(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
In removing a portion of the large bowel for adenocarcinoma, the en bloc resection of the appropriate corresponding portion of the mesocolon has been standardized, according to the location of the particular colon cancer, such as right hemicolectomy, left hemicolectomy, sigmoid resection, and so forth. For carcinoma of the small intestine, it is also well known and adequately standardized that in addition to removing an adequate length of small bowel proximal and distal to the tumor, the corresponding mesentery should be removed in a triangular shape from the mesenteric border of the small bowel at the points of its intended proximal and distal division to the base of the mesentery. When primary tumors involve the mesentery itself, however, particularly when the base of the mesentery is involved close to the proximal loops of small bowel, methods of dealing surgically with the situation are not clear. One finds in perusing the literature that often the resectability of tumors at the base of the mesentery is decided upon mere palpatory or visual examination, the rationale being that tumors at the base of the mesentery in this proximal portion probably involve the superior mesenteric vessels, so an attempt at resection poses the risk of complete devascularization of the small bowel and the right colon. The result for the patient would be a permanent need for intravenous hyperalimentation due to short-bowel syndrome. We have found, however, that in cases of desmoid tumors involving the small bowel or mesentery or retroperitoneal sarcomas located at the base of the mesentery (often causing bowel obstruction), dissection at the base of the mesentery and exposure of the superior mesenteric vessels allows preservation of the latter and resection of most of these tumors. The exposure of the superior mesenteric vessels to establish the presence or absence of actual involvement by the tumor of these vessels is the definitive way to decide deliberately whether the tumor can be removed safely.
In patients with Gardner’s syndrome, in whom the large bowel has been removed and a permanent ileostomy created, it is even more critical to assess the location of a desmoid tumor at the base of the mesentery and determine whether one can preserve some of the proximal small bowel, or perhaps most of the small bowel, depending on the relationship of the desmoid tumor to the superior mesenteric vessels and their branches.
For tumors involving the distal part of the mesentery and possibly the superior mesenteric vessels near their termination, the ileocolic artery being the last branch from the right side of the superior mesenteric artery (SMA), resection is not a problem. One can proceed with a right hemicolectomy and removal of the distal ileum without difficulty, followed by anastomosis between the ileum and the colon.
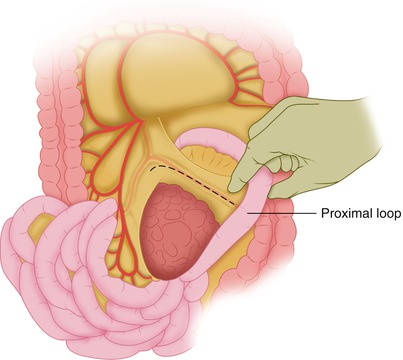
The case illustrated here is one of tumor in the mesentery of the proximal small bowel in which, if the superior mesenteric vessels are not carefully dissected, the result could be loss of all of the small bowel except the first foot or so of jejunum, as well as the right colon (for patients who still have their colon), causing continuous dependence on intravenous hyperalimentation. Certainly this result would not be advisable for a patient with a desmoid tumor, which can be dealt with otherwise, given that it does not metastasize; if the tumor is not resectable, one needs only to palliate the symptoms it causes, usually with an intestinal bypass of the obstructed area. By safely demonstrating the relationship of the tumor at the base of the mesentery to the superior mesenteric vessels, however, it is possible to proceed deliberately with a resection when it seems that the main trunks of the superior mesenteric vessels are not involved.
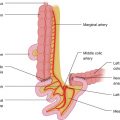
An incision in the mesentery is made from a point proximal to the involved mesentery, starting at the mesenteric border of the bowel and proceeding toward the base of the mesentery, the incision in the peritoneal leaf continued over the course of the mesenteric branches (Fig. 32.1). The adipose tissue covering the pairs of arterial-venous branches in the mesentery is carefully incised and dissected, but only as needed in order to be able to trace these mesenteric branches to the base of the mesentery (Fig. 32.2). The superior mesenteric vein (SMV) is first exposed, and its tributaries from the involved mesentery are ligated and divided close to the surface of the SMV (Fig. 32.3). To the left of and posterior to the SMV, the superior mesenteric artery (SMA) is exposed. From the left side of the SMA, 12–15 branches arise, distributed to the jejunum and ileum. These run almost parallel in the mesentery, each dividing to unite with adjacent branches in a series of arches. Branches from the first arch unite to form a second series, and this may be repeated three or four times. Following one of the artery-vein pairs of the mesenteric branches vertically disposed to the mesenteric border of the bowel, one is led to the surface of the superior mesenteric vessels. The bowel loop immediately distal to the tumor involvement of the mesentery is exposed. An incision is made in the peritoneal leaf from the mesenteric border of this bowel loop to the base of the mesentery and then carried on the surface of SMV in a proximal direction, where it is met with the incision coming from the site of the mesentery proximal to the area of tumor involvement. One thus exposes the surface of the SMV; and any remaining tributaries of the SMV coming from the area of the involved mesentery are ligated and divided serially (Fig. 32.3). Following division of the tributaries to the SMV from the involved mesentery, the SMA is exposed to the left and somewhat deeper (posterior) to the SMV, and all the branches of the SMA leading to the area of involved mesentery are dissected, ligated, and divided (Fig. 32.4). This type of dissection ensures that the blood supply of the distal uninvolved loops of bowel will be safe and intact. It is now possible to proceed with resection of the involved mesentery and the corresponding length of small bowel. The small bowel is divided proximally and distally, and the mesentery also is divided by ligating small branches (arches) from the adjacent mesenteric branches toward the mesentery that is to be removed.