Introduction
This chapter will provide a broad overview about factitious disorder or factitious disorder imposed on another (i.e., by proxy) to raise awareness about this rare disorder in patients evaluated for possible endogenous Cushing syndrome. It is not the intent of this chapter to provide in depth coverage of this very complicated topic, and the references provide the reader resources for more in-depth information.
Terminology
Factitious disorder (FD) imposed on self (formerly known as Munchausen syndrome) and factitious disorder imposed on another (FDIA) (formerly known as Munchausen-by-proxy) is a psychiatric disorder in which a person takes on the role of a sick person or in the case of by proxy, a caregiver-fabricated illness in a minor, without the intention of external gain (such as time off work or to obtain medication) [ ]. Several terms have been used in the literature to refer to Munchausen by proxy, such as factitious disorder imposed on another, pediatric condition falsification, child abuse in the medical setting, and medical child abuse. The American Academy of Pediatrics states “child abuse in a medical setting” can include physical abuse, medical neglect, and psychological maltreatment [ ]. Roesler and Jenny [ ] are credited with the term “medical child abuse” (MCA), which is defined as a type of child maltreatment in which the child is subjected to “unnecessary and harmful or potentially harmful medical care at the instigation of a caretaker” [ ]. The hallmark of MCA is a child undergoes evaluation for possible medical diagnosis based primarily on a caregiver’s report of symptoms, which exposes the child to unnecessary, invasive, and harmful tests and procedures and is associated with significant morbidity and mortality [ ]. The caregiver may falsify or exaggerate the signs and symptoms of an illness or may fabricate and cause the presenting signs and symptoms. The emphasis is on the child as a victim of abuse and not the mental status or motivation of the caregiver who is responsible for causing the signs and or symptoms. In FD or MCA, patients or a caregiver of a child may begin with fabricating symptoms and/or medical symptoms and may escalate to interference with medical investigations (simulation) or actively making themselves or their child ill (induction) [ ].
Factitious disorder versus malingering
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) lists factitious disorder as “deceptive behavior in the absence of external incentives” and is subclassified as “factitious disorder imposed on self” or “factitious disorder imposed on another,” or “malingering” [ ]. The motivation for factitious disorder (FD) or factitious disorder imposed on another (FDIA) (referred to as MCA in this chapter) is the patient or perpetrator seeks medical attention and emotional support in their role as a sick patient. Malingering is distinct from FD because external gain is the primary motivation of the individual. Malingering entails intentional falsification or grossly exaggerated physical or psychological signs or symptoms for personal gain such as financial incentive (e.g., Social Security disability claims, legal settlements, civil litigation, or worker’s compensation), obtain prescription medications, evade military duty or incarceration or stand trial, or obtain time off from employment [ , ]. Malingering by proxy involves a caregiver fabricating illness in a child (or the proxy may be an animal or vulnerable adult) or coaching their child to feign symptoms for external gain for the caregiver, such as long-term financial support associated with caring for a sick child or other incentives as listed above. Reports of malingering by proxy are rare in the literature, although this may be an underrecognized problem [ , ]. A literature review of malingering by proxy reported cases in humans in which the motive was financial (i.e., litigation for monetary gain, exploitation) and in animal cases, seeking to obtain medication was the motivator. Reports in the literature estimate a malingering rate in medical practice of approximately 40% of adults undergoing evaluation for Social Security disability [ ]. DSM-V advises that clinicians should consider malingering in situations where there is a medicolegal context; a discrepancy between the patient’s clinical or biochemical findings and the stated symptoms; lack of compliance with diagnostic evaluation or adherence to the prescribed treatment, frequent requests for early refill for medications with the potential for abuse, or in persons with an antisocial personality disorder [ ].
