Introduction
Due to their strong antiinflammatory and immunosuppressive actions, glucocorticoids (GCs) are one of the cornerstone treatments for the first-line therapy of various inflammatory and autoimmune disorders. However, notwithstanding their efficacy, long-term GC therapy presents numerous challenges on account of its wide range of side effects, some of these being hyperglycemia, hypertension, osteoporosis, and increased propensity to develop infections. To optimize patient outcomes, it is vital to achieve a balance between the drug’s therapeutic effectiveness and the management of the above adverse effects.
This chapter discusses iatrogenic Cushing’s syndrome, GC biosynthesis, the drug’s mechanism of action, and the most common uses of GCs while also examining the use of GCs in the therapeutic management of postchemotherapy as well as of asthma and joint and rheumatic diseases. Furthermore, the various adverse impacts affecting GC users are analyzed, while a relatively new tool for the calculation of GC administration is briefly discussed, the tool’s purpose being to minimize side effects caused by overdosing. Finally, emphasis is placed on the importance of safe and effective withdrawal of GC therapy via a gradual dose tapering procedure, so as to reduce the likelihood of adverse outcomes.
Exogenous (iatrogenic) Cushing syndrome
Cushing syndrome (CS) is defined by a chronic elevation in plasma cortisol levels that is not attributable to a physiological cause. It was originally reported by Harvey Cushing [ ]. Exogenous CS is a condition caused by the prolonged use of GCs, which are used for a wide variety of medical diseases ( Table 4.1 ). GCs can be administered orally and intravenously (iv), for example, methyl prednisone, prednisone, and dexamethasone, or locally by being applied to the skin, to the respiratory system, to the digestive tract, and to the joints. Excessive use of GCs can lead to endocrine and metabolic, myo-skeletal, cardiologic, dermatologic, neuropsychiatric, ophthalmologic, and immunologic adverse events.
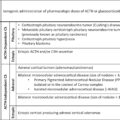
Table 4.1
Clinical uses of GCs.
Modified from Liu D, Ahmet A, Ward L, Krishnamoorthy P, Mandelcorn ED, Leigh R, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol 2013;9.
| Medical field | Diseases |
|---|---|
| Allergic reactions and respiratory system |
|
| Endocrinology |
|
| Gastroenterology |
|
| Dermatology |
|
| Rheumatology |
|
| Hematology |
|
| Opthalmology |
|
| Other uses |
|
Glucocorticoids
GCs, steroid hormones produced by the adrenal cortex, are tightly monitored by the hypothalamic-pituitary-adrenal (HPA) axis. These hormones execute crucial roles in regulating numerous essential processes, including metabolic balance, cell growth, inflammation, immune function, development, and reproduction. Apart from GC action, these synthetic compounds exhibit mineralocorticoid properties. Mineralocorticoids play a crucial role in regulating water and electrolyte balance by exerting specific effects on ion transport by renal tubular epithelial cells [ ]. Due to their lipophilic properties, GCs can easily diffuse through cellular membranes to perform their physiological functions.
In the mid-19th century, Thomas Addison observed that when such symptoms as muscle degeneration, weight loss, unaccustomed skin darkening, and chronic fatigue arose in his patients, they derived benefit from extracts of the adrenal medulla [ ]. This condition today is identified as Addison’s disease. It was in 1946 that the biochemist Edward Calvin Kendall achieved isolation of four steroidal substances from adrenal extracts, which he subsequently named compounds A, B, E, and F. Compound F was cortisol [ ].
Glucocorticoid regulation
The production of GCs by the adrenal gland is regulated by the hypothalamic-pituitary-adrenal (HPA) axis. Under basal unstressed conditions, GCs are secreted into the bloodstream following the circadian rhythm. This hormone pattern features morning peak levels in humans (around 8:00:00 a.m.). HPA axis activity is strongly affected by chronic physiological stress (for instance, disruption to the immune response) and emotional stress. Stimulation of the HPA causes secretion of corticotropin-releasing hormone (CRH) and arginine vasopressin (AVP) from the hypothalamus paraventricular nucleus (PVN), upon which they bind to CRH-R1 and V1B pituitary gland receptors, respectively, resulting in secretion of adrenocorticotropic hormone (ACTH) from the pituitary. Subsequently, ACTH acts on the adrenal gland to secrete GCs, for example, cortisol, into the circulation [ ]. The main effect of ACTH is to stimulate synthesis and secretion of cortisol, as there is minimal storage of steroids in the adrenal glands [ ].
