(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
In cancer of the gastroesophageal junction or thoracic esophagus, the use of a gastric tube may be convenient in replacing the removed esophagus with an esophagogastric anastomosis if a sufficient length of stomach can be procured after cancer resection. When the stomach is not available, however, a colon bypass may be used if prior colonoscopic evaluation shows no evidence of intrinsic or extrinsic lesions in the wall of the colon. At the time of the operation, the colon is explored carefully to rule out the presence of any lesions that would compromise its suitability as bypass.
The peritoneal attachment (Toldt’s line) of the right colon is incised and the peritoneum continues to be incised around the cecum and distal ileum (Fig. 30.1). The hepatic flexure of the colon is released, exposing the second and third portions of the duodenum, and the gastrocolic ligament is divided. The lesser sac will likely be open from the procedure of esophagogastrectomy. The right mesocolon is separated from the retroperitoneal tissues. Parts of the anterior surface of the inferior vena cava (IVC) are exposed where the precaval adipose tissue is relatively deficient, and the right gonadal vein is often visualized as it enters the IVC at a level just below the third portion of the duodenum. The right ureter is sufficiently exposed to trace its course to the bifurcation of the right common iliac artery and the wall of the lesser pelvis, as needed.
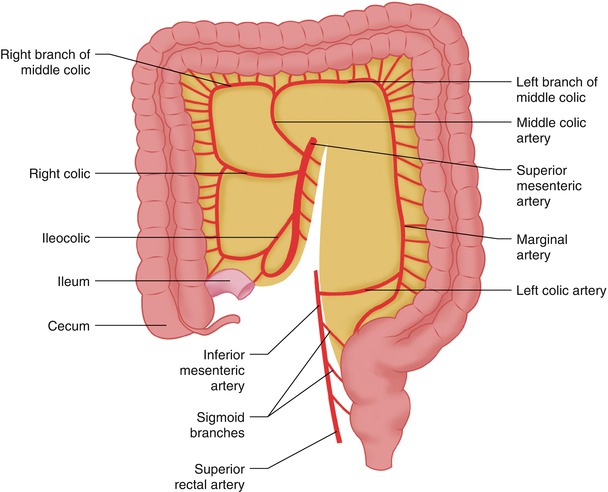
Fig. 30.1
The peritoneum is incised around the right colon. Typical blood supply to the right colon
The mobility of the right colon and of the small bowel loops may be aided by incising the peritoneum continuously from below the distal ileum to the ligament of Treitz (Fig. 30.2). Appendectomy is performed.
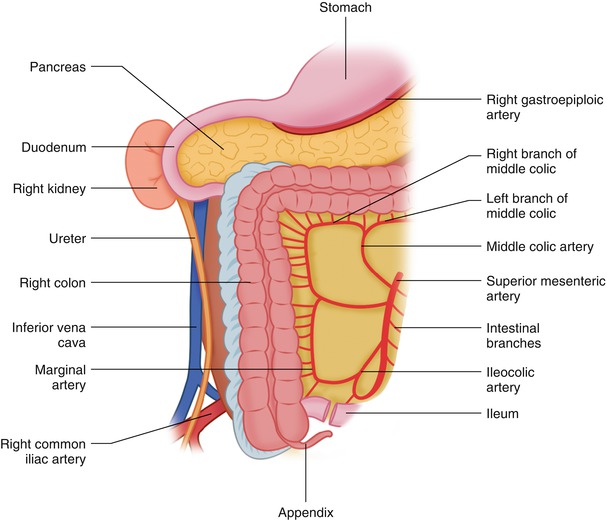
Fig. 30.2
The right colon is further mobilized by continuing the peritoneal incision around the terminal ileum and the base of the mesentery to the ligament of Treitz. The hepatocolic ligament is incised, and the site of the division of terminal ileum is indicated
Some surgeons prefer to leave the appendix in its place until the proximal end of the right colon has been delivered to the neck, using it for traction by gently pulling the cecum through the thoracic inlet into the lower neck. The colon interposition should be guided behind the antrum of the stomach in posterior mediastinum and to the neck, if the in situ esophageal position is available. This is the shortest route to the neck, followed by the substernal location, and finally, the antesternal (subcutaneous) location.
By stretching the right colon and mesocolon to a position outside the abdomen, one can see, by transillumination of the thin layer of peritoneum covering the mesocolon, the branches supplying the right colon (i.e. the ileocolic, the right colic, the right branch of the middle colic, and their connections through the marginal artery).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


