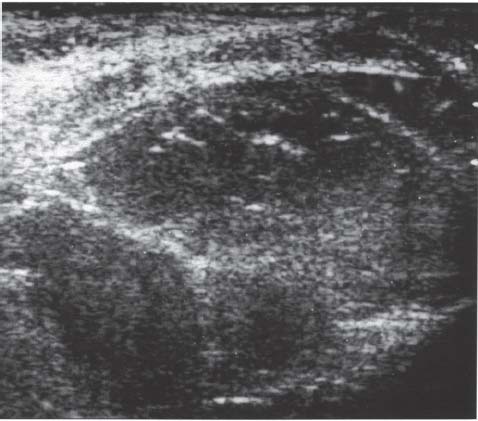
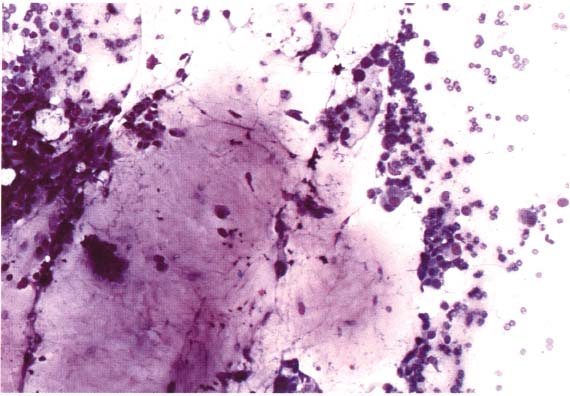
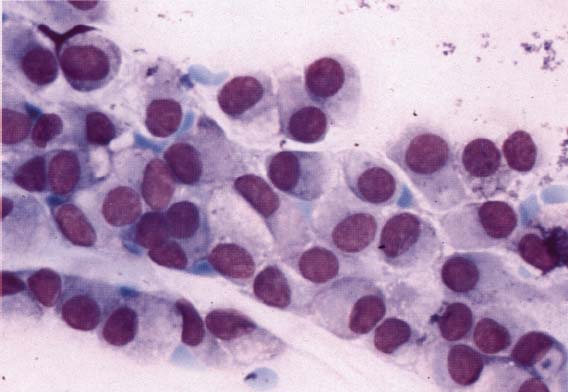
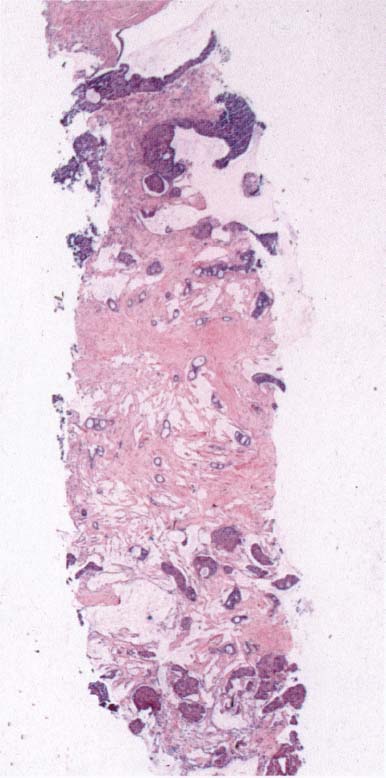
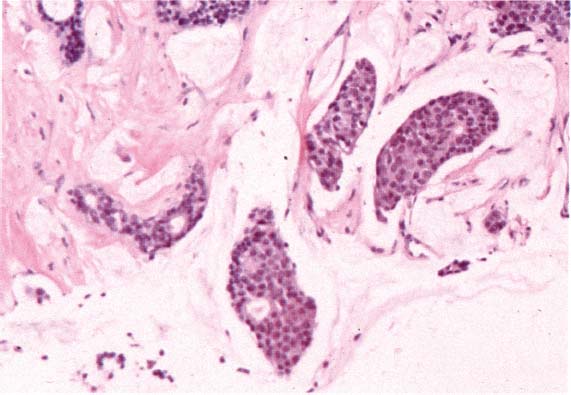
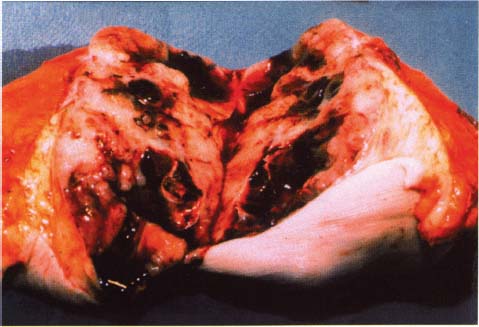
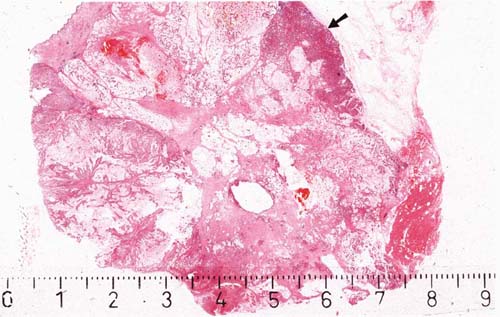
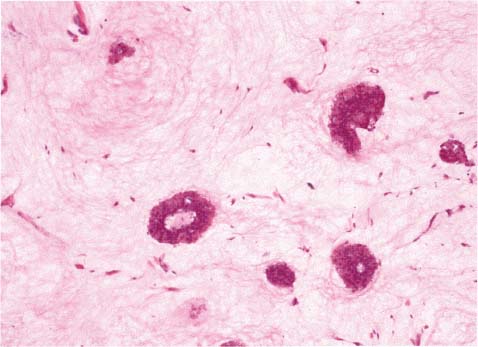
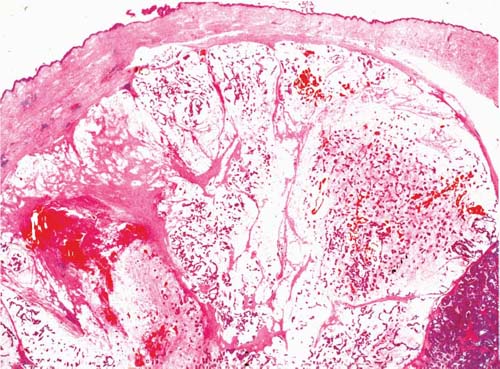
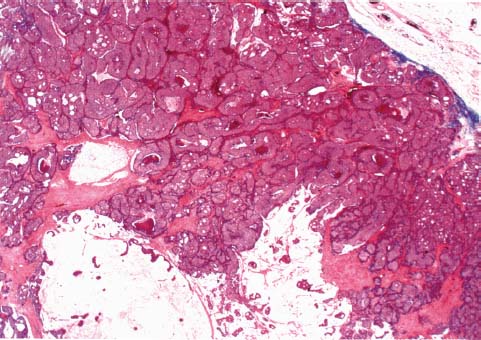
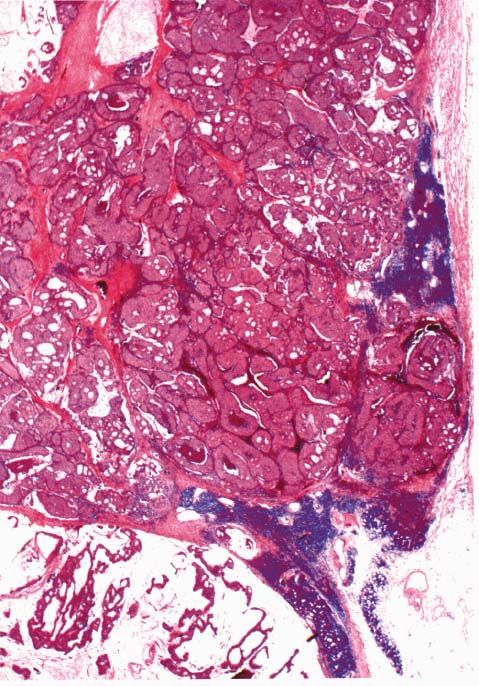
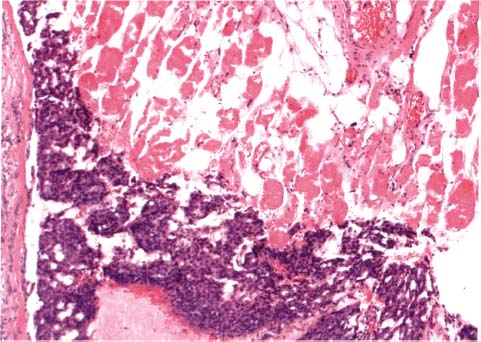
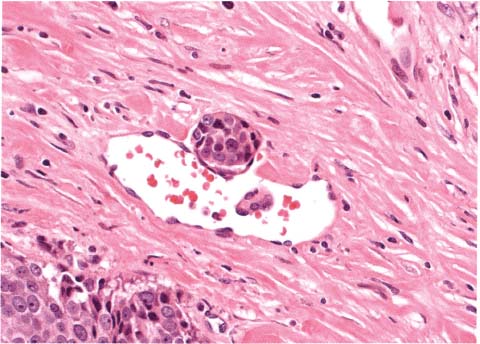
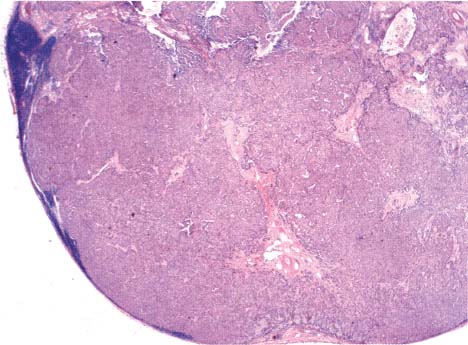
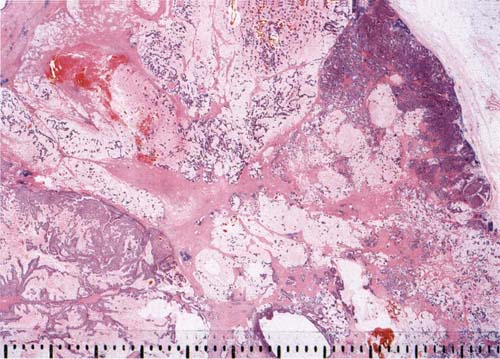
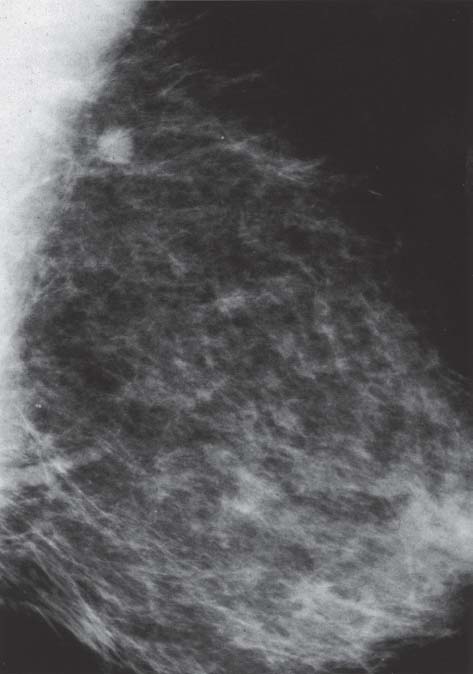
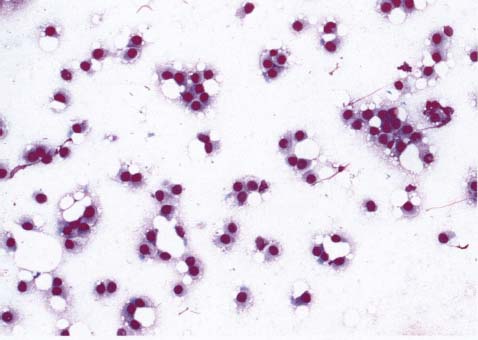
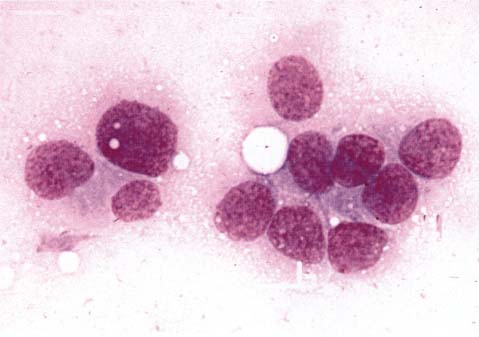
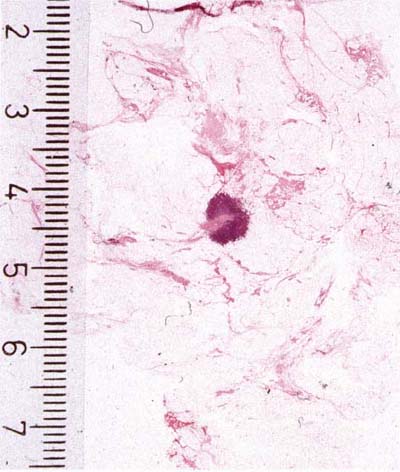
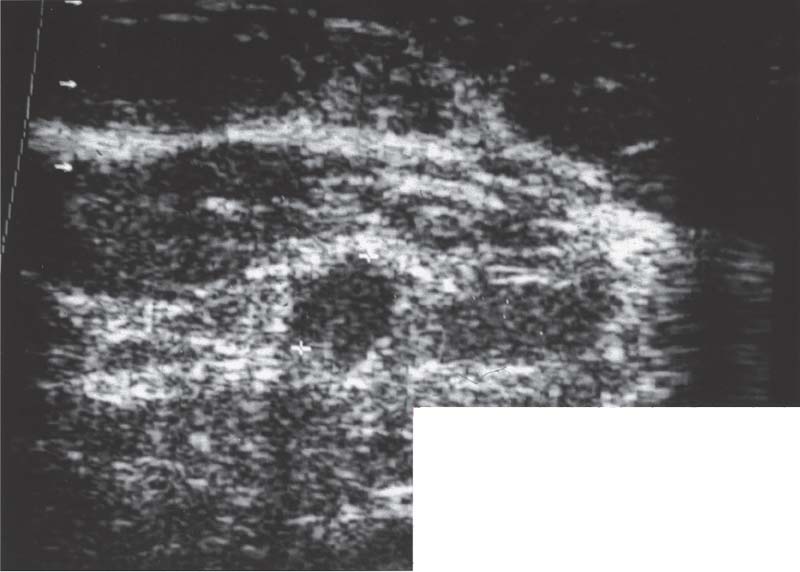
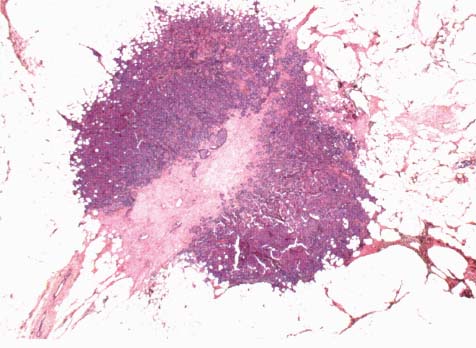
