characteristics of the various types of vaccines, as well as a newer experimental approach involving vaccination with naked DNA. Exhibit 11-2 depicts how vaccines are made and identifies examples of specific vaccines by type.
Whereas some vaccines are imagined as being able to prevent infection, many others prevent or minimize the consequences of infection. For example, toxoid vaccine prevents tissue damage from bacterial toxins (e.g., tetanus or diphtheria toxin) but does not actually act against the bacteria themselves. Likewise, inactivated poliovirus vaccine does not prevent wild-type poliovirus from multiplying in the intestinal tract, but the immunity induced by this vaccine prevents the virus from causing central nervous system disease.
Exhibit 11-2 Vaccine Manufacturing
The public health burden of cancers caused by viral infection may be considerably reduced through the introduction of preventive or therapeutic vaccines. The inclusion of hepatitis B (HBV) vaccine in several national immunization programs will prevent primary disease as well as—is also hoped—reduce the incidence of liver cancer, although overcoming the barriers to achieving adequate coverage will be necessary. Preventive vaccines have also been licensed for human papillomavirus (HPV) infection. It is estimated that 50% of sexually active adults will have genital HPV at some point in their lives. HPV is highly prevalent among young men in the United States (25%)3 and accounts for approximately 95% of all cervical cancers in women.4
Efforts to harness the specific targeting capacity of the immune system to selectively kill malignant cells has resulted in varying levels of success. Immunization with tumor antigen and stimulation of the immune system has been attempted as one approach. A novel gene therapy approach has reported results from a Phase 1 clinical trial. In this study, researchers used a modified, and crippled, HIV virus to insert genes to target the patient’s leukemia into autologous T cells. These T cells were then returned to the patient. In three out of three patients, significant improvement was subsequently reported; two patients were described as cured of their leukemia. How durable this response will be is unknown at this time, but it is an exciting result that holds great promise.5 Advances in this field are likely to lead to important victories in the war against cancer.6
Live Attenuated Vaccines
Bacteria and viruses are referred to as being attenuated if they have been rendered nonpathogenic. Bacteria can be attenuated through laboratory culture, and viruses through serial passaging in tissue culture or animal hosts. Both bacteria and viruses can be attenuated through genetic manipulation.
The potential role of attenuated organisms in vaccination was identified soon after Jenner’s landmark smallpox vaccination study in 1796. In the 1870s, Louis Pasteur recognized that inoculating a weakened form of chicken cholera protected chickens against challenge with the wild-type virus. Pasteur then developed an attenuated anthrax bacilli vaccine that was first administered to livestock in 1881, and an attenuated live rabies vaccine that was used to immunize two human volunteers in 1885.7 In 1909, the bacille Calmette-Guerin (BCG) tuberculosis vaccine was the first live attenuated bacterial vaccine developed for humans.
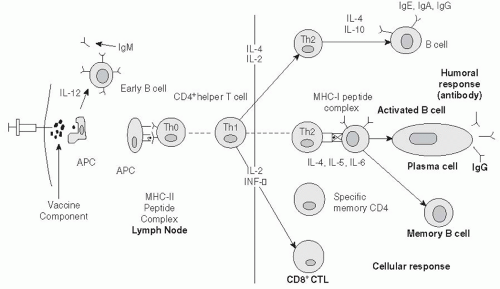
Live attenuated organisms must replicate, or multiply, in the host to induce an adequate immune response. These live vaccines typically generate a stronger immune response than inactivated vaccines, and immunity is considered lifelong due to immunologic memory. Live vaccines have the advantage of inducing both humoral and cell-mediated immunity. In simple terms, humoral immunity refers to antibody—specifically, immunoglobulin (Ig)— production. Antigen recognition by lymphocytes (T cells and B cells) leads to clonal expansion of specific B cells, the generation of memory cells, and production of specific antibodies that are directed against a particular antigen. The primary humoral immune response to a new antigen involves short-term production of IgM antibodies, which is replaced by longer-lasting, higher-affinity IgG antibodies. If the host is later reexposed to the same antigen, a rapid expansion of memory cells results in a secondary immune response involving production of specific IgG but not IgM antibodies. Cell-mediated immunity includes nonspecific first-line responses against invading organisms, such as phagocytes, natural killer cells, and complement as well as antigen-specific responses, such as activation of cytotoxic T lymphocytes (T cells that express CD8+ on their cell surface). These responses may be induced by live attenuated viral vaccines and potentially by naked DNA vaccines. Figure 11-2 depicts humoral and cellular immune response pathways. For a detailed account of the humoral and cell-mediated response to infectious agents, the reader is referred the referenced texts.7, 8, 9 and 10
