(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
The muscles of the leg are covered by a strong, deep fascia, and strong septa separate them into four main compartments: anterior, lateral, superficial posterior, and deep posterior. The anterior and posterior intermuscular septa to the investing fascia arise from the anterior and posterior borders of the fibula, whereas the transverse intermuscular septum between the posterior border of the fibula and the medial border of the tibia in the posterior aspect of the leg separates the superficial posterior component from the deep posterior compartment.
The Anterior Compartment
The anterior compartment of the leg is concerned with the dorsiflexion of the foot (tibialis anterior and peroneus tertius muscles), of the great toe (extensor hallucis longus), and of the other four toes (extensor digitorum longus). In surgery for anterior compartment sarcomas, the aim is to preserve at least one of the four muscles in the anterior compartment with intact nerve supply so as not to lose completely the capacity for dorsiflexion of the foot and therefore to avoid foot drop. It is obvious that one cannot obtain very wide margins, but if one can obtain margins of 1–2 cm around the tumor, with margins of 5 cm or more in some areas (e.g., in the longitudinal direction), there may be a good chance for local control. These patients with sarcomas in the distal part of the extremity are treated with a combination of modalities more often than those with sarcomas in other areas because of the inability to obtain truly adequate margins.
In anterior compartment sarcomas, a longitudinal incision is made over the most prominent part of the tumor to obtain an open biopsy (Fig. 51.1). More often, a needle core biopsy is taken. After histologic confirmation, a longitudinal elliptical incision is made and flaps are developed (Fig. 51.2). In the case illustrated, the tibialis anterior and extensor digitorum longus were resected, but it was possible to preserve the deep peroneal nerve, anterior tibial vessels, and extensor hallucis longus (Fig. 51.3). The origin of the peroneus longus at the head of the fibula was incised to expose the common peroneal nerve and its bifurcation into deep and superficial nerves. If necessary, all the muscles of the anterior compartment may be sacrificed in preference to performing an amputation. The resulting foot drop can be dealt with by using an ankle brace or later ankle arthrodesis.
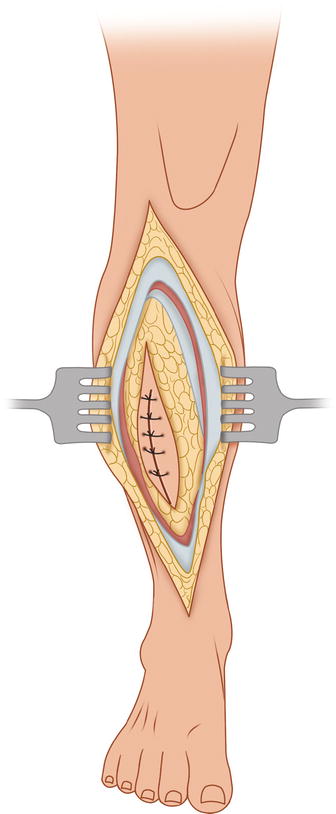
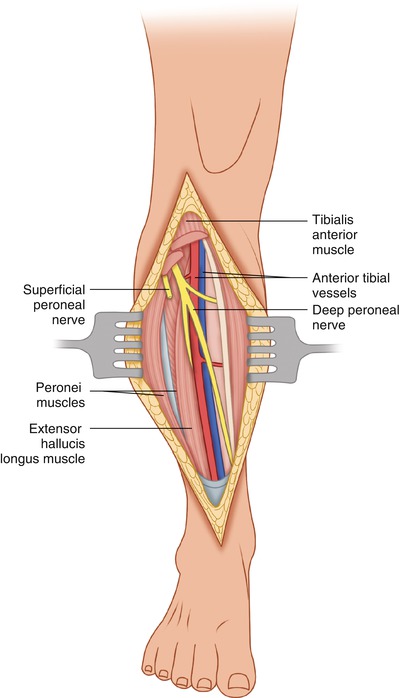
Fig. 51.1
A longitudinal incision is made over the location of the tumor to provide tissue for histologic confirmation
Fig. 51.2
The definitive incision is an elliptical incision around any previous biopsy site, with flaps developed medially as well as laterally
Fig. 51.3
In the case presented, the tumor was resected en bloc with the tibialis anterior and extensor digitorum longus. It was possible to preserve the deep peroneal nerve, anterior tibial vessels, and the extensor hallucis longus muscle
Tumors extending from the anterior compartment over the medial surface of the tibia, or tumors arising in the subcutaneous tissue over the medial aspect of the tibia present difficulties. Resection of these tumors may require resection of the overlying skin if it is too close to tumor, along with removal of the periosteum and sometimes part of the cortex of the tibia in order to obtain a clear margin. One is then left with a very wide wound with bone exposed, so a rotation flap is needed. In such cases, a flap may be obtained by mobilizing the medial head of the gastrocnemius off the lateral head and dividing the muscle distally at the point where the muscle belly becomes tendinous. The distal part of the belly of the medial head of the gastrocnemius is rotated anteriorly to cover a proximal defect in the anterior aspect of the tibia where the bone is exposed. Each head of the gastrocnemius is supplied by a separate arterial branch from the popliteal artery. The soleus muscle can be mobilized to cover defects in the middle portion of the tibia by simply separating the soleus from the undersurface of the gastrocnemius and suturing its medial edge to the tibialis anterior. A skin graft then may be applied over the muscles covering the tibia.
The Lateral Compartment
The lateral compartment of the leg consists of the peroneus longus (arising from the upper two thirds of the dorsal surface of the fibula), the head of the fibula, and the adjacent lateral condyle of the tibia. The peroneus brevis arises from the lower two thirds of the lateral surface of the fibula. The tendons of these muscles course behind the lateral malleolus. The tendon for the peroneus brevis, located anterior to that of the peroneus longus behind the lateral malleolus, inserts in the tubercle of the base of the fifth metatarsal bone. The tendon of the longus, located behind the tendon of the brevis at the level of the lateral malleolus, crosses the sole of the foot to insert in the medial cuneiform bone and the base of the first metatarsal bone. These muscles tend to evert the foot and to pull the leg laterally.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