Diagnosis of factitious disorder or medical child abuse
The diagnosis or FD or MCA may be for either a single or recurrent episodes. In FD or MCA, the patient or the caregiver of a child, fabricates, exaggerates, simulates, or actively induces illness to convince the HCP that medical attention is warranted. Patients or caregiver of a child provide inconsistent, selective, or misleading information in the health history and may be reluctant to allow the HCP access to all outside medical records [ , ]. FD or MCA—related illnesses commonly reported in literature include apnea, anorexia or feeding disorders, attention deficit hyperactivity disorder, learning disabilities, immunodeficiency, celiac, Gaucher disease, central nervous disorders, dystonia, complex regional pain syndrome, and renal disorders [ ]. Adults or caregivers may exaggerate healthcare issues or lie about medical history or symptoms or reinterpret trivial findings. Symptoms may be induced by the use of medications (e.g., insulin, sedatives, emetics, salt, warfarin, or laxatives), poisons, contamination of their or their/their child’s specimen collected for testing (i.e., add blood to a urine specimen, introduction of feces or other contaminant to a wound or intravenous line), report false temperature or blood pressure reading(s) by tampering with the measurement, or physically manipulate parts of the body (e.g., using heat, cold, pressure, scratching, forced immobilization) [ ].
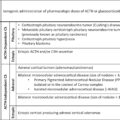
Reports of endocrine-related diagnosis of FD or MCA include surreptitious administration of hormones (i.e., catecholamine injections mimicking pheochromocytoma, thyroid hormone administration mimicking thyrotoxicosis, insulin administration mimicking insulinoma, or glucocorticoid administration mimicking noniatrogenic Cushing syndrome), frequent hypoglycemic episodes (e.g., sulphonylureas or insulin administration), and hypernatremia dehydration [ , , ].
Characteristics of patients with FD include female preponderance, unmarried, middle aged (typically 30–40 year old), comorbid mental health issues (i.e., depression, anxiety, somatoform and factitious disorders), and contact with the medical field (medical-related occupation or family/friends in medical field) [ , ]. Mortality is difficult to estimate; however, death from complications of the (provoked) interventions and suicide have been reported [ ]. Medical child abuse affects males and females equally, the median age at diagnosis is between 14mos and 2.7yrs, and siblings of victims of medical child abuse are at increased risk of abuse [ ]. In MCA, perpetrators are most often: female and the victim’s mother, married, a history of obstetric problems, comorbid mental health issues (e.g., depression, personality disorder), contact with the medical field (medical-related occupation or family/friends in medical field), and history of maltreatment in childhood. The mortality rate of MCA is estimated at between 6% and 10%, with children under 2 years of age at highest risk [ ]. It is generally thought that the prevalence of FD or MCA is underestimated due to the focus on the literature on unusual or dramatic presentations [ ]. Nurses, social workers, and support staff involved in the care of the patient or caregiver and child can contribute to the assessment of possible FD or MCA by reporting and documenting their observations and interactions with the patient, caregiver, and child.
The term “Munchausen by Internet” has been reported [ , ] where individuals or parents of a child create fatalistic stories of illness in online support groups, chat rooms, and publicly accessible blogs to gain attention. A case report series of caregiver-fabricated illnesses in children describes how access to online blogs provided information to supplement the standard procedures used to evaluate MCA in child protection investigations [ ]. Patterns of behavior noted in the blogs included exaggeration and misrepresentation of the patient or child’s symptoms, deception, contradiction of physician statements and medical findings, frantic quest for answers, false reports of severity of the patient or child’s prognosis, visual images (sometimes graphic), “us-vs.-them” theme regarding relationship with health care team, and fundraising activity [ ].
