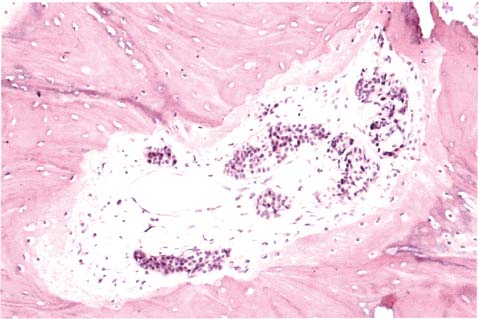
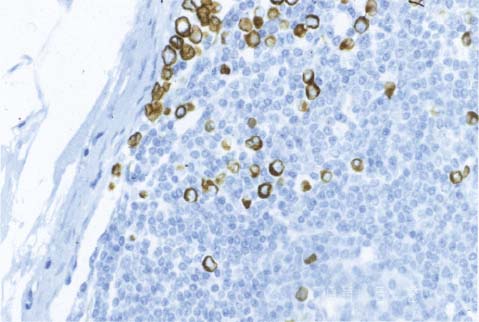
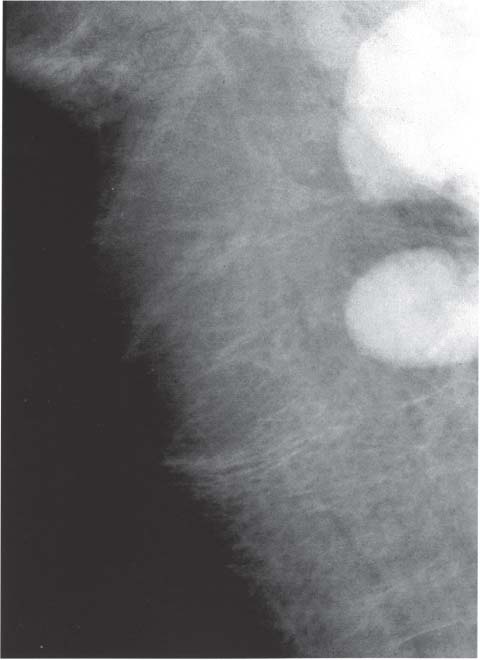
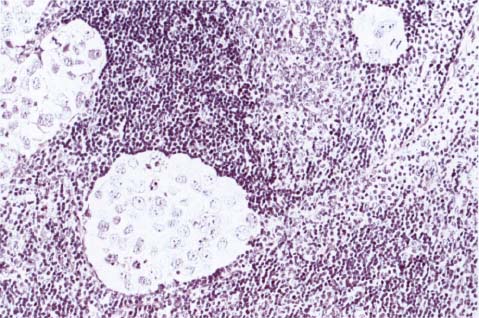
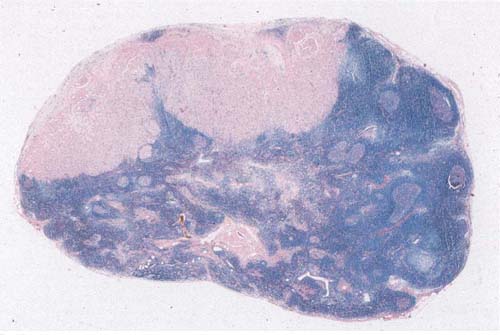
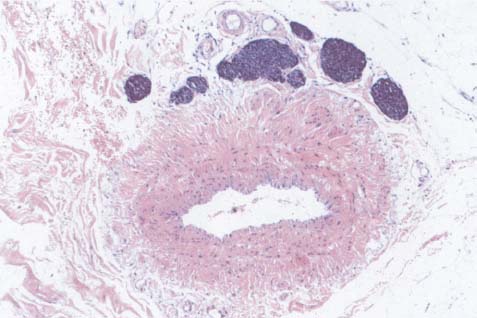
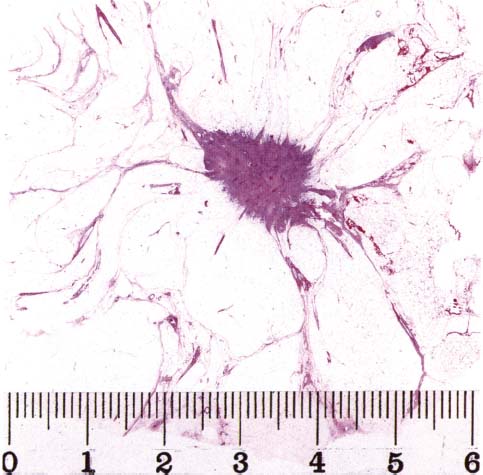
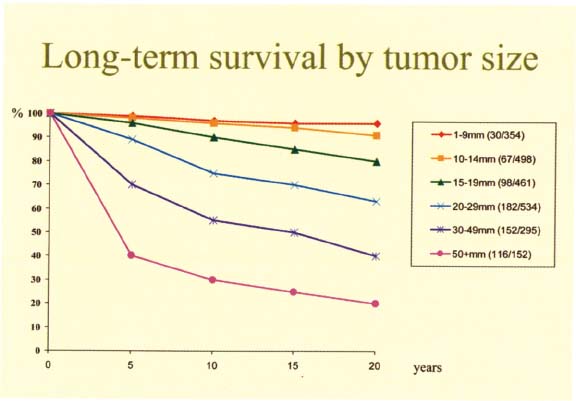
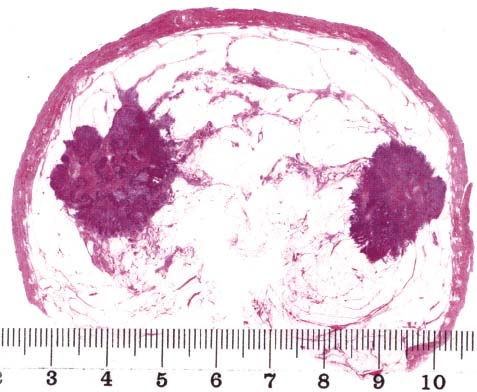
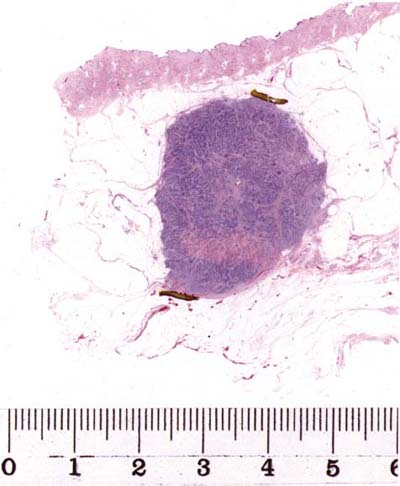
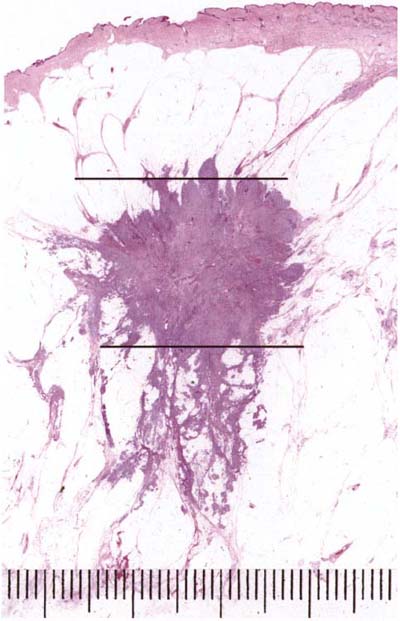
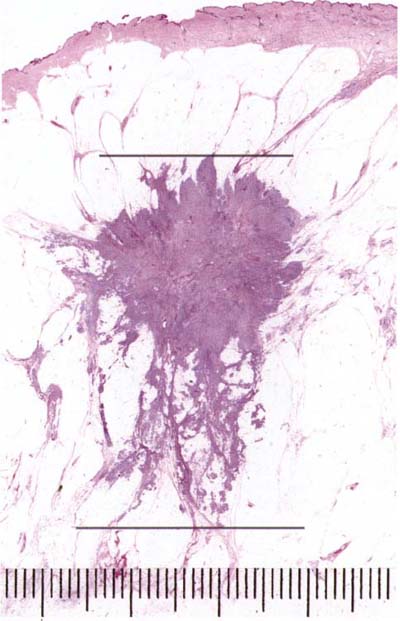
Chapter 9 Assessment of the Most Important Prognostic Factors Histologic typing of breast carcinomas is an important prognostic factor. However, most invasive tumors belong to the category of ductal, not otherwise specified (NOS) carcinomas. This large and prognostically heterogeneous tumor group needs to be stratified using morphologic-prognostic factors. Assessment of these factors is recommended not only for cases of ductal NOS carcinomas but also for all cases of breast carcinomas. The presence of distant metastasis is the most powerful prognostic factor (Fig. 9.1). Fig. 9.1 Fig. 9.2 Fig. 9.3 Fig. 9.4 Fig. 9.5 Fig. 9.6 The presence of metastasis in axillary lymph nodes (Figs. 9.2 and 9.5) is also a powerful prognostic factor and important for therapeutic decision-making. The presence of more than three involved nodes and periglandular infiltration are additional negative prognostic factors. The clinical importance of micrometastases (less than 2 mm) is questioned. The first target of lymphatic spread, the so-called sentinel nodes, may be used as an indicator of the presence of axillary lymph node metastases. Peritumoral or intratumoral vascular invasion (Fig. 