The terms polycythemia and erythrocytosis are often used as if they are interchangeable; in fact, they describe related but distinct findings that usually, but not always, coexist. Polycythemia (“many cells”) describes an increase in the total quantity or volume (mass) of red blood cells in the body without any implication regarding leukocytes or platelets. An increase in the concentration of erythrocytes, however, whether measured as number of cells, hemoglobin (Hb), or packed cell volume (PCV, hematocrit), is more correctly designated erythrocytosis. Erythrocytosis may be the result of an increase in the red cell volume or mass (polycythemia; also called absolute erythrocytosis) or the result of a reduced plasma volume (called relative or spurious polycythemia or erythrocytosis), which produces an increase in red cell concentration that does not reflect an increase in the quantity of red cells in the body.
Despite the precision with which these terms are defined, opportunities for confusion abound. Polycythemia vera (also called polycythemia rubravera) is a myeloproliferative disorder associated with trilineage marrow hyperplasia and characterized by an increased red cell mass, usually in association with leukocytosis and thrombocytosis. The outdated term erythremia refers to this disease (see Chapter 82). Some patients who do not have this myeloproliferative disease are described as having polycythemia vera simply because they have an elevated red cell mass (i.e., their polycythemia is “true” [“vera”]). Confusion on this point is frequently encountered in consultative hematology practice.
PATHOLOGIC PHYSIOLOGY
Red cell survival in polycythemic states is typically normal, implying that increased red cell mass reflects increased erythropoiesis. As the red cell mass rises, the total blood volume typically increases: the variability of changes in plasma volume means that the degree of increase is unpredictable.1
The clinical manifestations of erythrocytosis are related in part to the disorder responsible for erythrocytosis (e.g., thrombosis in patients with polycythemia vera,2 hypertension in relative polycythemia,3 etc.). In addition, the increased blood volume and increased blood viscosity that occur in association with polycythemia themselves produce certain symptoms and signs; these are related to the degree of the increase and the resulting effects on blood flow and oxygen transport.4 Thus, the “ruddy cyanosis” seen in patients with polycythemia vera is a consequence of dilatation of cutaneous vessels by expanded blood volume and sluggish local circulation caused by increased blood viscosity.5, 6, 7 Headache, dizziness, tinnitus, a full feeling in the head, and a bleeding tendency may develop in patients with erythrocytosis and expanded blood volume regardless of the basic cause.8, 9, 10, 11 These symptoms usually are relieved by normalization of the hematocrit.
Blood Viscosity and Oxygen Transport
Viscosity is an intrinsic characteristic of a liquid and represents the tendency of that liquid to resist changes in shape. The viscosity of blood is a result of the interaction of several factors, including the red cell concentration by volume, the physical characteristics (deformability, aggregability, and size) of red cells, the plasma volume, plasma proteins, platelet count, and leukocyte number and character.12 In this chapter, the red cell concentration by volume is referred to as the hematocrit, reflecting common usage. Other authors, particularly those studying rheology and oxygen transport, refer to this parameter as the volume of packed red blood cells or PCV. As discussed below, the blood viscosity affects the oxygen content and delivery. This section focuses primarily on the contribution of red cell concentration to viscosity and oxygen transport; more complete discussions are available elsewhere.12
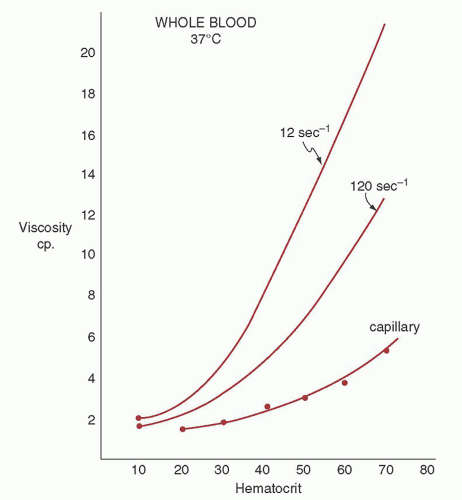
The rate of flow of a liquid through a tube of fixed length is directly related to the pressure gradient across that length of tube and to the radius raised to the fourth power (r4) and inversely related to the viscosity of that liquid (Poiseuille’s law).9, 10, 13, 14 Determinations of the effects of erythrocytosis on blood viscosity were largely made by determining the flow rate of venous blood through an 18-gauge needle under known pressure and thus calculating viscosity.14 The values thus determined are only an approximation of the in vivo situation. Poiseuille’s law is strictly applicable only to fluids that maintain constant viscosity under differing flow rates; this is not the case with blood (Fig. 44.1).13, 14 As the velocity of flow (indicated by the shear rate) increases, the viscosity at any given hematocrit decreases.14 Other factors that interact with the hematocrit to contribute to viscosity are the mean erythrocyte corpuscular volume (MCV) and mean corpuscular hemoglobin (MCH).15, 16, 17 At any given hematocrit, decreased MCV or MCH (or both) is associated with increased viscosity, especially at low flow rates.16, 17 This is a clinically significant observation, because iron deficiency (low MCV) with a normal Hb or hematocrit is a common endpoint of the treatment of polycythemia by phlebotomy.