The HPA axis undergoes negative feedback via secretion of GCs through various mechanisms. GCs bind to glucocorticoid receptors in the hypothalamus and the pituitary gland, causing repression of CRH, CRH-R1, and proopiomelanocortin (POMC), the latter being an ACTH prohormone [ ]. Moreover, GCs activate negative feedback loops against the HPA axis by releasing endocannabinoids from CRH neurons, which suppresses glutamate release from the presynaptic excitatory synapses [ ] as well as via release of γ-aminobutyric acid (GABA) via CRH neurons.
Glucocorticoid biosynthesis and mechanism of action (MOA)
Biosynthesis of GCs takes place in the mitochondria located in the zona fasciculata and zona reticularis of the adrenal gland. As mentioned above, ACTH then travels through the bloodstream to the adrenal glands, stimulating cholesterol conversion into pregnenolone, the precursor to all steroid hormones. Via a chain of enzymatic reactions, conversion of pregnenolone into GCs is achieved, primarily cortisol in humans. This pathway involves multiple steps of hydroxylation and oxidation, regulated by enzymes like 21-hydroxylase and 11β-hydroxylase, constituting a multienzymatic process called steroidogenesis [ , ].
Once released into the bloodstream, GCs are carried by transportation proteins, such as corticosteroid-binding globulin (CBG) and albumin. CBG has stronger affinity with GCs and binds around 80%–90% of them [ ]. It is noteworthy that during infection, several proteases, such as neutrophil elastase, aiming CBG, leading to release of GCs [ ]. Albumin affinity with GCs is less, around 10% [ ]. These proteins bind to GCs and maintain them in an inactive state.
Due to their lipophilicity, GCs easily diffuse through cell membranes where they perform multiple actions. However, the main regulator of GC activity are the enzymes 11β-hydroxysteroid dehydrogenase-1 (11β-HSD1), and 11β-hydroxysteroid dehydrogenase-2 (11β-HSD2).
GCs’ effects are exerted via both genomic and nongenomic mechanisms: the genomic actions encompass their interaction with the glucocorticoid receptor (GR), the latter being a part of the nuclear receptor group of transcription factors.
The process starts when GCs bind to GR, upon which they are activated and subsequently translocate in the nuclear compartment. In the nucleus, the hormone-receptor system attaches to particular DNA sequences, namely, glucocorticoid response elements (GREs). Once they bind, this can either stimulate or inhibit the expression of specific genes, thereby controlling the biosynthesis of proteins that govern various biological functions such as development, metabolism, inflammation, immune response, and homeostasis. GCs have been found to regulate 10%–20% of all gene expression in the cell. Genomic effects usually take time to manifest, as they involve gene transcription and protein synthesis. The variety of responses to GC signaling is partly attributed to the presence of multiple GR isoforms, which can form different homo- or heterodimeric complexes, each with distinct DNA binding properties and transcriptional profiles. In addition, GR can influence gene synthesis indirectly by interfacing with other transcription factors, thereby expanding the range of GC effects. Genomic action involves several steps, requiring time—typically 4–6 hours (the minimum being 30 minutes)—before clinical effects are observed. These mechanisms highlight the intricate nature of GC signaling and its broad physiological impact.
The nongenomic effect occurs when the mechanism of action does not depend on corticosteroid ligand with cell nucleus. Nongenomic actions of GCs and GRs occur rapidly involving neither transcription nor protein synthesis. These acts involve actions exerted on membrane lipids, modifying their physicochemical characteristics, and interactions with membrane-bound GRs, likely arising from initiation of alternative transcription, differential splicing, and posttranslational modifications [ , ]. Another membrane receptor, possibly a G-coupled receptor, although binding endogenous GCs with strong affinity, fails to couple the majority GC analogs, including dexamethasone. Achieving the desired effect requires fewer sequential events, which renders it more rapid, typically operating within 15 minutes. The rapid effect is normally achieved only at high doses of GCs, that is, which is equivalent to approximately 100 mg of prednisolone. Thus, treatment with high doses of methylprednisolone exhibits a biphasic response: a swiftly attained, rapid, nongenomic action, sometime afterward followed by a sustained genomic effect.
Glucocorticoid uses
Since their introduction in the 1940s, GCs have become essential for the treatment of numerous endocrine and nonendocrine conditions. In the realm of endocrine disorders, GCs are employed for diagnosing Cushing’s syndrome (primarily using dexamethasone) and are vital for managing adrenal insufficiency and congenital adrenal hyperplasia (CAH) [ ]. For nonendocrine uses, GCs are prescribed on account of their potent properties, which are antiinflammatory and immunosuppressive.