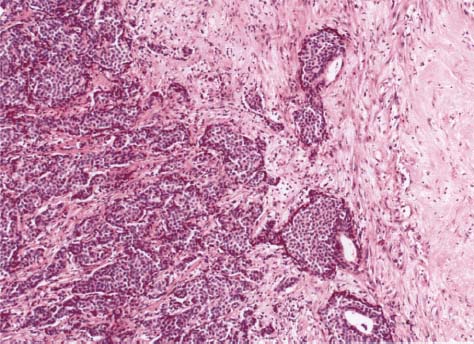
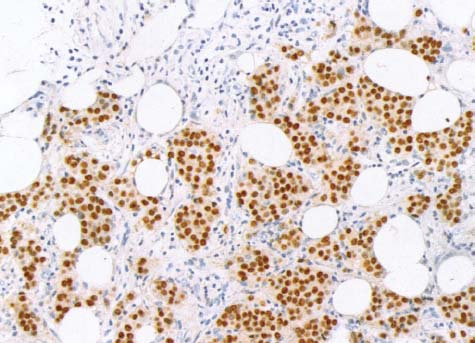
Chapter 10 Case Reports Case 1. The Importance of Intratumoral Heterogeneity This patient was an 80-year-old woman with a large, palpable, rapidly growing lump that filled her right breast (Fig. 10.1.1). Fig. 10.1.1 Mammography and ultrasonography demonstrated a 7 cm large malignant tumor (Figs. 10.1.2 and 10.1.3). Fig. 10.1.2 Fig. 10.1.3 Fig. 10.1.4 Fig. 10.1.5 Fine-needle aspiration biopsy yielded a cellular smear with a mucinous background and cellular atypia (Figs. 10.1.4 and 10.1.5). A definitive preoperative diagnosis of invasive mucinous carcinoma was made by core-needle biopsy (Figs. 10.1.6 and 10.1.7). Fig. 10.1.6 Fig. 10.1.7 Mastectomy was performed and a large tumor with a partly hemorrhagic cut surface was macroscopically evident (Fig. 10.1.8). On the histologic large