Epidemiology of Infectious Disease: General Principles
Epidemiology of Infectious Disease: General Principles
Kenrad E. Nelson
INTRODUCTION
Studies of the epidemiology of infectious diseases include evaluation of the factors leading to infection by an organism, factors affecting the transmission of an organism, and factors associated with clinically recognizable disease among those who are infected. Epidemiologic concepts such as the incubation period and resistance were originally developed in studies of infectious diseases and later applied to noninfectious diseases.
Epidemiologic characterization is the first step in defining a new disease, although diseases can also be classified according to their clinical or microbiologic features. For the public health professional, it is the epidemiologic features—for instance, the prevalence, incidence, transmission route, and susceptible populations—that are of paramount importance in developing a control program. In contrast, a clinician whose primary role is to treat a disease may be more concerned with the clinical symptoms or pathophysiology. For example, an infectious agent that causes secretory diarrhea will be treated empirically with fluid replacement and symptomatic management of the pathophysiology, irrespective of how the infection was acquired or what the infectious organism is. A microbiologist will be concerned primarily with the characteristics of the organism and will focus on the tasks of isolation, identification, and development of targeted treatments.
The control, treatment, and prevention of an epidemic usually requires the cooperative efforts of all three groups of specialists—clinicians, microbiologists, and epidemiologists. However, each has a unique orientation and contribution to make to this field. The perspectives from each of these three areas of study can best be appreciated by considering how infectious diseases are classified by each specialist.
THE CLASSIFICATION OF INFECTIOUS DISEASES
Clinicians tend to classify infectious diseases according to their most common or most important clinical manifestation or by the organ systems that are primarily affected. An example of a clinical classification is given in Table 2-1.
Microbiologists use classification schemes focused on the characteristics of the causative organism. An example of a typical microbiologic classification of infectious diseases is shown in Table 2-2.
Epidemiologists focus on the epidemiologic characteristics of a disease and classify diseases according to either the means of transmission or the reservoir of the organism. Infectious diseases can be classified according to their means of transmission into five distinct categories, as shown in Table 2-3. With the epidemiologic classification of infectious diseases according to where the pathogen is found, the most generalized form of categorization is based on whether a pathogen is either native to humans, animals, soil, or water. Some common examples of infectious diseases classified according to their reservoir are shown in Table 2-4.
When a new disease appears on the scene, the detailed microbiologic characteristics of the organism are typically unknown. Likewise, the full clinical manifestation may be undefined. For example, the fact that infection with Borrelia burgdorferii, the cause of Lyme disease, was responsible not only for the classical skin lesion, erythema chronica migrans (ECM), but also for acute and chronic arthritis, vascular and cardiac disease, and neurologic symptoms, including Bell’s palsy and encephalitis, was not appreciated initially. In fact, the full range of clinical manifestations of infection with B. burgdorferii is still being defined.
Table 2-1 Clinical Classification of Infections
Classification
Infection
Diarrheal diseases
Secretory
Invasive
Respiratory diseases
Upper respiratory
Lower respiratory
Central nervous system infection
Meningitis (bacterial vs. aseptic)
Encephalitis
Abscess
Cardiovascular infection
Endocarditis
Myocarditis
Vasculitis
Sepsis
Disseminated
Table 2-2 Microbiologic Classification of Infectious Diseases
Classification
Organism
Bacterial
Gram-negative
Gram-positive
Viral
DNA virus
RNA virus
Enveloped vs. nonenveloped viruses
Fungal
Disseminated (biphasic)
Localized
Parasitic
Protozoa
Helminths
Trematodes
Cestodes
Prion
Protein
Table 2-3 Classification of Infectious Organisms by Their Means of Transmission
Transmission
Characteristics
Contact
Requires direct or indirect contact (indirect 5 infected fomite, blood, or body fluid; direct 5 skin or sexual contact)
Food- or water-borne
Ingestion of contaminated food (outbreaks may be large and dispersed, depending on distribution of food)
Airborne
Inhalation of contaminated air
Vector-borne
Dependent on biology of the vector (mosquito, tick, snail, etc.), as well as the infectivity of the organism
Perinatal
Similar to contact infection; however, the contact may occur in utero during pregnancy or at the time of delivery
Table 2-4 Classification of Infectious Organisms by Their Reservoir in Nature
Reservoir
Some Typical Organisms
Human
Treponema pallidum, Neisseria gonorrhoeae, HIV, hepatitis B and C virus, Shigella, S. typhi