9.6) usually indicates that metastases are present in the lymph nodes. Fig. 9.7 The next most powerful prognostic factor is the size of the tumor, defined as the largest diameter of the largest invasive focus. Most of the measuring systems accepted by oncologists (e.g., TNM classification) determine the tumor size on macroscopic examination. The macroscopic size of the largest invasive focus correlates very closely with both the mammographic size and the tumor size as measured by ultrasonography. These methods all evaluate the central body of the tumor, which is a parameter representative of tumor cell mass and which correlates with patient survival (Fig. 9.8). A histologic large section taken in the plane of the largest tumor diameter provides medical documentation of the tumor size (Fig. 9.7), allowing retrospective and reproducible measurement. Comparison of mammographic, ultrasonographic, and macroscopic tumor size is essential when assessing the histologic size of the tumor. In cases of round or oval tumors (Fig. 9.10) the comparison is relatively easy and usually without discrepancies. In cases of stellate tumors, however, the tumor body should be measured histologically without the extensions; otherwise, the histologic size becomes disproportionately larger as compared with the mammographic or ultrasonographic measurements or macroscopic size. The extensions contain a relatively low number of tumor cells, and they do not represent a prognostically important aspect of the tumor. In cases with more than one clearly formed tumor body (Fig. 9.9), the size of the largest tumor is measured separately from the others. Fig. 9.8 (reproduced from reference no. 