Factitious CS (FCS) or factitious CS imposed on another (FCSIA)
Factitious CS is a rare form of FD or MCA that may present with varied clinical and biochemical findings and is often a diagnostic challenge. Many CS symptoms are nonspecific (i.e., similar to many medical conditions associated with obesity) therefore it is not uncommon for a diagnosis to be delayed or underdiagnosed. Patients or caregivers of children may search the internet (aka “Dr. Google”) or social media sites to find answers to why they/their child are experiencing weight gain and other related symptoms and may deliberately exaggerate or fabricate symptoms of CS with the impression that CS is a “fixable” cause of a weight gain problem. Also, glucocorticoids are prescribed for many different medical conditions such as inflammatory disorders (e.g., asthma, rheumatoid arthritis, inflammatory bowel or skin diseases) and prolonged exposure may result in iatrogenic Cushing syndrome. The morbidities associated with long-term use of supraphysiologic doses of exogenous glucocorticoids are well-known to health care providers (HCP). However, sometimes symptoms associated with glucocorticoid us can be unexpected, for example if the amount of glucocorticoid the patient takes is greater than prescribed (e.g., excessive use of topical steroids) or if the patient does not reveal the use of glucocorticoid to the HCP. Rarely, iatrogenic CS results when the patient or caregiver independently decides to take/give glucocorticoids and does not disclose this information to their/their child’s HCP for the purpose of obtaining medical evaluation and/or treatment without any obvious material gain. This condition is known as FCS or FCSIA, since endogenous CS is not the etiology, rather iatrogenic CS that is induced by the patient or caregiver and hidden from their HCP. FCS or FCSIA may also occur when a patient or caregiver exaggerates or fabricates symptoms of CS or manipulates laboratory tests to produce false results [ ].
FCS or FCSIA is rare, accounting for less than 1% of all CS cases [ ]. A literature review of 23 patients with FCS reported patient characteristics were primarily female (82%), median age 37 years, history of psychiatric disorders (57%), and contact with the medical field (43%) [ ]. However, mental health disorders are also prevalent in patients with Cushing syndrome, so this is not a distinguishing feature of FCS or FCSIA. The medical history provides important clues, similar to what is reported in patients with FD or FDIA. For example, the patient or caregiver of a child reports numerous medical evaluation/treatments (including surgeries and hospitalizations) from multiple healthcare providers for both similar and unrelated illnesses, symptoms are reportedly unresponsive to treatment, multiple drug or food allergies reported, and there is access to medical profession through employment or family/friend. Patients or the caregiver of a child typically “doctor shop” to find an HCP who agrees to repeat testing and procedures and decline follow-up with HCP who don’t agree to escalate the work-up or treatment.
Patients with FCS or FCSIA may present with classical signs and symptoms of CS (i.e., weight gain, centripetal distribution of fat in trunk and abdomen, dorsocervical fat pad, moon facies, striae, hypertension, glucose dysregulation). However, cortisol and ACTH levels are suppressed, and if adrenal imaging of the adrenals is performed, may reveal atrophy of the adrenal glands. Oftentimes there are discrepancies between the reported physical symptoms, biochemical, and imaging findings so the diagnosis is not always straightforward. In some cases, high doses of GC may cross-react with cortisol by immunoassay (however not by LC-MS/MS). Chronic intermittent use of GC may confound the diagnostic evaluation [ ]. FCS or FCSIA may be mistaken for ACTH-independent CS in cases of intermittent use of GC. In other cases of chronic or intermittent GC use, the cortisol and ACTH levels are low or within normal range, it may be mistaken for ACTH-dependent CS. Diagnosis may be difficult and require numerous invasive tests and procedures.
Biochemical findings may provide important clues for suspicion of FCS or FCSIA, such as low cortisol levels in urine and serum without symptoms of adrenal insufficiency or discrepancies between serum and urine cortisol levels. Also, low serum corticotropin, 17-hydroxyproogesterone, progesterone, dehydroepiandrosterone sulfate, and 17-hydroxypregnenolone in the setting of normal or high serum cortisol are consistent with FCS or FCSIA [ ]. Hypopituitarism has been reported after chronic administration of high-dose glucocorticoids [ ]. It is important to use a laboratory that provides a reliable ACTH assay since the performance of the immunoassays at low concentrations may skew the interpretation of results [ ]. Proper handling of the ACTH specimen (on ice, processed promptly) is also crucial for accurate results. Also, several factors can affect the cortisol immunoassay including heterophile antibodies, cortisol-binding globulin deficiency, hook effect, and cross-reacting corticosteroids [ ].