FIGURE 44.1. Relation of volume of packed red cells (hematocrit) to blood viscosity in centipoise (cp) as measured in a capillary viscosimeter compared with that calculated for shear rates of 120 sec-1 (ascending aorta) and 12 sec-1 (medium arteriole). (From Wells RE Jr, Merrill EW. The variability of blood viscosity. Am J Med 1961;31:505, with permission.)
It is noted above that the model for determining blood viscosity represents a somewhat artificial system: calculated values probably exceed those existing in vivo.13 However, studies of cerebral blood flow in patients with erythrocytosis of various etiologies have demonstrated the clinical effects of an elevated hematocrit on in vivo blood flow.18, 19, 20, 21 Cerebral blood flow in patients with erythrocytosis was significantly reduced compared to controls whether it was due to an elevated red cell mass,19 due to reduced plasma volume,20, 21 or of unknown etiology18 (Table 44.1). Hematocrit reduction, either by venesection18, 19, 20, 21 or by volume expansion,21 improved cerebral blood flow.
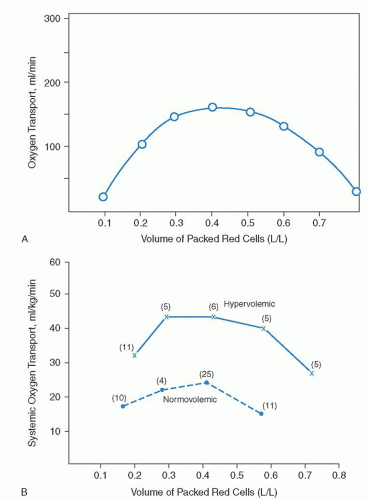
The determination of blood viscosity values at different hematocrits allows the estimation of blood flow rates under different conditions. As Poiseuille’s law predicts (and the data in Table 44.1 imply), blood flow decreases linearly with increasing viscosity.22 The rate of oxygen transport can then be calculated from the blood flow rate and oxygen content. At a given vessel size and pressure gradient, the predicted relation of oxygen transport to hematocrit is expressed by an arch-shaped curve (Fig. 44.2A).14, 22, 23 At low hematocrits, the reduced Hb content of blood translates into reduced oxygen content. At elevated hematocrits (>0.5 to 0.6), increased viscosity reduces oxygen transport despite increased blood oxygen content. Optimal oxygen transport would be predicted to occur in the normal hematocrit range.22, 23, 24, 25, 26 Experiments in normovolemic dogs (Fig. 44.2B, dashed line) support this prediction.23
The differences in oxygen transport observed between normovolemic and hypervolemic dogs at different hematocrits (Fig. 44.2B) reflect the probable situation occurring in patients with erythrocytosis due to an expanded red cell mass (polycythemia). In polycythemia, the associated hypervolemia permits an oxygen transport curve that is similar to that of normovolemic patients but which is elevated and shifted to the right.23, 26 Therefore, in patients with tissue hypoxia, polycythemia is beneficial because it leads to hypervolemia and increases oxygen transport (compare oxygen transport at hematocrit 0.6 on the hypervolemic and normovolemic curves in Fig. 44.2B). In contrast, in patients who have a normal or decreased total blood volume (as in relative or spurious polycythemia), erythrocytosis has an adverse effect on oxygen transport.
