(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
Scapulectomy is performed when tumors arise in the scapula or when tumors in the soft tissue surrounding the scapula invade the bone. A subtotal scapulectomy is preferable if it is consistent with oncologic principles of obtaining an adequate margin around the tumor. The subtotal scapulectomy involves removal of nearly the whole scapula except for a small part adjacent to the glenoid. Leaving this part in place preserves the glenohumeral joint [1].
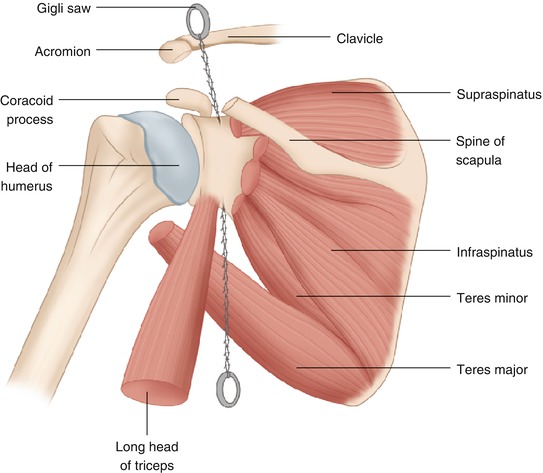
For both subtotal and total scapulectomy, the whole procedure can be done through a posterior approach, with the patient in a lateral position, which actually facilitates the exposure of the brachial plexus and vessels so they can be safely preserved. An oblique incision is used, beginning at a point inferior and medial to the inferior angle of the scapula and extending obliquely cephalad and laterally to the acromion. The medial flap is developed by dissecting on top of the fascia covering the underlying muscles. If it is safe at any time to enter a deeper plane and thus provide one or more of the adjacent muscles to supply the flap, doing so will tend to create more favorable circumstances for viability of the flap. The trapezius muscle is incised from the lateral end of the incision, dividing it off its insertion to the spine of the scapula and the acromion at a sufficient distance from the tumor. The division of this muscle is carried around the superior angle of the scapula and then down alongside the vertebral border of the scapula to well below its inferior angle (Fig. 15.1), The levator scapulae is divided, followed in sequence by the rhomboid minor, rhomboid major, and the portion of the latissimus dorsi over the inferior angle of the scapula. This frees the medial border of the scapula (Fig. 15.2). The lateral flap is also developed inferiorly, exposing the latissimus dorsi and then the fascia covering the teres major, teres minor, and infraspinatus muscles. After division of the deltoid muscle fibers off the spine of the scapula all the way to the acromion process, the teres major fascia and that of the teres minor are exposed and incised. The teres major muscle is divided, and then the teres minor and the infraspinatus tendon, at the level of the neck of the scapula (Fig. 15.3).
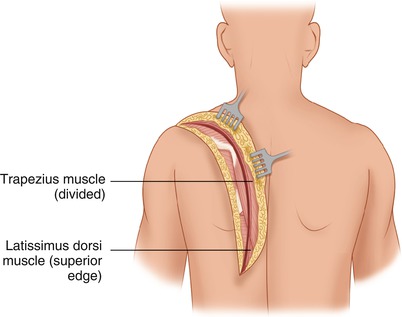
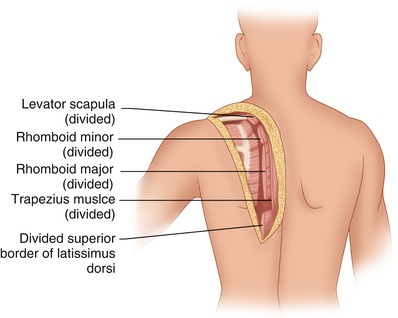
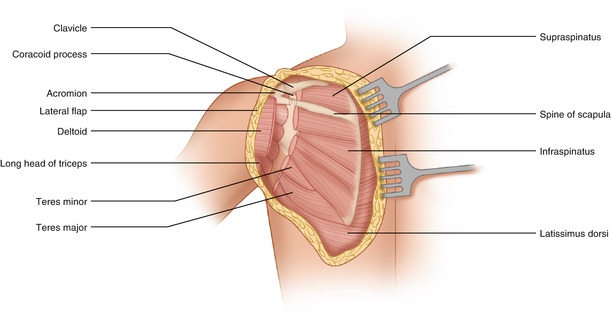
Fig. 15.1
The medial flap is developed. The relevant portion of trapezius muscle is divided
Fig. 15.2
The levator scapulae, rhomboid minor and major are divided. Also, part of latissimus dorsi as it skirts the tip of the scapula
Fig. 15.3
The lateral flap is developed. The posterolateral portion of the deltoid is detached off the spine of the scapula and the acromioclavicular arch. At the level of the neck the teres major, teres minor, and infraspinatus are divided
If a subtotal scapulectomy is planned, the acromion is divided off the spine of the scapula, along with the supraspinatus muscle. The specimen is retracted from the medial side. The insertion of the pectoralis minor to the coracoid process, as well as the origin of the coracobrachialis and the short head of the biceps brachii, may be preserved. Thus, if the tumor is not too close, the coracoid process may be left attached to the lateral angle of the scapula by the glenoid. After the supraspinatus is divided at the neck of the scapula, the coracoid process is visualized better, so that the osteotome or a Gigli saw can be guided through the neck of the scapula just medial to the coracoid (Fig. 15.4). The origin of the long head of the triceps brachii from the lateral border of the scapula next to the glenoid is divided. If the bone is divided at the level of the spine of the scapula, where this process becomes the free end (acromion), it is possible, as mentioned above, to preserve a small part of the scapula with the glenoid and with the coracoid process on the anterior aspect of the remaining bone. Doing so helps to retain the ligaments connecting the coracoid process to the acromion process, clavicle, and humerus, significantly preserving the stability of the shoulder joint. To free the anterior aspect of the scapula, the serratus anterior is divided close to its rib origin (second to ninth ribs), and the subscapularis muscle is divided near its insertion to the lesser tubercle of the humerus (Fig. 15.5).