Another potential advantage of live vaccines is the possibility of horizontal transmission, or indirect vaccination, which refers to the transmission of vaccine virus to other susceptible individuals. Horizontal transmission of vaccine virus has been described for live oral polio vaccine (OPV), for example.12 Indirect vaccination has the significant benefit of enhancing vaccine coverage by exposing unvaccinated persons to the vaccine strain. However, the vaccine strain of polio reverts to the virulent strain in the gut of vaccinated patients over time. This conversion has resulted, on rare occasions, in vaccine-associated paralytic polio (VAPP) among the non-immune contacts of OPV recipients.13 For this reason, horizontal transmission of vaccine strains requires careful monitoring and surveillance for the detection of disease cause by these strains. In countries where polio is no longer endemic, inactivated polio vaccine is recommended to eliminate the risk of VAPP. In the United States, OPV has not been used since 1999.13
Although attenuated vaccine strains may be controlled by immunocompetent persons, they may be poorly controlled by in the bodies of individuals with compromised immune systems (e.g., the elderly, infants, those on immunosuppressive drugs, persons with HIV/AIDS). In these populations, severe adverse events can occur with administration of such live vaccines. All unintended and serious consequences of vaccination are assessed through both clinical trials before approval and through surveillance mechanisms post licensure.
Antibody induction by live attenuated vaccines can sometimes be suppressed by circulating antibodies that cross-react with the attenuated organism. Interference can be caused by antibody produced during concurrent natural infections, immune globulin administered during recent passive immunization, or maternal antibodies. Measles vaccine is particularly sensitive to circulating maternal antibodies, which leads to the complicated measles immunization schedules used with preschool children.14 In rare cases, antibodies induced by one vaccine can inhibit the immune response to another vaccine, a situation that bears watching when several vaccines are administered simultaneously. Previous concerns that administering yellow fever and cholera vaccines simultaneously could reduce the long-term immune response to both have not been borne out;15 however, the Centers for Disease Control and Prevention (CDC) still recommends that these vaccines be administered at least 3 weeks apart. In addition, some antimalarial drugs (e.g., chloroquine) do interfere with live cholera vaccine.16
Immunization programs that incorporate live vaccines need to take appropriate measures to protect the vaccine from environmental conditions (e.g., heat, light). The system of vaccine storage and transport from manufacturer to client is called the cold chain, as constant refrigeration is one of the greatest challenges. Although stabilizing agents (e.g., magnesium chloride) can be used to safeguard the viability of live vaccines, failure to maintain the cold chain can compromise vaccine efficacy. When appropriate, simultaneous administration of several live virus vaccines (e.g., measles, mumps, rubella [MMR]) reduces cost by bundling the cumbersome handling, shipping, and storage requirements of the three vaccines.16
Inactivated Vaccines
In the recent past, inactivated vaccines were either whole viruses or bacteria that were “killed” using heat or chemicals (e.g., formalin). Today, most inactivated vaccines are not based on the whole virus, but rather use only extracted or purified protein or polysaccharide components of an organism.
As early as 1888, it was discovered that the diphtheria bacillus (Corynebacterium diphtheriae) produced a powerful toxin that caused the disease pathology.17 In the early 1900s, chemical inactivation of bacterial toxins led to the first toxoids for diphtheria and tetanus that could be used for vaccination.