Relation to Treatment of Polycythemia
The considerations noted above are of interest in understanding not only the pathophysiology of the different etiologies of erythrocytosis, but also their treatment. Patients with polycythemia vera have no need for increased tissue oxygen transport. In some areas where fixed vessel diameter (from arteriosclerosis) limits increased blood flow, however, the additional impeding effect of increased blood viscosity may limit oxygen transport and result in local tissue ischemia. Phlebotomy can bring about a significant clinical benefit (see Chapter 82). When treating by phlebotomy, however, blood volume should not be reduced too greatly at any one episode, especially in patients with known symptoms of cardiovascular disease (angina pectoris, transient ischemic attacks). This is particularly true early in the course of therapy, when hematocrit (and consequently viscosity) is highest.27 Rather, time should be allowed for hemodilution to occur between phlebotomies; in emergencies, the blood volume should be maintained by infusing saline or some other plasma expander.6 A concern is that the patient not suddenly be shifted from the hypervolemic, erythrocytosis-beneficial curve to the normovolemic, erythrocytosis-adverse curve. Another concern is that a sudden fall in blood volume from any cause, such as dehydration or acute hemorrhage, may result in local ischemia because increased cardiac output cannot compensate immediately for the effects of high viscosity. In patients with congestive heart failure, the need for reduction of blood viscosity may be urgent, because the ability to increase cardiac output to compensate for the increased blood viscosity has been compromised. The oxygen-Hb dissociation curve is shifted to the right in such patients.28
TABLE 44.1 EFFECT OF ERYTHROCYTOSIS ON CEREBRAL BLOOD FLOW
Note: Values expressed as mean ± standard deviation.
FIGURE 44.2. Arterial oxygen transport at different volumes of packed red cells and thus different viscosity values. A: Values in curve were calculated from blood viscosity values as measured by Pirofsky.9B: Systemic oxygen transport as calculated from cardiac output measured in normovolemic and hypervolemic dogs. (From Murray JF, Gold P, Johnson BL Jr. The circulatory effects of hematocrit variations in normovolemic and hypovolemic dogs. J Clin Invest 1963;42:1150-1159, with permission.)
In contrast to polycythemia vera, patients with polycythemia due to tissue hypoxia may benefit from an increased hematocrit. Reduced arterial oxygen saturation means that blood oxygen transport is less efficient at particular Hb or hematocrit levels. Therefore, the curves for oxygen transport would be shifted closer to the origin than those noted in situations in which Hb oxygenation is normal (Fig. 44.2B). In the presence of decreased arterial oxygen saturation, tissue hypoxia may persist even when erythrocytosis is marked. The main advantage to decreasing blood viscosity and blood volume in hypoxic (secondary) polycythemia is to decrease the cardiac workload. One would predict that in such situations an increase in tissue oxygen transport and clinical improvement should result from phlebotomy; results show that this is the case.29 Again, especially early in the course, phlebotomy with preservation of an expanded blood volume may be beneficial.6, 27 To achieve the best balance between increased cardiac work and decreased tissue hypoxia in patients with hypoxemic erythrocytosis, some authors suggest that the hematocrit be maintained between 0.50 and 0.55;6, 29 however, the subjective symptomatology of the patient is usually the best guide.22
CLASSIFICATION AND APPROACH TO THE PATIENT WITH ERYTHROCYTOSIS
An increase in hematocrit (erythrocytosis) may result from decreased plasma volume or from polycythemia, which is an increase in the absolute quantity of red cells or red cell mass. The various forms of erythrocytosis are listed in Table 44.2. They are classified according to red cell mass (relative erythrocytosis or polycythemia vs. actual polycythemia). Polycythemia, in turn, is divided into primary polycythemia (polycythemia vera and familial primary polycythemia/primary proliferative polycythemia) and polycythemia driven by erythropoietin production (secondary polycythemia). The secondary polycythemic syndromes are divided into those that represent a response to tissue hypoxia (physiologically appropriate) and those driven by erythropoietin not produced in response to tissue hypoxia (physiologically inappropriate).