If one is aware of the reservoir of the agent in addition to the means of transmission, it is generally possible to develop a strategy to prevent transmission, even when the microbiologic characteristics of the organism are not known. The demonstration of the water reservoir of cholera by John Snow in London in 1853 preceded the identification of the Vibrio cholera by Robert Koch in 1884.1 In this case, the epidemiologic information alone was sufficient to develop public health strategies to limit exposure to contaminated water and prevent human infections. Similarly, the demonstration of the importance of human carriers of Salmonella typhi as the important reservoir in outbreaks of typhoid fever by Budd in 1858 antedated by 22 years the isolation of the infectious organism in the laboratory by Eberth in 1880. Walter Reed succeeded in transmitting yellow fever by the bite of infected Aedes aegypti mosquitoes in 1901, but it was not until 1928 that Stokes and colleagues isolated the causative virus in the laboratory. In more recent times, investigation of pneumonia at the American Legion convention in Philadelphia in 1976 demonstrated that disease was due to airborne spread of microorganisms from the air-conditioning system and suggested that infection could be prevented by avoiding the air in the hotel.2 The implicated organism, Legionella pneumophila, was not isolated and characterized in the laboratory until 1978, when it was identified by McDade and Sheppard at the Centers for Disease Control and Prevention (CDC).
Knowledge of the reservoir often is essential before one can devise rational and effective means of preventing transmission of infectious diseases. Prior to John Snow’s demonstration that contaminated water was the reservoir of Vibrio cholerae in the outbreak in London in the 1850s, the predominant theories were that miasma—that is, exposure to foul or malodorous air—was the critical exposure leading to infection. However, there were no successful efforts to control the outbreak that were based on the miasma theory. When Snow demonstrated that attack rates of cholera were highest in those persons who received their water from one particular water company and subsequently terminated an epidemic by closing down the pump at one water source, the evidence was persuasive.1
Infectious Diseases Transmitted by More Than One Means
Some organisms may be spread by several different means, depending on the epidemiologic circumstances. Therefore, it is important for an epidemiologist to keep an open mind to detect unusual epidemiologic features of an infection. A few examples of infectious diseases that have been spread by multiple means are described here.
Tularemia
Perhaps a typical example of a disease that can be spread by more than one means is tularemia, which can be acquired by the bite of infected ticks or deer flies,8 by contact with infected rabbits or other animals during the hunting season,9, 10 or by inhalation of an aerosol.11, 12 In addition, nosocomial infection among microbiology laboratory workers has been reported from inhalation of infected aerosols of the causative organism, Francisella tularensis.13 Curiously, none of the investigators who have studied epidemics of tularemia have found evidence of human-to-human transmission.14
Plague
Plague—the disease that has been associated with perhaps the most serious and extensive epidemic in human history—is caused by the plague bacillus, Yersinia pestis. This zoonotic disease of rodents is transmitted to humans and other mammalian hosts from infected rodents by rat fleas. Percutaneous inoculation of the plague bacillus in humans initiates inflammation of lymph nodes draining the inoculation site, resulting in bubonic plague. Bloodstream invasion may lead to septicemic plague or to infection of other organ systems, such as the lung or meninges. Involvement of the lungs may result in pneumonic plague, which can then be transmitted from person to person via the respiratory route.
Historically, many epidemics of plague have spread rapidly through populations, causing very high mortality. The earliest description of plague dates from the sixth century AD in Egypt, when the epidemic spread throughout North Africa and into Europe. Epidemic plague reappeared in the Far East in the 1300s and subsequently spread to Europe. During the “Great Plague” epidemic in London, which peaked in August and September 1665, 7,000 deaths per week were reported in a population of an estimated 500,000 persons. For unknown reasons, plague gradually disappeared from Europe in the 1700s, and the entire continent was free of plague by 1840.15 Zinsser considers the disappearance of epidemics of plague from Europe to be one of the great mysteries of the epidemiology of infectious diseases.16
However, epidemics of plague did occur in Asia in the late 1800s and more recently in Vietnam, during the war between 1962 and 1975.17 An epidemic of plague was reported in India in 1994.18 Sporadic cases of plague have occurred throughout the American Southwest for the past several decades, related to epizootics in infected prairie dogs.19, 20 The infectious organism was first isolated by Yersin in Hong Kong in 1894.21 Although a vaccine is available, its efficacy in preventing pneumonic plague is unknown.