Another type of inactivated vaccine is based on polysaccharides that are typically derived from bacterial cell walls (e.g., pneumococcus, meningococcus, Haemophilus influenzae type b [Hib]). Purified polysaccharide-based vaccines are not consistently immunogenic for the elderly, immunocompromised persons, or infants, and are not recommended for children younger than 2 years of age. More successful vaccines have chemically linked, or conjugated, the polysaccharides to a protein carrier that can boost the immune response. This approach has been successfully used to maximize the immune response to Hib. Conjugate Hib vaccine was the first of this type of vaccine licensed for use in humans. Newer conjugate vaccines include the 7-serotype pneumococcal vaccine (PCV7) and the newly licensed 13-serotype pneumococcal vaccine (PCV13) that prevent many invasive Streptococcus pneumoniae infections, which replaced Hib as the most common bacterial cause of meningitis, bacteremia, and pneumonias.18 A fourth quadrivalent conjugate vaccine, MCV4, was licensed in 2005 for the prevention of Neisseria meningitides sepsis, meningitis, and other severe disease caused by organism.19 MCV4 is recommended for children, adolescents, persons living in close quarters such as students in dormitories or military recruits, and persons who have a complement deficiency or are asplenic.20
By definition, inactivated vaccines are not alive; thus they cannot replicate in the host or revert to virulence. These vaccines are not rendered ineffective by circulating antibody and require less stringent handling procedures. Inactivated vaccines are associated with fewer adverse effects, which, when they do occur, are commonly localized to the injection site. Although these properties are favorable, the immune response associated with inactivated vaccines is typically restricted to humoral immunity. Several doses are usually required to boost the specific antibody level, or titer. Immunity produced by inactive vaccines wanes with time, necessitating the administration of booster doses.
In cases where the antigenic component of the organism cannot be easily isolated, whole inactivated viruses or bacteria have formed the basis of vaccine preparations. Because these vaccines include many antigens, they are more likely to be reactogenic, meaning they induce more adverse effects. This problem arose with whole-cell pertussis vaccine, for example—use of the vaccine was associated with febrile seizures and allergic reactions. Newer inactivated acellular pertussis vaccines, which are component vaccines, have been developed and licensed since 1991. These vaccines are associated with fewer side effects and are considered very safe.
Recombinant Vaccines
In the last two decades, attention has focused on genetic manipulation of organisms to generate either live attenuated or inactivated vaccines. Several different approaches have been used.
Hepatitis B vaccine, the first recombinant DNA vaccine, was licensed in 1986. There was substantial interest in developing a new hepatitis B vaccine as an earlier vaccine; while it was highly efficacious, this vaccine was derived from human blood products, and it was later determined that some blood product donors were HIV infected. The vaccine production process was designed to inactivate HBV and, therefore, also inactivated HIV. Although no infections with either virus were ever documented, this near-miss encouraged the production of non-human-based vaccine components.
The recombinant vaccine harnessed the ability of Saccharomyces cerevisiae, yeast cells, to make proteins. The hepatitis B surface antigen (HBsAg) genes were transvected (inserted) into the yeast cell genome. Once the genes were inserted, the yeast cells could be clonally expanded so that large quantities of HBsAg could be produced. This technique allows for high production of antigen without the use of human-derived materials and has been used to generate many new vaccines. For example, Escherichia coli has been used to express lipoprotein from Borrelia burgdorferi, the arbovirus responsible for Lyme disease.21 The first human vaccine for Lyme disease was licensed in 1998.
In recent years, two new recombinant vaccines have been developed to prevent hepatitis E virus (HEV) infection. HEV is an enteric organism that is spread by fecal-contaminated water; it causes widespread outbreaks and sporadic cases of severe fulminant hepatitis. HEV infection has been predominantly identified in developing countries in Asia and Africa. This type of hepatitis has a high mortality rate, especially in infants and pregnant women.22 The new recombinant vaccines induce antibody to a capsid protein (E2) that prevents infection. In two large clinical trials, these vaccines have been shown to be 95% and 100% effective, respectively.23, 24 While neither vaccine has become commercially available, advocates are urgently demanding release of these vaccines for both prevention and outbreak control.25, 26 and 27
Another approach to developing a recombinant vaccine involves deletion or modification of genes that are known to confer pathogenicity. This method has been used to construct an oral typhoid vaccine, among numerous other vaccines. Recently, genetic manipulation of rhesus monkey and human rotavirus genomes enabled the development of vaccines for rotavirus, the major etiologic agent responsible for diarrheal deaths in children. Development of rotavirus vaccines took advantage of the fact that human and animal (i.e., bovine, rhesus) strains of the virus readily underwent reassortment. The resultant multivalent vaccine increases the potential to provide protection against multiple serotypes.28
A third approach to recombinant vaccine development involves insertion of a gene from one organism to another, usually a live virus. The modified virus subsequently acts as a carrier, or vector, that expresses the foreign gene. Using this innovative approach, canarypox virus has been used to express HIV glycoproteins.29 In 2009, a canarypox-based HIV vaccine was the first vaccine to demonstrate a small level of protection from infection. In a Thai trial that began in 2003, researchers tested a vaccine regimen that included a priming dose of a recombinant canarypox vector vaccine (ALVAC-HIV) followed by two booster doses of a recombinant glycoprotein 120-subunit vaccine (AIDSVAX B/E). A modest reduction in the risk of HIV infection (31.2%) was noted among vaccine recipients.30 As the vaccine was effective enough to have an impact, it has raised hopes that a vaccine may someday be developed to control HIV.
