1 Epidemiology and Risk Factors of Colorectal Cancer
Epidemiology
Types of Colon and Rectal Cancer
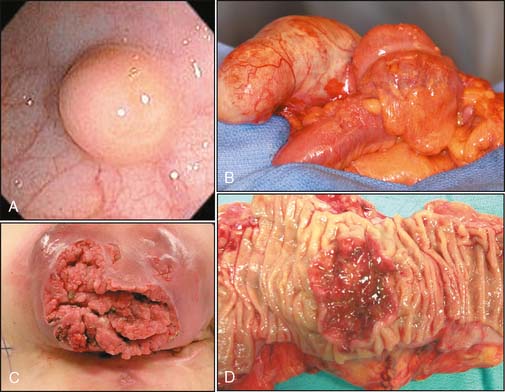
Several types of primary cancer are located in the colon and rectum.1 These include adenocarcinoma, carcinoid tumor, gastrointestinal stromal tumor, lymphoma, and squamous cell cancer of the anus. The majority (95%) of cancers of the colon and rectum are adenocarcinomas or tumors arising from intestinal glands. The epidemiology of this type of tumor is discussed in this chapter. Metastases to the colon and rectum are rare but can occur with melanoma and breast cancer. Carcinoid tumors arise more commonly in the small bowel and appendix, although on occasion these tumors can be identified in the rectum (Fig. 1-1A). Carcinoid tumors develop from gastrointestinal neuroendocrine cells. Gastrointestinal stromal tumors develop from interstitial cells of Cajal and can be found anywhere in the gastrointestinal tract (Fig. 1-1B). Lymphoma may originate in the colon and rectum but is more commonly found in the lymphatic system. Squamous cell cancer of the anus is associated with human papilloma virus infection (Fig. 1-1C).
Incidence of Adenocarcinoma of the Colon and Rectum
Colorectal cancer (CRC) is found throughout the world, but the incidence of this disease varies widely (Fig. 1-2). Developed countries have a higher incidence of CRC than do developing countries, with the highest incidences occurring in Australia, North America, and Northern and Western Europe. The United States has one of the highest rates of CRC in the world. The incidence is almost 10-fold lower in parts of Africa and Asia.2,3
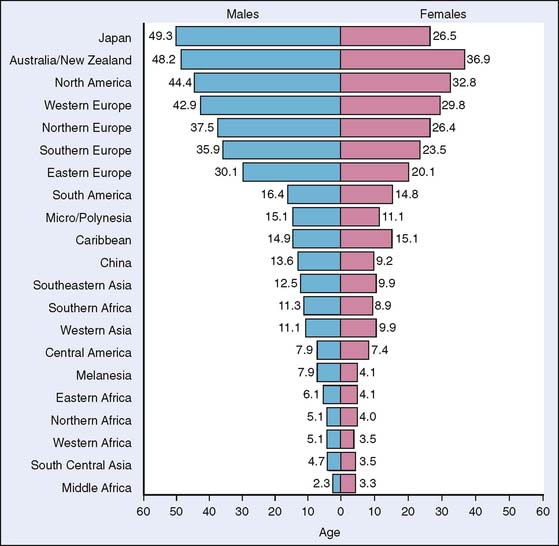
Figure 1-2 Age-standardized incidence rates per 100,000 for colorectal cancer by gender.
(From Parkin DM, Bray F, Ferlay J, Pisani P: Global cancer statistics, 2002. CA Cancer J Clin 55:74–108, 2005.)
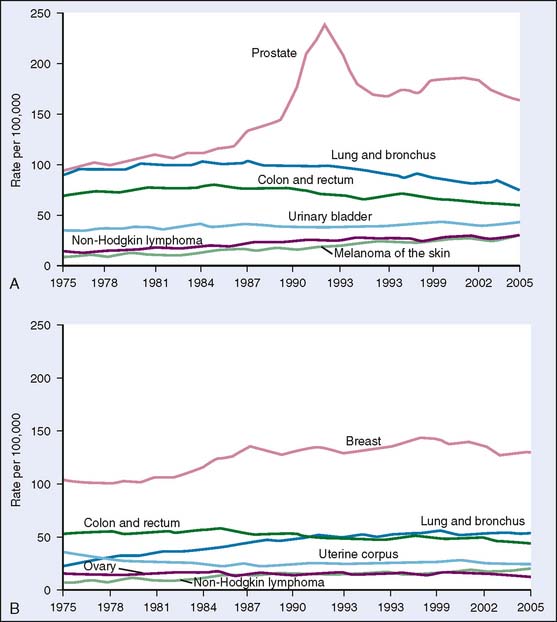
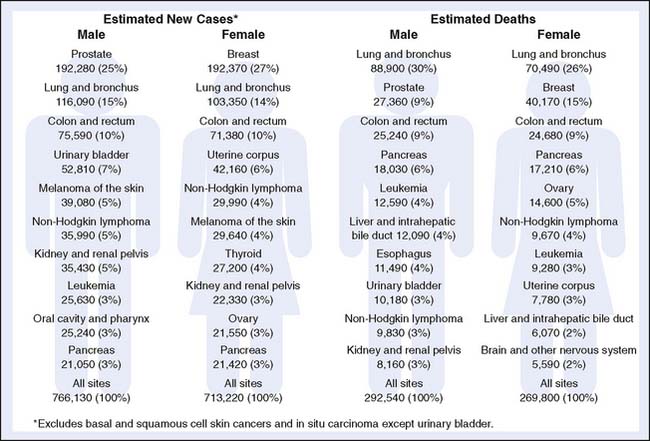
CRC is the third most common cancer in the United States for men and women4,5 (Fig. 1-3). Approximately 147,000 people (76,000 men and 71,000 women) will be diagnosed in 2010 (Fig. 1-4). The incidence of CRC has been decreasing over the last 20 years. In 2004, the reported incidence of CRC was 48.2 per 100,000, whereas in 1985 the reported incidence was 66.3 per 100,000. This decline is believed to be related to an increase in screening for CRC (detection and removal of colorectal polyps),4,5 although changes in lifestyle may also play a role.