Anthrax
Anthrax is an infection with Bacillus anthracis, a gram-positive spore-forming organism that causes a zoonotic disease in herbivorous animals. The pathogen can be transmitted to humans from contact with infected animals, and the resulting disease has three clinical forms in humans: cutaneous, gastrointestinal, and inhalation anthrax.
The organisms from infected animals most often infect humans by contact with contaminated animal hides or pelts; this disease has been called woolsorter’s disease.22 Infection can also occur by inoculation of organisms into the skin during butchering of an infected animal; this type of exposure usually leads to cutaneous anthrax, consisting of a black eschar on the skin with swelling and inflammation of the draining lymphatics. Consumption of meat from an infected animal leads to gastrointestinal anthrax, which has a much higher mortality than does cutaneous anthrax. Inhalation anthrax occurs when an infectious aerosol of B. anthracis spores is inhaled and germinates in the pulmonary lymphatic tissues. This form of anthrax is rare, which is fortunate because it usually proves rapidly fatal.
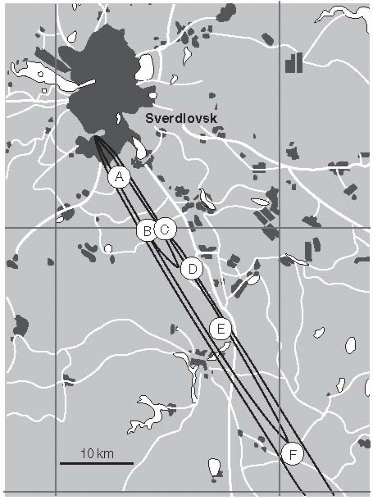
An epidemic of inhalation anthrax occurred among persons living in Sverdlovsk, Union of Soviet Socialist Republics, in April and May 1979. At least 96 cases and 66 deaths occurred. The outbreak also affected cattle within 50 kilometers of the city. Interestingly, Sverdlovsk was known to have a military facility that was suspected of manufacturing biologic weapons, including anthrax spores, for potential use in warfare. Initially, the Soviet authorities maintained that this outbreak was from gastrointestinal exposure due to the consumption of contaminated meat from cattle that had died of anthrax. However, in 1992, Meselson and colleagues visited the site of the epidemic and were able to conduct an epidemiologic investigation, together with Russian scientists. Their study found that all of the human cases were living or working in a narrow belt south of the city on the day the outbreak occurred.23 Furthermore, the animal deaths also occurred in this belt, up to 50 kilometers distant (Figure 2-1). The wind pattern on the day of the outbreak could explain the geographic distribution of cases. Subsequently, evidence was discovered that many of the human cases had pneumonic anthrax. The researchers concluded that this outbreak—the largest outbreak of human inhalation anthrax ever recorded—was due to an infectious aerosol emanating from the military facility.
One very interesting finding in this study was that human cases continued to occur for as long as 6 weeks after the initial point-source exposure. Apparently, spores were inhaled and continued to germinate and cause disease for several weeks after they were inhaled. This outbreak has raised considerable concern among scientists and policymakers about the potential for the use of aerosolized B. anthracis spores as an agent of biologic terrorism. Indeed, these fears were confirmed in 2001 when an outbreak of 22 cases of anthrax occurred in the United States from intentional contamination of the U.S. mail delivered to a number of persons by the U.S. Postal Service. This outbreak is described in detail in the chapter on emerging infections.
Rabies is a nearly uniformly fatal infection of the central nervous system that is almost always transmitted by a bite from an animal infected with the rabies virus. Historically, rabies has nearly always been acquired by a bite from an infected dog, skunk, fox, bat, or other animal. It has been regarded as a typical contact-transmitted infection, in that percutaneous inoculation of rabies virus by a bite is usually required. Nevertheless, a few persons have developed rabies from exposure to infected aerosols in caves that harbored by many infected bats.24 In addition, rabies has occurred in a laboratory worker who was exposed to an infectious aerosol25 and in persons who have received corneal transplants from a donor who died of undiagnosed rabies.26 In recent years, in the United States, only 2-3 cases have occurred annually; however, reported bite exposures in these cases has been unusual. Of the 32 cases of rabies that were diagnosed in the United States between 1980 and 1996, 25 (78%) had no history of a bite exposure.27 Some of these non-bite-transmitted cases in the United States have occurred in persons exposed in the same room (or closed space) to an infected bat; presumably, the transmission in these cases was by aerosol. Genetic analysis of the viruses has shown that 17 (53%) of these cases in the United States were related to rabies viruses found in insectivorous bats.