Vaccinia virus and adenovirus have been used to express rabies G protein.31, 32 This vaccine vector has been used to immunize wildlife against rabies in a novel program in the southwestern United States.31 Because the vaccine can be administered orally, meat sticks impregnated with vaccine were distributed in an aggressive campaign that used airplane drops as well as ground distribution to surround known cases of rabies. Coupled with an immunization campaign for domestic animals and an education campaign about the purpose and safety of the immunization meat sticks, the campaign was successful in slowing the spread of rabies in Texas.31
DNA Vaccines
DNA vaccines differ from traditional vaccines in that the naked DNA coding for a specific component of a disease-causing organism is injected directly into the body. The delivery system is either a saline solution injected through a hypodermic needle or DNA-coated gold beads propelled into the body using “gene guns.” Although no DNA vaccine is currently licensed, DNA vaccination represents a considerable technological advance that may revolutionize immunization. Developed extensively throughout the 1990s, this approach offers the possibility of safer and cheaper vaccines, even for diseases where traditional vaccines have achieved only limited success. DNA vaccines are currently under development for malaria, West Nile virus, tuberculosis, and HIV, among other infections.
There are several potential advantages associated with DNA vaccines. First, the actual production of the immunizing protein takes place in the cells of the vaccinated host. This approach theoretically eliminates the risk of the vaccine causing the infection it is intended to prevent, which is a concern with traditional live attenuated vaccines. Second, like live vaccines, DNA vaccines have the ability to elicit a wide range of humoral and cell-mediated immune responses that might potentially have a long-term duration. Third, DNA vaccines are very stable and can be stored under a vast array of conditions, eliminating the need for a cold chain. For this reason, they may be particularly suitable for use in developing countries. Finally, DNA vaccines may lend themselves to generic production methods that will simplify and standardize vaccine production.
An important shortcoming of DNA vaccines is that they are limited to developing immune responses against protein components. As a consequence, they cannot substitute for traditional polysaccharide-based vaccines (e.g., pneumococcal vaccine). These vaccines also pose novel safety concerns. For example, they may cause long-term immunologic stimulation at the injection site, leading to chronic inflammation. DNA from the vaccine might also become incorporated into host chromosomes and could be oncogenic if their presence turned on oncogenes or turned off tumor suppressor genes. Clearly, the safety and efficacy of DNA vaccines need to be carefully evaluated to ensure that the potential risks of these new vaccines are well understood.
Novel Vaccines
Novel approaches in vaccine development include the identification of new targets, new adjuvants, and new vaccine delivery methods, as well as the development of new vaccine types and combination vaccines. Both disease severity and disease burden remain important criteria for selecting an organism for vaccine development. Notable infections influencing vaccine development include HIV, tuberculosis, and malaria—a virus, bacterium, and parasite, respectively. The Jordan Report lists many infectious agents for which vaccines are in the pipeline.33 Viral vaccines include those focused on the hepatitis C virus and herpesvirus (HSV-1 and HSV-2). In addition to HSV and HPV vaccines, other vaccines are in development to prevent sexually transmitted infections including gonorrhea, syphilis, and chlamydia. Along with the two licensed rotavirus vaccines, vaccines to prevent Escherichia coli, Salmonella typhi, and Shigella species are among the many vaccines being developed to prevent the diarrheal diseases that account for 4.0% of all deaths and 5.7% of the disease burden worldwide.34
Enhancing the specific and protective immune response to a vaccine remains a significant challenge. Adjuvants, such as aluminum salt (alum), have been used since the 1920s to increase immunogenicity. The mechanism of action of these older adjuvants was to inhibit clearance of an antigen from the site of injection, thereby allowing better recognition of the antigen by antigen-presenting cells (APCs). Newer adjuvants that improve the delivery of antigens to APCs in the lymphoid tissue have been developed. For example, particulate adjuvants, such as liposomes and microspheres, protect antigens from being destroyed in the stomach and present antigens to macrophages in the gut to enhance mucosal immunity. Other adjuvants are being