Screening for oral contraceptive use is important because estrogen-containing compounds (or mitotane) increase cortisol-binding globulin and since serum assays measure total cortisol, higher rates of false-positive postovernight dexamethasone test have been reported [ , ]. Medical conditions that may affect gut transit time (e.g., chronic diarrhea, celiac) and alter the absorption of dexamethasone or medications that alter the metabolism of dexamethasone through the CYP 34A could result in false positive overnight dexamethasone test results. Also, screening for drugs that may give falsely elevated urine-free cortisol results (e.g., carbamazepine, fenofibrate, synthetic glucocorticoids, licorice, or carbenoxolone or chewing tobacco (via inhibition of 11B-HSD2), or excessive fluid intake (>3 L/day) is useful [ ]. Imaging studies are typically not useful since a normal adrenal CT does not rule out ACTH-independent CS (i.e., primary pigmented adrenal nodular disease); pituitary MRI findings of a microadenoma do not confirm ACTH-dependent CS since incidentalomas are found in up to 20% of healthy individuals [ , , , ].
It is crucial for the patient or caregiver to provide access to all prior medical records to review. Red flags in the medical records include atypical symptomology, inconsistencies in the patient or child’s medical history/report of symptoms, patient or caregiver of a child repeatedly not satisfied with prior medical evaluation or treatment, patient/child does not respond to treatment, seeking numerous evaluations by various medical subspecialties (“doctor shopping”), numerous surgeries or hospitalizations for similar or unrelated illnesses, multiple food or drug allergies, reported symptoms and signs that are not observed independently. Self-inflicted skin lesions have also been reported in FCS characterized by constant picking of the skin often leading to chronic skin infections [ , ]. A primary concern for the HCP is to not miss a treatable cause for the patient or child’s symptoms, however over-investigating or treatment not in line with good medical practice, may unintentionally cause harm.
Box 5.1 lists medical history red flags for FD or MCA and Box 5.2 clinical findings in FCS and FCSIA.
Box 5.1
Medical history red flags for FD or MCA
Inconsistencies in report of symptoms and clinical findings.
Atypical symptomology.
“Doctor shopping”—evaluations by multiple endocrinologists and other medical subspecialties.
Symptoms are reportedly unresponsive to treatment.
Repeatedly not satisfied with prior medical evaluation or treatment.
Numerous surgeries or hospitalizations for similar or unrelated illnesses.
Multiple food or drug allergies.
Health-care related occupation or access family member or friend in health-care occupation.
History of depression or personality disorder.
In MCA the perpetrator has a history of obstetric complications, childhood maltreatment, or relationship abuse.
Box 5.2
Clinical findings in FCS or FCSIA
Discrepancy between serum and urine cortisol levels.
Marked variability or suppression of urine cortisol levels.
Low cortisol levels in serum and urine without symptoms of adrenal insufficiency.
Normal or elevated serum cortisol levels with low corticotropin and precursor adrenal hormones.
Elevated urine or serum cortisol level and CT shows atrophic adrenals.
Hypopituitarism with elevated cortisol levels in serum or urine.
Identification of FCS or FCSIA is critical since it can lead to inappropriate and potentially harmful interventions. There are case reports in the literature where patients with FCS or FCSIA underwent inferior petrosal sinus sampling [ ], adrenalectomy [ ], exploratory laparotomy, transsphenoidal surgery [ ], or were identified at postmortem [ ]. Serum or urine testing for synthetic GC use is useful to identify factitious CS (measured by LC-MS/MS); however, it is not always possible to distinguish if the patient has recently stopped taking the GC prior to the diagnostic evaluation [ ].