Stage at Time of Diagnosis
There are several historical colorectal staging systems, including the Dukes and Astler-Coller systems. The most widely used staging system is the TNM system of the American Joint Committee on Cancer (AJCC).6 In this system, the four stages are based on the depth of invasion of the primary tumor (T), lymph node status (N), and distant metastasis (M) (Table 1-1 and Box 1-1). Approximately 39% of colon and rectum cancer cases are diagnosed while the cancer is still confined to the primary site (localized stage or stage I/IIa), 36% are diagnosed after the cancer has spread to regional lymph nodes (stage III) or directly beyond the primary site (stage IIb), 19% are diagnosed after the cancer metastasized (distant stage or stage IV), and for 5% the staging information is unknown.5 The most common site of metastasis for stage IV CRC is the liver.
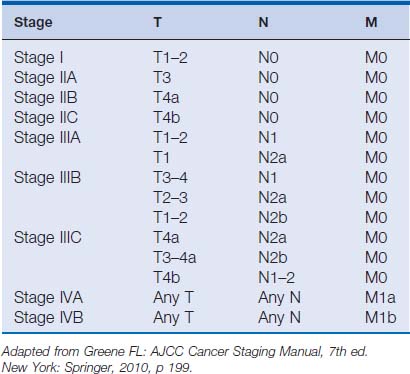
Box 1-1 American Joint Committee on Cancer TNM Classification of Colorectal Cancer
| Primary Tumor (T) | |
| T0 | No evidence of primary tumor |
| T1 | Tumor invades submucosa |
| T2 | Tumor invades muscularis propria |
| T3 | Tumor invades through muscularis propria into pericolorectal tissue |
| T4a | Tumor penetrates the surface of the visceral peritoneum |
| T4b | Tumor directly invades or is adherent to other organs or structures |
| Regional Lymph Nodes (N) | |
| N0 | No invasion of regional lymph nodes |
| N1a | Invasion into one regional lymph node |
| N1b | Invasion into two to three regional lymph nodes |
| N1c | Tumor deposits without invasion into regional lymph nodes |
| N2a | Invasion into four to six regional lymph nodes |
| N2b | Invasion into seven or more regional lymph nodes |
| Distant Metastasis (M) | |
| M0 | No distant metastasis present |
| M1a | Single distant metastasis |
| M1b | Multiple distant metastasis |
In recent years, a greater proportion of CRC has been diagnosed at earlier stages.7 This shift reflects the trend toward increased and improved screening. Gross and associates demonstrated that when Medicare began to reimburse for screening colonoscopy in 1998, a significantly higher percentage of cancers were diagnosed at an early stage (stage I).8
Location of Primary Tumor
Approximately 30% of CRC is located in the right colon, 10% in the transverse colon, 15% in the left (descending) colon, 25% in the sigmoid colon, and 20% in the rectum (Fig. 1-5). In the past 20 years, epidemiologic studies have shown that the ratio of proximal to distal cancers has been increasing.9–12 This is due to a slight increase in proximal cancers and a decrease in cancers of the descending colon and rectum. Older persons are more at risk for proximal lesions (Fig. 1-6), and the aging and growing population has contributed to this increase. The decrease in distal cancers is likely due to improved screening of the sigmoid and rectum.
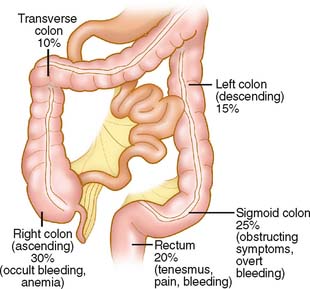
Figure 1-5 Distribution of colon and rectal cancer.
(From Hopkins Colon Cancer website. Used with permission from author, Michael Choti, MD. http://hopkinsgi.nts.jhu.edu/pages/latin/templates/index.cfm?pg=disease1&organ=6&disease=36&lang_id=1. Digestive Diseases Library—Colon Cancer. Sporadic Colon Cancer. Accessed June 24, 2007.)


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