developed to direct the immune response toward either a cellular-mediated (TH1) or an antibody (TH2) immune response. These adjuvants include cytokines, such as interleukin and interferon-gamma, and che-mokines.35, 36 and 37 Vaccines that target intracellular infections, such as HIV and Mycobacterium tuberculosis, or parasites, such as Plasmodium spp. (malaria), need to produce a strong TH1 response. Strong antibody (TH2) responses are the best defense for extracellular bacterial infections (e.g., Haemophilus influenzae type b) and toxin-mediated diseases (Bordetella pertussis).35, 36 and 37 Unfortunately, the incorporation of an adjuvant in a vaccine’s formulation may increase the risk of an adverse reaction; therefore, separate animal studies and safety studies are needed to evaluate the adjuvant effects. For more in-depth discussion of adjuvants, the reader is referred to the article by Vogel and Alving in the 2002 Jordan Report.36
The way vaccines are administered is also changing. Combination vaccines have been developed to reduce the number of overall injections. The measles, mumps, and rubella (MMR) vaccine, the diphtheria-tetanus-acellular pertussis vaccine (DTaP), and the Haemophilus influenzae type b and hepatitis B vaccine (Hib-HepB) are a few examples of the many combination vaccines currently being administered. The newly licensed live attenuated influenza vaccine administered intranasally aims to produce both local (mucosal) and systemic immune responses. Likewise, orally administered vaccines (e.g., polio and cholera vaccines) are advantageous in that they produce mucosal immunity.
In the foreseeable future, edible vaccines may be used to administer vaccines more widely, safely, and cheaply. Transgenic plants such as potatoes, tomatoes, and bananas are being developed such that the plant gene will encode for the targeted vaccine antigens.34, 35 Among the edible vaccines in the development pipeline are vaccines that target measles, E. coli, Norwalk virus, and hepatitis B. It is hoped that such plants can be developed for the delivery of multivalent vaccines for protection against a broad range of diseases.
Lastly, transcutaneous immunization systems, including skin patches and gene guns, aim to deliver vaccine antigen and adjuvant across the epidermis to Langerhans cells, a specific class of dendritic APC.35, 37
The development of DNA and other gene-based vaccines holds promise that new mechanisms to deliver antigen-encoding genomes to the host will result in novel vaccine types: vector vaccines, such as simple plasmids or more complex modified viral vaccines (e.g., Vaccinia or adenovirus) or bacterial vectors.37 The newly licensed HPV vaccines include a piece of the HPV genome enclosed in a non-enveloped capsid, which creates a virus-like-particle (VLP).38 VLPs are being developed for other viral infections such as avian influenza and HIV.39
IMMUNIZATION SCHEDULES
The goal of an effective immunization program is to vaccinate a high proportion of susceptible persons early in life (i.e., before they are potentially exposed to the infectious agent). In the United States, infants and children are immunized against hepatitis B, diphtheria, tetanus, pertussis, Hib, polio, measles, mumps, rubella, and varicella virus (Exhibit 11-3). Alternative immunization schedules are available from other sources for children who have missed primary immunization series or who were inadequately immunized.28, 29
Immunization schedules40 differ from country to country, depending on the burden of disease in the population, the availability of an efficacious and effective vaccine, economic factors, and the level of priority that is placed on vaccine preventable diseases. Prevention of hepatitis B infection has become a worldwide priority; therefore, an HBV vaccine has been added to the World Health Organization’s (WHO) Expanded Program on Immunization recommendations. The routine vaccinations recommended by WHO are diphtheria, tetanus, and pertussis vaccine; oral polio vaccine; and measles, mumps, and rubella vaccine. In addition, WHO recommends vaccination against tuberculosis (i.e., BCG) and yellow fever in countries where these diseases are endemic.
Target Populations
Vaccine programs must identify individuals before exposure to natural infection and must boost vaccination rates among these populations before immunity wanes and is no longer at protective levels. A failure to maintain vaccine levels has resulted in outbreaks of disease among school-aged children. Assessment of adolescents at routine healthcare visits is warranted to ensure completion of primary vaccine series for newer vaccines (e.g., varicella, hepatitis B vaccine) and provide boosters for MMR if necessary.41 In 2005, two new vaccines were licensed and recommended for adolescents: a conjugate meningococcal vaccine and a DTaP vaccine.