Cyclic CS is an important differential diagnosis for FCS or FCSIA, which is characterized by cycles of high then normal cortisol levels. It is not unusual in cases of FCS or FCSIA for the adult or caregiver of a child to insist that they/their child has cyclic CS if the initial biochemical testing for CS is negative or inconclusive, and demand continued evaluation and testing. The Endocrine Society’s guidelines for evaluation of CS provide a useful tool for HCP to utilize during their discussion with patients or caregivers about the appropriate steps in a diagnostic evaluation of possible CS [ ]. For a review of cyclic CS, refer to Chapter 3 . Also, nontumorous functional hypercortisolism (formerly known as pseudo-CS) is another differential diagnosis to consider since signs and symptoms are similar to CS, but the etiology of nonneoplastic functional hypercortisolism is typically nonendocrine [ ] (refer to Chapter 5 for a review of nontumorous functional CS).
Management
The provider-patient relationship is altered in cases of FCS or FCSIA, because typically an HCP expects that a patient or parent is telling the truth with the goal of getting appropriate medical evaluation and care to improve their health. False allegations or perceived accusations may further threaten the provider-patient relationship. In FCS and FCSIA harm is caused by the patient’s or caregiver’s behavior and often inadvertently by the responses of medical providers. The adult patient or child may undergo unnecessary investigations, procedures, and treatments, including surgery; or in cases where illness is induced, a potentially life-threatening outcome.
Providers of medical care are mandated reporters when there is suspicion of MCA. Tests for MCA that may be utilized as directed by appropriate child protective services or judicial system include a separation test [ ] or covert video surveillance [ ] of the child. Covert video surveillance has been useful in reported cases of MCA; however, it is labor-intensive and before it is put in place the child protective services, the medical management team, nursing, security, and risk management teams must coordinate. In addition, some hospitals/states/jurisdictions may require a court order. Once child protective services completes an evaluation and submits recommendations to the appropriate legal authority, a court may order temporary removal of the parent from the child’s bedside. During the period of separation, the clinical staff caring for the child documents any change in the child’s condition in the medical record.
When working with adults or parents of children with FCS or MCA, a team-based nonconfrontational approach is best. The team should include the physician, nurse, social worker, and mental health counselor to discuss the diagnosis with the patient or caregiver/parent team. In some situations, a review of the case with the legal team of the medical practice or health care institution may be warranted prior to meeting with the patient or caregiver. Emphasis is on providing help to the patient/child and giving assurance that the team is open to continuing to offer medically appropriate care. Even with “supportive confrontation” the patient or caregiver of a child may feel humiliated and seek care elsewhere, become defensive and deny the diagnosis, escalate their behavior, or file a formal complaint [ ]. It is beyond the scope of this chapter to address appropriate steps involved in cases of suspected MCA. If an HCP has concerns regarding possible MCA, contacting child protective services is required.
Evidence-based recommendations for the management of FCS and FCSIA are limited. Appropriate medical interventions include taper or discontinue unnecessary medications (initiate stress dose of glucocorticoids with a taper if exogenous steroid use was involved), assess safety, social work or psychiatric referral, and a low threshold for referral to appropriate services such as child protection team or law enforcement. It is important for an HCP to ensure accurate medical record documentation of details of encounter(s), a detailed medical evaluation, as well as the factors that raise HCP’s concern for possible FCS or FCSIA in the medical record [ ].
Related posts:
 Endogenous Cushing’s syndrome: Causes and genetics
Endogenous Cushing’s syndrome: Causes and genetics
 Identification of Cushing’s syndrome (CS) and its history from Harvey Cushing to today
Identification of Cushing’s syndrome (CS) and its history from Harvey Cushing to today
 Cushing syndrome in pediatrics: From molecular pathogenesis to therapeutic management
Cushing syndrome in pediatrics: From molecular pathogenesis to therapeutic management
 Cushing syndrome in pregnancy
Cushing syndrome in pregnancy
 Adrenal tumors causing Cushing syndrome: Genetics, molecular advances, diagnosis, and treatment
Adrenal tumors causing Cushing syndrome: Genetics, molecular advances, diagnosis, and treatment
 Surgical issues for a patient with Cushing’s syndrome: Techniques, complications, and recovery
Surgical issues for a patient with Cushing’s syndrome: Techniques, complications, and recovery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