Most of the effects exerted by GCs are antiinflammatory and immunosuppressive and are made possible through their binding with the GC receptor. This interaction gene transcription by either stimulating (transactivation) or else preventing (transrepression) gene expression in both structural cells, including the epithelium as well as inflammatory leukocytes [ , ].
Synthetic GCs are employed for the treatment of a broad spectrum of immunologic and inflammatory disorders, such as chronic obstructive pulmonary disease, chronic inflammatory bowel diseases, rheumatic diseases, asthma, and cancers. Despite significant advancements in medical therapies for inflammatory and malignant diseases, GCs continue to be extensively utilized, highlighting their substantial therapeutic effectiveness, though, sometimes, their use is due to the absence of effective alternative treatments.
Commonly utilized synthetic glucocorticoids in clinical practice
Administration of corticosteroids may be carried out either systemically (whether orally or intravenously) or locally (including directly to the skin, via through the gastrointestinal tract, in the joints, in the eyes, or else via the respiratory tract) [ ]. A more rapid antiinflammatory effect is generally achieved by means of systemic administration given that corticosteroids spread rapidly throughout the organs. A wide range of systemic corticosteroid substances are accessible on the market, and every single one features difference in action period, potency, and the ratio of mineralocorticoid to GC properties. All GCs (including endogenous and synthetic) bind to and activate the glucocorticoid receptor (GR) with varying potencies and possess different pharmacokinetic and pharmacodynamic properties. While many GCs can also activate the mineralocorticoid receptor (MR), they do so to different extents. These differences influence both the efficacy and the therapeutic applications of the corticosteroid.
Prednisone is among the main utilized systemic corticosteroid. It is primarily utilized for its antiinflammatory and immunosuppressive properties due to its high GC activity and relatively low mineralocorticoid activity. Due to its short half-life, oral administration, and wide dosing options, prednisolone is usually the preferred GC for chronic treatment. Experts suggest administration of prednisolone in the morning, as it has lower risk of HPA suppression [ ]. Methylprednisolone has the same efficacy in GC activity as prednisone and prednisolone although less mineralocorticoid activity. Thus, it may be favored due to its ability to minimize mineralocorticoid events (such as water retention) [ ].
Although the mineralocorticoid activity of dexamethasone is minimal, its potency is much higher and its duration of action is longer as compared to prednisone and prednisolone. However, on account of the drug’s high potency, prolonged use may result in acute HPA axis suppression. Dexamethasone is commonly used as a dynamic test, assisting with differential diagnosis between endogenous Cushing’s syndrome and adrenal incidentaloma [ ]. Compared with hydrocortisone, prednisolone and dexamethasone are much more efficacious against antiinflammatory activity. It is consequently most frequently used for short-term administration in exceptionally critical conditions. In addition, its prolonged duration of action renders it inappropriate for day-to-day medication (Deshmukh, 2007).
Betamethasone is a synthetic corticosteroid whose action is very similar to that of dexamethasone.
Among the least potent GCs are cortisone and hydrocortisone ( Table 4.2 ). Due to the fact that they exert mineralocorticoid as well as GC activity, they are commonly favored for the treatment of adrenal insufficiency patients. Fludrocortisone, possessing far greater mineralocorticoid potency by comparison with its GC effects, frequently replaces aldosterone for individuals with Addison’s disease and among patients suffering from the classic salt-wasting type of congenital adrenal hyperplasia [ ].
Table 4.2
Pharmacological properties of most common GCs. Potency is determined with cortisol as reference value 1.
Modified from Chapter Glucorticoids with Isabelle Bourdeau.