In 2006 and 2009, two preventive vaccines were licensed for human papillomavirus (HPV). These vaccines were immediately recommended for adolescents females as young as 9 years, with catch-up immunization through age 26 years. Gardasil, a HPV vaccine currently licensed for use in the United States, protects against HPV types 6, 11, 16, and 18. HPV vaccination provides nearly 100% protection against persistent infections, genital warts, and precancerous lesions of the cervix caused by HPV types 6, 11, 16, and 18,42 and data indicate that the vaccine may partially protect against 10 additional HPV types that cause up to 90% of cancers.42 On a national level, U.S. HPV immunization rates lag far behind the Healthy People 2010 goals of 90% coverage for adolescent females. Public perception, parental health beliefs, and naïveté of adolescents’ sexual behavior are barriers to HPV immunization. To further prevent the spread of HPV, in 2010 these vaccines were recommended for all adolescents, including young adult males. If developed, other vaccines to prevent sexually transmitted infections, including herpes simplex virus type 2 (HSV-2) and the human immunodeficiency virus (HIV), will likely be offered to adolescents in the future to assure vaccination prior to exposure to these viruses.
Exhibit 11-3 Recommended Childhood and Adolescent Immunizations Schedule, United States 2012
Vaceine ▼
Age▶
Birth
1 month
2 months
4 months
6 months
9 months
12 months
15 months
18 months
19-23 months
2-3 years
4-6 years
Hepatitis B
Hep B
Hep B
Hep B
Rotavirus
RV
RV
RV
Diptheria, tetanus, pertusis
DTaP
DTaP
DTaP
*
DTaP
DTaP
Haemophilusinfluenzae type b
Hib
Hib
Hib
Hib
Pneumococcal
PCV
PCV
PCV
PCV
PPSV
Inactivated poliovirus
IPV
IPV
IPV
Influenza
Influenza (annually)
Measles, mumps, rubella
MMR
*
MMR
Varicella
Varicella
*
Varicella
Hepatitis A
Dose 1
Hep A series
Meningococcal
MCV4
Range for all children
Range certain high-risk children
Range all children and for certain high risk groups
* The schedule has extensive footnotes that clarify the spacing between vaccination doses, and it generally allows a slightly earlier administration of a vaccine if the previous doses were given at the earliest possible time. Further adjustments are made for children at higher risk of measles.
This schedule includes the recommendations in effect as of December 23, 2011. Any dose not administered at the recommended age should be administered at a subsequent visit, when indicated and feasible. The use of a combination vaccine generally is preferred over separate injections of its equivalent component vaccines. Vaccination providers should consult the relevant Advisory Committee on Immunization Practices (ACIP) statement for detailed recommendations, available online at http://www.cdc.gov/vaccines/pubs/acip-list.htm. Clinically significant adverse events that follow vaccination should be reported to the Vaccine Adverse Event Reporting System (VAERS) online.
Modified from the Centers for Disease Control and Prevention (2012). Recommended immunization schedule for persons aged 0 through 6 years—United States, 2012. http://www.cdc.gov/vaccines/schedules/downloads/child/0-6yrs-schedule-pr.pdf. Updated May 31, 2012. Accessed June 25, 2012.
Adult vaccination is an important part of preventive medical care. Routine adult vaccines include pneumococcal vaccine, influenza, and tetanus toxoid. A newer varicella vaccine, Zostavax, was licensed in 2006 for use in people age 60 and older to prevent shingles. MMR, hepatitis B, and hepatitis A are recommended for adults at higher risk. The U.S. Public Health Service and the CDC provide immunization recommendations for international travelers, depending on the endemic diseases in the destination country (e.g., MMR, hepatitis A and B, yellow fever, meningococcal, typhoid, polio, rabies, plague, and Japanese encephalitis).43 Hib, pneumococcal, and meningococcal vaccinations are recommended for immunosuppressed persons who are at high risk of invasive bacterial infections. However, vaccine-induced immune responses may not be optimal in immune-suppressed people, and some individuals may remain susceptible to the infections targeted by the vaccines.
Conditions that Contraindicate Vaccination
Immunization schedules are modified when an individual has a contraindication to a particular vaccine (Exhibit 11-4). Mild illnesses (e.g., low-grade fever, upper respiratory infection, otitis media, and mild diarrhea) or breastfeeding are not contraindications for immunization. Previous or suspected anaphylactic reaction to a vaccine component is the strictest contraindication to immunization. When a concurrent moderate or severe illness may be exacerbated by a vaccine-induced immune response, immunization can be delayed. Contraindications are specific to live attenuated vaccines, which pose a threat to immunosuppressed individuals or to fetuses. Because measles can be a severe illness in an HIV-infected person, MMR immunization is recommended for HIV-infected persons before they become severely immunocompromised. Among blood-product recipients, circulating antibody present in transfused blood components can interfere with the replication of live vaccine virus. Therefore, it is recommended that MMR and varicella vaccinations be postponed for a period following blood or blood product transfusions.