Brucellosis
Brucellosis is an infectious disease of humans acquired through contact with an infected animal (i.e., a zoonosis). Four species of Brucellae have infected humans: B. abortus (from cattle), B. melitensis (from goats or sheep), B. suis (from pigs), and B. canis (from dogs). Human infections with the two other known species, B. ovis (from sheep) and B. neotomae (from desert wood rats), have not been reported. Clinically, the most serious human infections are seen with B. melitensis. However, in the early decades of the 1900s, infections with B. abortus were common, and these infections often were acquired by the consumption of contaminated milk from infected cows.
After World War II, the U.S. Department of Agriculture (USDA) undertook a campaign to eliminate milk-borne brucellosis as a human health problem in the United States. The program included testing of cattle for B. abortus and slaughtering of infected animals or animals from infected herds, and pasteurization of all milk and dairy products.28 This program was quite successful. More than 6000 cases of human brucellosis were reported each year at the start of this program; the rate had declined to 4.5 cases per 100,000 population in 1948. In the 1990s, only about 100 cases per year were reported; 0.05 case per 100,000 population was reported in 1993.
In recent years, persons affected brucellosis have usually had an occupation that directly exposed them to infected animals, such as slaughterhouse workers, farmers, or veterinarians. Brucellosis in these workers was acquired by direct contact with infected animals, not through consumption of infected milk. Also, B. suis infections from infected pigs have become proportionally more common, because the brucellosis control program was directed at eliminating the disease in cattle.
Transmission of Microbial Agents by Transfusions
Evidence shows that several microbial agents can be transmitted by blood transfusion or contaminated injection if exposure occurs during a time when the organisms are present in the bloodstream. For example, hepatitis B virus, hepatitis C virus, and HIV are commonly transmitted by the transfusion of blood or blood products. Trypanosoma cruzii, a protozoan parasite that causes Chagas’s disease, is usually transmitted to humans by the bite of a reduviid bug but can be transmitted by blood transfusion from a carrier.29 Malaria usually is caused by the transmission of one of four species of Plasmodium parasites by the bite of an infected female Anopheline mosquito, but it can also be transmitted by blood transfusion or to an infant by perinatal transmission. Hepatitis A virus is generally transmitted by ingestion of contaminated food or water but can be transmitted by blood transfusion during the brief viremic stage early in the infection.
Perinatal Infections
Infections of an infant may be acquired from the mother in utero via placental transfer, during passage through the birth canal, or in the postpartum period.
Rubella
The dramatic effect of rubella infections during the first trimester of pregnancy in producing congenital anomalies in the infant was first reported by Sir Norman Gregg following an outbreak of rubella in Australia in 1940.30 Gregg noted ocular defects and cardiac lesions in the affected infants. Subsequently, these findings were confirmed by studies conducted during rubella outbreaks in Australia, the United States, and the United Kingdom. These studies further defined the congenital rubella syndrome (CRS) from intrauterine exposure to rubella during the first trimester of pregnancy to include cataracts and other ocular abnormalities, cardiac defects, deafness, microcephaly, and mental retardation. Infants exposed during the first trimester of pregnancy have a 90% risk of developing congenital rubella syndrome; during the early second trimester, the risk of congenital abnormalities from exposure to rubella declines to 20-40% and often involves only deafness.
In 1962, the rubella virus was isolated by investigators at Harvard University31 and independently by scientists at the Walter Reed Army Institute of Research.32 Shortly thereafter, in 1964, a major epidemic of rubella and CRS occurred in the United States.33 An attenuated live rubella virus vaccine was developed and licensed in the United States in 1969.34 Subsequently, congenital rubella infections have become rare in the United States, due to routine immunization of infants and screening and selective immunization of susceptible women of childbearing age.
Cytomegalovirus
Cytomegalovirus (CMV) infections during the first trimester of pregnancy are known to lead to congenital malformation, especially of the central nervous system. Cytomegalovirus was first isolated in human fibroblast cultures in 1956.35, 36 and 37 It is possible to screen pregnant women for susceptibility to infection during pregnancy. Epidemiologic studies suggest that CMV infection may occur in about 1% of all U.S. births, or approximately 40,000 infants annually.38 In most instances, these infections are asymptomatic.