TABLE 44.2 CLASSIFICATION OF ERYTHROCYTOSIS
Relative Erythrocytosis or Polycythemia (Spurious Polycythemia)
Hemoconcentration
Spurious polycythemia (Gaisböck syndrome)
Polycythemia (Absolute Erythrocytosis)
Primary polycythemia
Polycythemia vera
Primary familial polycythemia
Secondary polycythemia
Secondary to decreased tissue oxygenation (physiologically appropriate polycythemia or hypoxic erythrocytosis)
High-altitude erythrocytosis (Monge disease)
Pulmonary disease
Chronic cor pulmonale
Ayerza syndrome
Cyanotic congenital heart disease
Hypoventilation syndromes
Primary alveolar hypoventilation
Pickwickian syndrome, Ondine curse
Positional desaturation
Sleep apnea
Abnormal hemoglobins
Inherited
Acquired: Drugs and chemicals, carboxyhemoglobin
Familial polycythemia
Secondary to aberrant erythropoietin production or response (physiologically inappropriate polycythemia)
Tumors, cysts, hemangiomas, and so forth
Androgen abuse
Erythropoietin abuse
Familial polycythemia
Idiopathic polycythemia
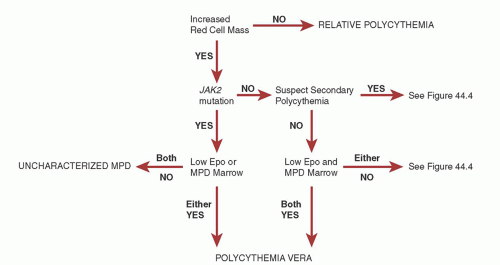
An approach to the evaluation of the patient with erythrocytosis is outlined in Figures 44.3 and 44.4. Although actual polycythemia can usually be differentiated from relative polycythemia on clinical grounds (as described below), an assessment of the red cell mass is the initial step in evaluation. Traditionally, this has been done by measurement of red cell mass and blood volume by isotope labeling. Normal values are presented in Table 44.3, but considerable variation exists from one subject to another in red cell, plasma, and total blood volume, even when expressed as milliliters per kilogram (ml/kg) body weight. This variation results, in part, from differences in body fat content31, 32, 33, 34; blood volume is more closely related to lean body mass33 than to weight or surface area. It has been proposed that a red cell mass of at least 125% of that predicted should be considered as indicating polycythemia.35 It has been a common practice at many to measure either plasma volume or red cell volume and, from one of these determinations, to calculate total blood volume on the basis of the relative amounts as indicated by a hematocrit determination. In the view of most,36, 37, 38 but not all,15 investigators, this practice is associated with an increased chance of error; measuring red cell mass and plasma volume separately is preferable. It must be emphasized that blood volume measurements do not differentiate between secondary polycythemia and polycythemia vera; they are useful only in distinguishing absolute from relative erythrocytosis.
However, availability of actual red cell volume measurement has become limited to a small number of large medical centers with special expertise. Surrogate measures based on Hb or hematocrit are now the routine basis for distinguishing relative and actual polycythemia. In men with a hematocrit > 0.60 or women with a hematocrit > 0.55, there is reported to be >99% likelihood that the red cell mass is elevated.39 In its 2007 criteria for the diagnosis of polycythemia vera, the World Health Organization (WHO) uses an Hb concentration of >18.5 g/dl in men or 16.5 g/dl in women to define an elevated red cell mass.40 In a comparative study, the hematocrit 0.60/0.55 standard was reported to identify elevated red cell mass more accurately than the Hb concentration 18.5/16.5 g/dl standard.41 It should be noted that in certain circumstances of severe hemoconcentration (e.g., in the systemic capillary leak syndrome42), Hb concentrations or hematocrits in this range may be observed in patients with a normal red cell mass. Such patients typically exhibit anasarca and other physical findings suggestive of severe intravascular volume depletion and redistribution of intravascular volume.
The goal of the approach outlined in Figures 44.3 and 44.4 is initially to distinguish spurious (relative) polycythemia from actual polycythemia, then to distinguish polycythemia vera from secondary polycythemia and primary proliferative polycythemia, to rule out other primary polycythemia, and finally to identify the etiology of secondary polycythemia. The characteristics of polycythemia vera are outlined in Chapter 82; the other polycythemic syndromes are discussed below. A certain number of patients are not readily classified as having either polycythemia vera or secondary polycythemia. These patients fall into a category called (for want of a more physiologic term) idiopathic polycythemia or idiopathic erythrocytosis and appear to represent a heterogeneous group of disorders (see below).