section, nearly the entire cut surface could be seen (Fig. 10.1.9). Almost 90% of the tumor exhibited the typical picture of mucinous carcinoma with groups of well-differentiated tumor cells floating in a large amount of mucin (Fig. 10.1.10). However, an area (about 20 × 10 mm) of more solid tumor tissue was also evident. Fig. 10.1.8 Fig. 10.1.9 Fig. 10.1.10 Fig. 10.1.11 Fig. 10.1.12 The solid part of the tumor was clearly different from the mucinous component. The cells were poorly differentiated and formed solid nests with central necrosis (Figs. 10.1.11 and 10.1.13). The pattern corresponds to a poorly differentiated, grade III ductal carcinoma. Fig. 10.1.13 The grade III component of the tumor infiltrated the pectoralis muscle (Fig. 10.1.14). Lymph vessel invasion was verified (Fig. 10.1.15), and the cancer had metastasized to one of the nine examined lymph nodes (Fig. 10.1.16). Fig. 10.1.14 Fig. 10.1.15 Fig. 10.1.16 Conclusions Although the tumor fulfilled the criteria for mucinous carcinoma (grade I tumor with a mucinous pattern in 90% of the histologic picture), it did not follow the natural history typical of mucinous carcinomas. The outcome will be determined by the minor grade III component. A thorough postoperative work-up should include a search for evidence of intratumoral heterogeneity. Fig. 10.1.17 Fig. 10.1.18 (the same as 9.32) Case 2. Breast Carcinoma of Limited Extent (Unifocal Tumor) A malignant breast lesion was detected by mammographic screening in a 56-year-old asymptomatic woman (Fig. 10.2.1). Ultrasound-guided fine-needle aspiration biopsy (FNAB) yielded a cellular smear without myoepithelial cells and with a large number of noncohesive epithelial cell groups (Fig. 10.2.2). The epithelial cells exhibited moderate atypia (Fig. 10.2.3). The preoperative cytologic diagnosis was malignant breast tumor. The large histologic section (Fig. 10.2.4) demonstrated that the 7-mm tumor was unifocal invasive ductal carcinoma with an in situ component. Fig. 10.2.1 Fig. 10.2.2 Fig. 10.2.3 Fig. 10.2.4 Fig. 10.2.5 The tumor clearly showed a central fibrotic area resembling a needling artifact; however, the lesion was present on ultrasound before the aspiration was performed (Figs. 10.2.5 and 10.2.6). The tumor was intermediately differentiated (Fig. 10.2.7), and the tumor cells were estrogen-receptor positive (Fig. 10.2.8). The patient has been followed for 4 years and the tumor has not recurred. Fig. 10.2.6 Fig. 10.2.7 Fig. 10.2.8

Case Demonstrations
Only gold members can continue reading. Log In or Register to continue


Full access? Get Clinical Tree