Exhibit 11-4 Contradictions for Vaccination
Severe allergy to any vaccine component
Severe illness
Immunosuppression (live vaccines only)
HIV infection (live virus vaccines except measles)
Pregnancy (especially live vaccines)
Encephalopathy
Recent receipt of blood products (MMR and varicella)
VACCINE DEVELOPMENT
Vaccine innovation includes identification and characterization of antigens that induce neutralizing antibody or humoral response, identification of genetic clones that produce these antigens, vaccine biochemical formulation, numerous animal studies, and extensive manufacturing innovation to mass-produce vaccine. Vaccine science, innovation, and manufacturing are critical components in the development of safe and efficacious vaccines for all national immunization programs.
Licensure of any new vaccine requires that efficacy be demonstrated from preclinical studies. In the United States, the vaccine manufacturer begins this process upon filing an investigational new drug (IND) application with the U.S. Food and Drug Administration (FDA). All information concerning vaccine formulation, vaccine manufacturing, stability and sterility testing, and results of animal testing is submitted to the FDA. The FDA approves the implementation of human studies only if the new vaccine demonstrates preliminary potency, safety, and effectiveness in animal studies. The following section outlines the hierarchical process of preclinical and clinical research. At each point, the decision to progress to the next phase is based on promising results from the previous set of studies.
Preclinical Studies
Animal testing is used to develop assays that assess the humoral and cellular immune response to candidate vaccines. Through a series of studies, appropriate animal models are used to determine the dose-response relationship, to identify the optimal routes of administration, and to specify the dosing schedule necessary to achieve the maximum beneficial dose (i.e., the dose that maximizes the protective immune response and minimizes serious adverse events). Animal studies represent the first step in evaluating vaccine safety. A list of vaccine-induced toxicities is established, which may include severe systemic effects and organ systems damage, as well as the unlikely potential of a vaccine to be carcinogenic or teratogenic. Provided that its potential benefit is deemed to outweigh its potential harm, the product then proceeds to human studies.
Phase 1: Dose Finding and Safety
Following FDA review and approval by an institutional review board (IRB), early vaccine studies in humans are conducted to evaluate vaccine dose and safety and to assess whether the vaccine is biologically active. Specific toxicities (e.g., local and systemic reactions and hematological abnormalities) are evaluated in both Phase 1 and Phase 2 safety and immunogenicity studies. Rules for stopping an immunization series are established from the outset and are modified as more data are collected.
Most preventive vaccine clinical trials begin with trials in healthy, adult volunteers. Childhood vaccines are first tested in healthy adults and older children, prior to testing in infants. For some vaccines (e.g., HIV vaccines), initial clinical trials may be conducted in previously infected persons and subsequently among uninfected healthy adults. Adult studies typically begin with a single fixed dose of vaccine in a small number of volunteers (e.g., 5-10 subjects). Post-inoculation serologic assays measure the level and duration of the immune response. Adverse events are carefully enumerated and graded for severity, duration, and the relationship to vaccination. Small sequential studies may be conducted whereby the vaccine dose is increased until a beneficial dose is established. Additional Phase 1 or Phase 1/2 safety and immunogenicity studies are performed in children and infants to fine-tune the dose, define the vaccine schedule, and continue monitoring immune response and vaccine safety in these age groups.
Phase 2: Safety and Immunogenicity Trials
In Phase 2 studies, safety, benefit, and evidence of efficacy are the primary endpoints. Safety and immunogenicity endpoints are predefined based on preclinical and Phase 1 studies. The vaccine is tested in healthy persons representing the population for which the vaccine is indicated. In this phase of testing, the sample size needs to be sufficiently large to measure the vaccine’s benefit (i.e., evidence of efficacy) without compromising the ability to estimate rates of adverse events. Studies enrolling 50-100 persons can measure adverse events at a rate of 10 in 100 doses and estimate the beneficial effect that occurs in 10% or more of the population.
Only gold members can continue reading. Log In or Register to continue