(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
Tumors involving the ribs of the lower chest wall, the hemidiaphragm (or a portion of it), and the upper abdominal wall pose special problems in reconstruction. In the case depicted, a large sarcoma on the left side of the lower chest and upper abdominal wall is protruding and is easily palpable. Assuming that the tumor is roughly spherical, the direction of the incision is preferably oblique, following the direction of the lower ribs (Fig. 20.1). The usual position of the patient is a lateral one, with the affected side up. The previous biopsy incision is included in an elliptical incision. Skin flaps then are raised several centimeters beyond the palpable extent of the tumor (Fig. 20.2). The fascia covering the muscles is incised around the tumor (Fig. 20.3).
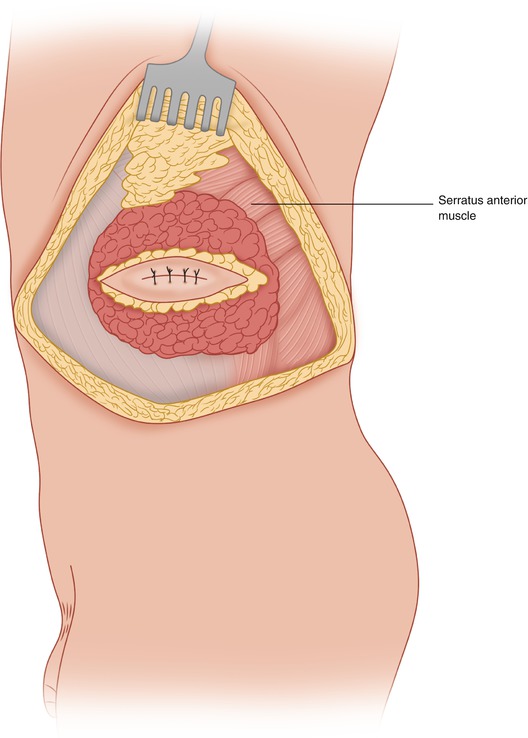
Fig. 20.1
An elliptical incision is made around the previous biopsy site
Fig. 20.2
Flaps are developed beyond the palpable extent of the tumor
Fig. 20.3
The deep fascia is incised and the underlying muscles are exposed at a sufficient distance from the tumor
It is preferable to divide the anterolateral abdominal wall muscles and first enter the abdominal cavity (Fig. 20.4). The abdominal wall is more dispensable than the chest wall, as the integrity of the chest wall is essential for adequate respiration and expansion of the lungs. If extensive metastases of the tumor are found within the abdominal cavity, the operation may be rendered inadvisable and the more traumatic entry into the thoracic cavity can be avoided. However, occasionally, a palliative resection of the tumor may be of value for the patient.
Fig. 20.4
The abdominal cavity is entered first to evaluate the extent of the tumor. The tumor involving the left diaphragm is retracted with a Deaver retractor over a laparotomy pad
Following assessment of the peritoneal cavity and lysis of any adhesions in the area to be resected, the incision of the abdominal muscles is completed around the palpable extent of the tumor, maintaining the appropriate margin. The incision is continued to the costal margin, both anteriorly and posteriorly. Then an incision through the muscle layers—the external oblique over the lower ribs and the serratus anterior higher—is carried around the palpable tumor to the surface of the ribs. The costal margin is divided anterior and posterior to the tumor mass, removing a 3-cm segment of the ribs to allow entry into the pleural space and digital appraisal of the parietal pleura and of possible infiltration by the chest wall tumor, which may protrude into the pleural cavity and involve the lower lung. Palpation of the chest wall from the inside as well as from the external surface allows precise assessment of the chest wall involvement and of the number of ribs that must be resected (Fig. 20.5). The intercostal vessels and nerves are ligated and divided. The decrease in the pleural space resulting from removal of the ribs depends, of course, not only on the number of ribs involved but also on the length of the involved segments. Only the number and portion of the ribs considered necessary for adequate resection of the tumor should be removed.