| Steroids | Half-life (min) | Duration of action (hours) | GC potency | MR potency | Replacement dose (mg) |
|---|---|---|---|---|---|
| Glucocorticoids | |||||
| Hydrocortisone (cortisol) | 80 | 8–12 | 1.0 | 1.0 | 20 |
| Cortisone | 30 | 8–12 | 0.8 | 0.8 | 25 |
| Prednisone | 60 | 12–36 | 4.0 | 0.3 | 5 |
| Prednisolone | 200 | 12–36 | 4.0 | 0.3 | 5 |
| Methylprednisolone | 200 | 12–36 | 5.0 | 0 | 4 |
| Triamcinolone | 200 | 12–36 | 5.0 | 0 | 4 |
| Betamethasone | 300 | 36–72 | 25.0 | 0 | 0.6 |
| Dexamethasone | 300 | 36–72 | 30.0 | 0 | 0.75 |
| Fludrocortisone | 240 | 12–24 | 10.0 | 125 | 2 |
Glucocorticoid use in pregnancy
During normal pregnancy, a state of physiologic hypercortisolism occurs due to the stimulation of the maternal HPA axis. However, this physiologic elevation of cortisol concentrations during pregnancy does not result in the clinical manifestations associated with Cushing’s syndrome [ , ]. Given that maternal GCs cannot cross the placenta, the fetus is generally shielded from these hormones. In addition, placental enzyme 11β-hydroxysteroid dehydrogenase type 2(11-β-HSD) metabolizes cortisol and prednisolone into inactive forms. Thus, the prednisolone ratio between maternal and fetal plasma is 10:1. On the contrary, betamethasone and dexamethasone are poorly metabolized by placental 11-β-HSD. As a result, the mother-to-fetus concentration ratio of these GCs is approximately 1:1. Understanding this concept clarifies why preference is given to treating women in pregnancy with prednisone, prednisolone, and methylprednisolone. If a therapeutic effect on the fetus is needed, betamethasone and dexamethasone should be considered [ ].
Despite to the protective mechanism of placental 11-β-HSD, there are instances when fetuses exposed to antenatal steroids may experience low birth weight, intrauterine growth restriction, or oral clefts. It is recommended that high doses of steroids be avoided during the first trimester to minimize these risks [ ].
Glucocorticoid potency
The potency of various GCs is often represented as a prednisolone/prednisone equivalent dose, a standard rooted in prednisone’s early clinical use as the first synthetic GC. The scientific foundation for these equivalence values is not robust: nevertheless, they are employed as practical therapeutic guidelines in clinical settings. It is essential, on the contrary, not to adhere to these ratios too strictly. The above equivalent doses are established by comparing the potency of the GC at issue to the potency of prednisolone. For instance, given that hydrocortisone’s conversion factor is 4, 200 mg of hydrocortisone will be analogous to 50 mg of prednisolone (200 mg/4 = 50 mg). Importantly, one must be aware that the equivalent dosing concept is applicable primarily to doses of prednisone that are below 100 mg. Beyond this dosage, nongenomic effects have greater significance, so that they can diverge substantially from the classical genomic effects, thereby strongly influencing therapeutic outcomes.
Glucocorticoid dosing
As mentioned above, GC dosing can vary widely for the administration of inflammatory and autoimmune diseases. Based on diagnosis, clinical indications, and treatment goals, different dosing regimens are employed. We separate GC dosages into five categories, as follows: low dose, intermediate dose, high dose, very high dose, and pulse therapy. These doses are presented analytically in Table 4.3 .
Table 4.3
Definitions of conventional terms for glucocorticoid doses.
This table is modified from Peinado-Acevedo JS, Rivera-Bustamante T, Rivera J, Santamaría-Alza Y. Balancing inflammation and adverse effects of glucocorticoids in clinical practice. Rev Colomb Reumatol ;498–510.
| Dose | Definition | GC receptor saturation |
|---|---|---|
| Low dose | ≤7.5 mg/day of prednisone or its equivalent | <50% |
| Intermediate dose | >7.5 and ≤30 mg/day of prednisone or its equivalent | 50%–100% |
| High dose | >30 and ≤100 mg/day of prednisone or equivalent | 50%–100% |
| Very high dose | >100 mg/day of prednisone or equivalent | Over 100%. At this dose, complete receptor saturation is assumed. It is believed that alterations in pharmacodynamics, synthesis, and expression of new receptors may come into play |
| Pulse dose | ≥250 mg/day of prednisone or its equivalent for 1 or a few days |
In clinical practice, a low dose is often used for rheumatoid arthritis along with disease-modifying antirheumatic drugs (DMARDs) and extremely low doses (prednisone <5 mg or its equivalent) to maintain remission in RA patients with adverse events [ ]. Moderate doses can be used to treat acute gout attacks [ ]. High doses and very high doses are crucial for the management of severe conditions and of acute flair-ups (along with immunosuppressive drugs, such as cyclophosphamide) in systemic arteritis.