In 1990, the CDC established a national surveillance registry in the United States to monitor congenital CMV infections.39 The most common clinical manifestation reported was petechiae, observed in 50% of cases, which was often accompanied by hepatosplenomegaly, intracranial calcification, and thrombocytopenia.
Herpes Simplex Virus
In contrast to CMV and rubella, in utero infection with herpes simplex virus (HSV) is rare, and when it does occur, it is most likely to lead to a miscarriage, rather than a congenital malformation. However, infants can be infected when passing through the birth canal if the mother has an active infection, especially with HSV type 2 (HSV-2), which causes recurrent genital tract infection. When the mother has an active HSV infection at the time of delivery, the infant can develop a generalized infection, which is quite serious. The risk to the newborn is higher when the mother has a primary HSV infection than when the HSV is a recurrence; the risk to the newborn is approximately 40% when exposed to a mother with primary infection, compared with 2-5% when the mother has a recurrent infection. In the latter situation, the infant’s risk is modified by maternal passive transfer of antibodies to HSV-2 and by lower maternal viral load.
Cesarean section is recommended to prevent neonatal herpes in children born to women with active HSV at the time of delivery. Nevertheless, most cases of neonatal HSV occur where the mother was not identified as having active HSV infection. For example, during an 18-month hospital-based surveillance study, CDC identified 184 cases of neonatal herpes, but only 22% of the mothers had a history of genital HSV infection, and only 9% had lesions at the time of delivery.40
Toxoplasmosis
Congenital infection with Toxoplasma gondii occurs when a pregnant woman develops a infection with this pathogen, especially early in pregnancy. Clinical manifestations in the infant at birth may include a maculopapular rash, generalized lymphadenopathy, hepatomegaly, splenomegaly, jaundice, or thrombocytopenia. In addition, the infant can develop meningoencephalitis with cerebrospinal fluid abnormalities, hydrocephalus, microcephaly, chorioretinitis, and convulsions. More typically, congenital infection is asymptomatic at birth, although sequelae can become apparent several years later. Sequelae of congenital Toxoplasma infection include mental retardation and learning disability.
Ocular toxoplasmosis most often results from reactivation of a congenital infection, but it can occur from an acquired infection as well. Ocular toxoplasmosis usually occurs among adults.
Syphilis
Syphilis is caused by infection with a spirochete, Treponema pallidum. It is usually transmitted sexually but can be transmitted by the perinatal (congenital) route by infection through the placenta, especially in the second and third trimester of pregnancy. More rarely, transmission may occur during delivery by contact of an infant with the mucosa of a woman with primary or secondary syphilis during the birth process.
Congenital syphilis can be asymptomatic or it may manifest as multisystem involvement, including osteitis, hepatitis, lymphadenopathy, pneumonitis, mucocutaneous lesions, anemia, and hemorrhage. Late manifestation may involve the central nervous system, bones, teeth, and eyes. Rates of congenital syphilis parallel the rates of primary and secondary syphilis in women and can be prevented by treatment of infected pregnant women with penicillin, to which the organism is uniformly sensitive. Rates of congenital syphilis increased in the late 1980s and early 1990s, in part related to the epidemic of crack cocaine use in the United States.41
Because newborns infected with each of the agents so far have similar clinical symptoms, pediatricians often consider all of them in the differential diagnosis of perinatal infections. The syndrome of congenital infection is often referred to by the abbreviation TORCHS to signify the most common etiologies: toxoplasmosis, rubella, CMV, HSV, and syphilis.
Hepatitis B Virus
Women who are carriers of hepatitis B virus (HBV) may transmit the virus to their infants in utero or at the time of birth (peripartum). Infection of a newborn with HBV carries a very high risk of chronic infection, with the possibility of subsequent chronic active hepatitis, cirrhosis, or liver cancer when carriage persists for decades. Most perinatal transmission of HBV can be prevented by screening pregnant women for hepatitis B surface antigen (HBsAg) and administering hepatitis B immunoglobulin and a course of HBV vaccine to the infants of HBsAg carriers, beginning immediately after birth.
Table 2-5 Effects of Transplacental Fetal Infection
Organism or Disease
Effect of Infection on the Fetus and Newborn Infant
Prematurity
Intrauterine Growth Retardation and Low Birth Weight