The diagnostic approach to polycythemia has been substantially altered by the observation that more than 95% of patients with polycythemia vera express a mutation in the JAK2 gene in which phenylalanine is substituted for valine at position 617.43, 44, 45JAK2 V617F mutation-negative polycythemia vera patients have been reported to have mutations in other exons of JAK2.46 It is tempting to regard the JAK2 mutation in polycythemia vera as conceptually analogous to the bcr/abl mutation in chronic myelogenous leukemia; however, the JAK2 V617F mutation is also found in other myeloproliferative disorders.44 Its implications are discussed in more detail in Chapter 82, but in terms of differential diagnosis, it should be regarded as a marker of a myeloproliferative state. Polymerase chain reaction-based assays for JAK2 V617F versions of this test are widely available through reference laboratories in the United States and Europe at costs in the $300 to $500 range. As the role of JAK2 assessment in the approach to myeloproliferative disorders continues to expand, increasing numbers of medical centers are developing in-house tests for JAK2 V617F.
FIGURE 44.3. Approach to patients with erythrocytosis. EEC, endogenous erythroid colonies; EpoR, erythropoietin receptor; JAK2 mutation, testing for JAK2 V617F or other mutations associated with polycythemia vera; low Epo, serum or plasma erythropoietin concentration less than the lower limit of normal; MPD, myeloproliferative disorder; MPD marrow, bone marrow findings suggestive of a myeloproliferative disorder (see text); MPD, myeloproliferative disorder; VHL, von Hippel-Lindau protein.
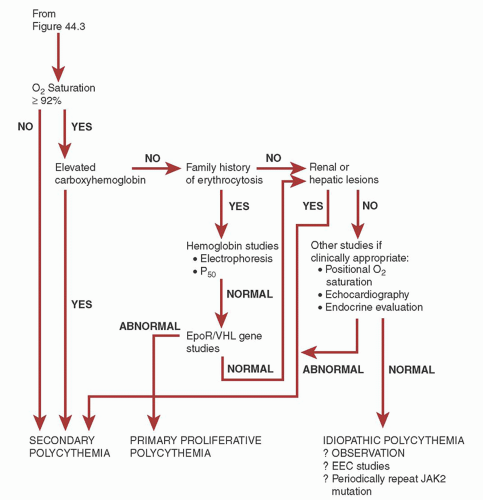
FIGURE 44.4. Approach to patients with erythrocytosis. JAK2 V617F-negative erythrocytosis. CNS, central nervous system; EEC, endogenous erythroid colonies; EpoR, erythropoietin receptor; MPD, myeloproliferative disorder; VHL, von Hippel-Lindau protein.
TABLE 44.3 NORMAL VALUES FOR RED BLOOD CELL, PLASMA, AND TOTAL BLOOD VOLUME (ML/KG ± 1 STANDARD DEVIATIONa)
aRed blood cell volume measured by 51Cr method. Other values calculated without correction for trapped plasma.
bOnly values of which we are aware at altitudes significantly above sea level. They may be somewhat low for unknown reasons; the packed cell volumes at 1,600 m were the same as at sea level, a finding that contradicts an earlier author’s own large experience.
The WHO criteria for the diagnosis of polycythemia vera requires evidence of an increased red cell mass, and a JAK2 or other functionally similar mutation and one minor criterion; or evidence of an increased red cell mass and all three minor criteria.40 The minor criteria are a serum or plasma erythropoietin concentration below the range of normal for the laboratory; a bone marrow examination exhibiting the characteristic features of a myeloproliferative disorder (hypercellularity with trilineage hyperplasia, clustered pleomorphic megakaryocytes, and no features of inflammation) and the formation of erythroid colonies in vitro in the absence of added erythropoietin (“endogenous erythroid colonies”[EECs]).40 Although these tests can be evaluated in any order desired, ease of test access would suggest that erythropoietin concentration be ordered first, followed by marrow evaluation if necessary. In a JAK2 mutation-positive patient, either a characteristic erythropoietin concentration or a characteristic marrow would permit the diagnosis of polycythemia vera. In a JAK2 mutation-negative patient, absence of both a characteristic erythropoietin concentration and a characteristic marrow would rule out the diagnosis. EEC assays, a hallmark of myeloproliferative disorders in general,47, 48 are not readily available outside of research laboratories, which limits their diagnostic practicality.