Pulse therapy involves administering high doses over a short period to manage severe disease flares or for induction therapy in connective tissue disorders [ ]. A standard pulse dose is 1000 mg of methylprednisolone intravenously over 3 days. Edel et al. stress the fact that physicians frequently express concern regarding the risk of GC pulse therapy [ ]. This study estimates that the complication rate regarding GC pulse therapy is approximately 35 cases per century. Among the most common events that can be caused by pulse therapy are diastolic blood pressure elevation, hyperglycemia, hypertension, flushing, headache, chest pain, and heart rhythm disorders such as palpitations and tachycardia [ ]. Therefore, pulse therapy should be carefully considered and used when it is necessary and clinically reasonable.
Postchemotherapy uses of GCs
Corticosteroids number among the most frequently prescribed drugs in oncology. Corticosteroids (CSs) are indicated for cancer-related palliative care to manage refractory symptoms and for use in oncological emergencies [ ]. The four primary roles of corticosteroids used in oncology are the following: managing palliative symptoms due to their antiinflammatory properties, exerting anticancer activity in particular hematological malignancies, making available supportive prophylaxis during therapies specific to cancer, and exerting immunosuppressive actions for the handling of immune-related adverse events (irAEs) caused by immunotherapy [ , ].
GCs and symptoms related to cancer
Corticosteroids are extensively utilized in cancer care due to their ability to alleviate inflammation- and edema-caused symptoms, as well as their antiemetic, antiallergic, and anticancer properties. Their uses include exerting anticancer effects particularly in lymphoid hematological malignancies, providing an extra weapon for cancer-specific therapies (including immune-related adverse events), managing refractory cancer symptoms, and treating noncancer-related comorbidities. Corticosteroids are frequently preferred in oncological emergencies due to their rapid action and wide availability.
Brain metastasis (symptomatic)
Corticosteroid therapy is essential for managing symptoms associated with elevated edema and intracranial pressure caused by brain lesions. Radiotherapy-induced intracranial edema can also be effectively managed by GCs [ ]. In addition, clinical manifestations like nausea, headache, visual disturbances, and mild neurological issues can also be alleviated by GCs [ , ]. In cases of leptomeningeal carcinomatosis, corticosteroids might provide only limited relief. Dexamethasone seems to be the most potent drug [ ]. The initial dose typically ranges from 4-16 mg daily in accordance with the severity of the clinical presentation. However, no definitive guidelines currently exist for dose tapering, thus, it is advised to gradually decrease the dose throughout a period of 2 weeks or more in patients with severe symptoms [ ].
Cancer-related dyspnea
CGs can improve the management of such pulmonary adverse events as drug-induced interstitial lung disease (DILD) and radiation pneumonitis when they arise.
GCs are also used to alleviate palliative symptoms of carcinomatous lymphangitis and tumor-induced airway obstruction, despite the current insufficient evidence as to their efficacy in clinical use [ ]. Overall, certain patients may be prescribed GCs, particularly those experiencing cancer-related breathlessness and mainly when dyspnea occurs due to inflammation [ ].
Nausea, vomiting, and bowel obstruction
The concept of adding dexamethasone to antiemetic regimens likely arose from the observation of reduced rates of chemotherapy-induced nausea and vomiting (CINV) in patients receiving steroids as a component of their antineoplastic treatment. GCs commonly employed in conjunction with serotonin 5-HT3 receptor antagonists and neurokinin-1 receptor antagonists when moderately or highly vomiting-induced medical regimen is administered [ , ]. A meta-analysis of 32 RCTs involving 5613 patients demonstrated superiority of dexamethasone versus placebo in both rapid and delayed onset nausea [ ]. Corticosteroids are frequently employed in conjunction with antiemetic drugs in cases of malignant intestinal obstruction caused by peritoneal carcinomatosis to help reduce inflammation and edema, thereby improving gut function and relieving such symptoms as nausea and vomiting. This combination can also enhance the patient’s overall well-being and quality of life(QoL) by addressing both the mechanical and inflammatory components of the obstruction.
Use of GCs in spinal cord compression and pain from bone metastasis
In cases of pain related to vertebral metastases and acute neural deterioration, which is frequently observed in metastatic epidural spinal cord compression, corticosteroids (CSs) have proven to be a cornerstone of pharmacological treatment. They provide analgesic effects, diminish vasogenic spinal cord edema, reduce inflammation, and significantly enhance short-duration neurological function; they also alleviate pain by inducing the production of prostaglandin E2 and vascular endothelial growth factors(VEGF) [ ]. Dexamethasone is the most commonly utilized corticosteroid for these conditions. Recommended dosage varies from 8 to 16 mg iv per day gradually reducing over 2 weeks [ ].
