(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
The popliteal space is bound superiorly by the hamstring muscles and inferiorly by the two heads of the gastrocnemius. The popliteal nodes, about six in number, are located in the space behind the knee joint. Apparently, this group drains only a small area of the skin of the posterior calf, and it rarely becomes involved by metastatic malignant neoplasm of the skin. A positive sentinel node in this area, or palpably involved nodes, may require popliteal node dissection. In these patients, the inguinal nodes also may be involved by metastatic disease, and in-transit lesions may be present. Even then, however, resection of the involved tissues may be indicated, if there is no evidence of distant hematogenous dissemination that cannot be surgically resected. The vast majority of these patients do relapse unless there is evidence of low biologic aggressiveness of the melanoma as in patients with a long disease-free interval between the diagnosis of the primary lesion and a regional recurrence. For patients with multiple in-transit lesions, the technique of isolation hyperthermic perfusion may be preferable to control the disease in the lower extremity.
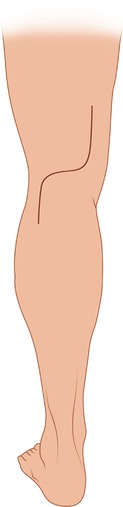
With the patient in prone position and the knee slightly flexed with a narrow pillow under the ankles, an S-shaped incision may be used, with a vertical portion along the edge of the biceps femoris, a transverse portion along the popliteal crease, and another vertical portion along the tendons of the medial hamstrings. A reverse incision—that is, one starting proximally along the medial hamstring muscles, followed by a transverse portion in the popliteal crease and a vertical portion along the distal end of the biceps femoris—may also be used (Fig. 50.1). The lateral flap may be raised, initially about 3–4 mm thick, but as one develops the flap and proceeds toward its base, it can be made thicker medial to the palpable edge of the biceps. The common peroneal nerve can be seen through the deep fascia and dissected free (Fig. 50.2). Scalpel dissection with the appropriate amount of tension in the tissues is the safest technique to avoid nerve injury. The vertical portion of the incision above the level of the popliteal crease is extended proximally, tracing the common peroneal nerve until the point of bifurcation of the sciatic nerve is identified. One then can recognize and dissect the tibial nerve (Fig. 50.3). The medial flap is also developed, aiming toward the edge of the medial hamstrings. Below the popliteal crease, one exposes the medial and lateral heads of the gastrocnemius muscle. The two branches of the sciatic nerve (i.e., the common peroneal and tibial nerves) are surrounded by vessel loops and dissected free within the popliteal space (Fig. 50.4). The lateral sural cutaneous nerve, arising from the common peroneal nerve, and the medial sural cutaneous nerve, arising from the tibial nerve, can be dissected free if they are not involved by tumor. These two nerves join at the level of the midcalf to form the sural nerve, sensory to the posterolateral aspect of the leg’s distal third and the lateral side of the foot and little toe. The sural nerve courses near the small saphenous vein.