The roles of erythropoietin levels and EEC assays in the differential diagnosis of erythrocytosis are most strongly supported by their association with the WHO diagnostic criteria; as stand-alone tests in individual cases, utility is less clear.49, 50, 51 Although mean serum erythropoietin concentration in the subset of patients with polycythemia vera is significantly lower than that observed in secondary polycythemia, there is considerable overlap, making it less useful for individual cases. This would be expected physiologically. A patient with secondary polycythemia due to tissue hypoxia would have an elevated serum erythropoietin level until the hematocrit was sufficiently high to oxygenate tissue adequately; then the erythropoietin concentration would be expected to decrease. The intermittent nature of detection of an elevated serum erythropoietin concentration in secondary polycythemia has been described,52 as has the failure of serum erythropoietin concentrations to predict clinical course in idiopathic erythrocytosis.53 Studies have been reported demonstrating that polycythemia vera and secondary polycythemia can be distinguished based on the serum erythropoietin response to phlebotomy: after phlebotomy, serum erythropoietin levels increase in secondary polycythemia but remain stable in polycythemia vera.49 EECs corresponding to erythroid burst-forming units were observed in 12 of 17 polycythemia vera patients, 3 of 11 secondary polycythemics, 1 of 6 relative polycythemics, and 1 of 11 normal individuals in one series.54
Soluble transferrin receptors are typically elevated in all forms of polycythemia and thus do not distinguish polycythemia vera and secondary polycythemia.55
As a general approach to the evaluation of erythrocytosis, all patients with presumed polycythemia should undergo JAK2 V617F testing. If the clinical features are suggestive of a secondary etiology of polycythemia, patients who do not show a JAK2 mutation should follow the process outlined in Figure 44.4. Individuals without a documented JAK2 mutation but in whom suspicion of a myeloproliferative disorder is high, should be investigated for minor WHO criteria (Fig. 44.3).
RELATIVE POLYCYTHEMIA
Lowered fluid intake, marked loss of body fluids, or a combination of both causes a decrease in plasma volume and may produce a relative erythrocytosis. The decrease in plasma volume may result from any cause of intravascular fluid loss, insensible fluid loss, persistent vomiting, severe diarrhea, copious sweating, postoperative complications, or shift of fluid into the extravascular space (“third spacing”)3, 37, 42, 56 or may be an effect of high altitude.53 In severe burns, plasma loss leads to hemoconcentration.
Chronic relative polycythemia or erythrocytosis has been variously referred to as Gaisböck syndrome,57“stress” erythrocytosis,3benign polycythemia,52, 56benign erythrocytosis,58spurious polycythemia,59, 60pseudopolycythemia,61 and apparent polycythemia.62 The last three terms are the most accurate: in the absence of an elevated red cell mass, there is no polycythemia. In one series of 215 patients referred with a diagnosis of polycythemia vera,63 18 (8.3%) were believed to have chronic relative erythrocytosis, possibly caused by “stress.”3 Patients with relative polycythemia or erythrocytosis are typically male; the mean age at diagnosis is less than is seen in patients with polycythemia vera.62 Obesity is typically described as an associated feature,3 although not all studies support this association.64 Other features reported to be strongly associated with relative polycythemia are hypertension and smoking;62, 64, 65 associations with alcohol abuse and renal disease are occasionally reported.62, 63 It is probable that this syndrome is not a true clinical entity.60 The red cell mass values generally accepted as normal at sea level, or at any given altitude, represent the mean ±2 standard deviations. Thus, on the basis of the normal frequency distribution curve for this physiologic parameter, the values in 2.5% of the population are above this range. The individuals in this group should not be regarded as necessarily abnormal.66
The optimal management of relative polycythemia is unknown. As noted previously, phlebotomy increases cerebral blood flow even in patients with relative polycythemia; whether it is of symptomatic benefit is less clear.20, 21 It should probably be avoided. Theoretic arguments can be made that contracting the blood volume further in these patients who already are normovolemic or slightly hypovolemic may impair tissue perfusion. Satisfactory control of hematocrit can be obtained in at least two thirds of patients by reduction of excess weight, improved hypertension control, avoidance of diuretics, and reduction if not cessation of smoking.64 Potentially leukemogenic cytoreductive therapy, such as radioactive phosphorus or oral chemotherapeutic agents, is probably never indicated.
Only gold members can continue reading. Log In or Register to continue