4 with permission of the publisher) Fig. 9.9 Fig. 9.10 Fig. 9.11 The tumors on Figures 9.10 and 9.11 are not the same size, although if the extensions are measured and included, both tumors would measure 30 mm. The correct way to assess tumor size histologically is demonstrated in Figure 9.12. This can be compared with the erroneous assessment shown in Figure 9.13. Fig. 9.12 Fig. 9.13 Fig. 9.14 Measurement of the area including all the invasive and in situ tumor foci provides another parameter, the extent of the tumor. It is measured in two dimensions as distances between the most distant tumor cells, irrespective of whether the cells are in an in situ portion of the tumor, in a body of an invasive tumor or in its extension, or within a lumen of a lymph vessel. The category of breast carcinoma of limited extent has been defined as a tumor having no invasive carcinoma, in situ carcinoma, or lymphatic emboli farther than 1 cm from the edge of the dominant mass. This category of breast carcinomas is an appropriate candidate for breast-conserving surgery. On the other hand, in cases of extensive breast carcinomas (Fig. 9.14) with a greater distance between invasive tumor foci, a seemingly clear margin free of tumor may be created between two invasive or in situ foci. This may represent a risk for insufficient surgical intervention and local tumor recurrence. Routine use of the technique of large histologic sections (see Chapter 8) is essential for assessing the extent of breast diseases. Fig. 9.15

Assessment of the Most Important Prognostic Factors
Only gold members can continue reading. Log In or Register to continue


Full access? Get Clinical Tree


