(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
For tumors of the pelvis, a midline incision is commonly used, starting from above the umbilicus and continuing around the umbilicus down to the pubic symphysis. The incision is deepened through the subcutaneous fat, and the linea alba is incised on the entire length of the incision to the pubic symphysis. The linea alba is found exactly at the midline more easily close to the umbilicus. The peritoneum also is incised, but this can be done only for the upper portions of the incision, starting from the superior end and then around the umbilicus down to the junction of the middle and lower third of the infraumbilical portion of the midline incision. The reason for stopping the incision at this point is because the peritoneum at that level is splayed around the urinary bladder, so it cannot be divided straight all the way to the pubic symphysis.
Following exploration of the abdomen through the upper part of the incision, however, if one decides to go ahead with resection of the pelvic tumor, then the peritoneum can be incised around the bladder on both the right and left sides. Extending this incision in the peritoneum all the way to the obturator foramen bilaterally allows the abdominal incision to be more extensively retracted. Even so, the attachment of the rectus abdominis to the pubic crest from the pubic symphysis to the pubic tubercle does not permit exposure of the obturator area or the distal portions of the external iliac vein and artery. If the tumor extends bilaterally to the obturator foramina, then the lower end of the midline incision from the pubic symphysis is extended transversely to the pubic tubercle on both sides (Fig. 39.1), and the anterior rectus sheath and rectus abdominis muscle are divided bilaterally a few millimeters above the attachment to the pubic crest (T incision, Fig. 39.2). This incision allows improved exposure, which facilitates the surgical maneuvers and the resection of tumors that otherwise could be called unresectable (Fig. 39.3). If the tumor extends mostly on one side toward the obturator foramen or the distal portion of the external iliac vessels, the incision can be simplified by extending it from the midline at the pubic symphysis along the pubic crest, to the pubic tubercle on the side of involvement only (L incision). The skin, subcutaneous fat, and anterior rectus abdominis sheath and muscle are divided a few millimeters from the pubic crest. The lateral extension of the midline incision, from the pubic symphysis to the pubic tubercle, is completed when required by the needs of exposure by continuing the division of the anterior rectus sheath (and rectus abdominis to its lateral edge) around the pubic tubercle, interrupting thus the medial attachment of the inguinal ligament. This allows exposure in continuity of the proximal part of the femoral vein, into the femoral canal, to the external iliac vein.
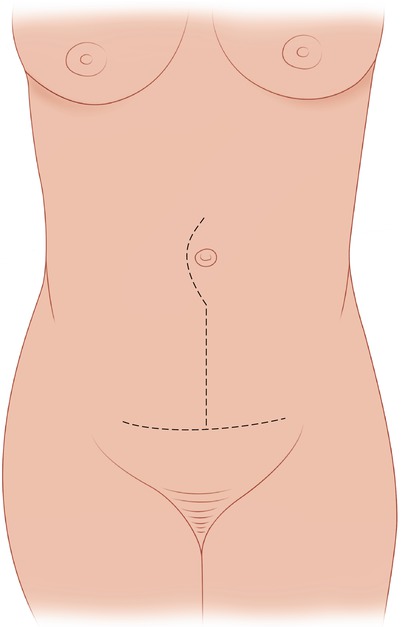
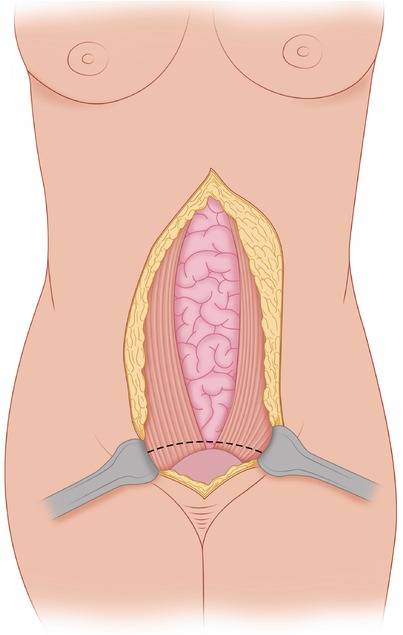
Fig. 39.1
Outline of the skin incision
Fig. 39.2
The linea alba is incised to the pubic symphysis. The lower part of the anterior rectus sheath is exposed bilaterally
Fig. 39.3
The anterior rectus sheath and the underlying rectus abdominis are divided bilaterally to the pubic tubercle a few millimeters above the attachment to the pubic crest, allowing exposure to the obturator foramen and inner side of the inguinal ligament, bilaterally
Closure of the L or T incision is simple. The lower midline abdominal component is closed in routine fashion. The lateral or bilateral extension is closed with interrupted, heavy 0, or 1-0 figure-of-eight sutures between the anterior rectus sheath and muscle and the pubic crest (a 0.5-cm edge of rectus abdominis sheath has been left along the crest for that purpose). If there is tension in bringing together the edges of the horizontal (lateral) extension, this portion of the closure can be reinforced with a 3 cm–wide strip of mesh. Following are examples of the use of these incisions.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