Fatigue and overall quality of life
In late-stage diseases, GCs provide relief for fatigue and better QoL, as shown by some RCTs [ , ]. These RCTs demonstrated that dexamethasone (4 mg twice daily/14 days) or methylprednisolone (16 mg twice daily/7 days) demonstrates higher potency than placebo in alleviating cancer-related fatigue and in improving QoL.
Oncological emergencies
GCs are employed in numerous oncological emergencies, including superior vena cava, pericardial infusion, hypercalcemia, and acute tumor lysis. The mechanism of action of GCs in the management of hypercalcemia remains unclear. However, they have shown a potent effect in hypercalcemia due to multiple myeloma and lymphoma. In these cases, the preferred GC is prednisone (doses range from 60 to 100 mg once daily). On the contrary, GCs should be avoided in the management of hypercalcemia associated with solid neoplasms as no therapeutic benefits have been observed [ ]. Although the benefit of corticosteroids for the treatment of superior vena cava (SVC) syndrome, pericardial effusion, and acute tumor lysis syndrome is to date unclear, they are frequently prescribed.
Glucocorticoid use in asthma treatment (inhaled and systemic use)
Asthma, a chronic inflammatory disease of the respiratory tract, marked by recurring periods of short breathe, chest tightness, wheezing, and coughing. There is variation in these symptoms’ intensity and frequency among individuals. The episodes are linked to reversible airway obstruction, which can either resolve on its own or with medical intervention. Asthma, a common, noncommunicable pulmonary condition, affects youths and adults. Globally, it is associated with urgent healthcare utilization, reduced quality of life, and mortality. Evaluation of its incidence is challenging due to the variety of characteristics. The goals of chronic asthma management can be categorized into two main areas, as follows: achieving effective control of asthma manifestations and reducing potential danger, like asthma exacerbations, impaired lung function, and medication-related complications[ ]. Synthetic GCs are crucial for asthma treatment, as well as for the antiinflammatory therapy of chronic inflammatory diseases in general [ ].
Regarding asthma, GCs may be administered either orally or via inhalation (inhaled corticosteroids—ICs). These medications reduce airway inflammation and relieve bronchial hyper-responsiveness, leading to significant improvements in symptom severity and lung function [ ]. In addition, they effectively prevent and reduce the frequency of asthma exacerbations.
GC MOA in asthma
As mentioned above, GCs act through binding to the GC receptor and changing its structure [ ]. This structure change leads to repression of proinflammatory factors (transrepression) and enables antiinflammatory factors that have been stimulated by proinflammatory signals (transactivation). More specifically, GCs connect with glucocorticoid receptor and cause activation of the antiinflammatory histone deacetylase 2 (HDAC2). This histone seems to have a major antiinflammatory action. Although the histone’s exact mechanism remains unclear, it seems to reverse the acetylation of histones conducted by histone acetyltransferases (HAT). In conditions of mild or severe asthma or chronic tobacco use, reduced levels of HDAC2 are observed [ , ]. In mild asthma, ICs can restore HDAC2 activity [ ]. In addition, GCR activation promotes mitogen-activated protein kinase (MAPK) phosphatase, inhibiting MAPK signaling. Furthermore, in asthmatic inflammation, the decrease by GCs of the production of major asthma-related interleukins (ILs), including IL-4, IL-5, and IL-13, aids in the reduction in airway inflammation [ ].
GCs impact the airway vasculature and phosphorylation pathways as well as numerous cells and mediators involved in bronchial hyperresponsiveness [ ]. They exert direct inhibition of multiple cell types linked to asthma-related airway inflammation, including airway smooth muscle cells (ASM), mast cells, epithelial cells, eosinophils, macrophages, and T-lymphocytes [ ].
GC structure and clinical characteristics in asthma treatment
Both oral and inhaled GCs are indispensable for the treatment of acute and chronic asthma [ ]. Medications as prednisone and fluticasone are extensively utilized on account due to strong antiinflammatory properties, which help control acute asthma exacerbations [ ]. For instance, the daily use of inhaled fluticasone can significantly reduce the occurrence of acute asthma symptoms. Therefore, depending on the degree and incidence of asthma symptoms, GCs inhaled daily are considered to be the standard of care for asthma management [ , ]. At present, there are eight ICS molecules on the market, each with distinct potency, selectivity, pharmacokinetic and pharmacodynamic characteristics, physicochemical properties, as well as a range of inhaler or formulation options [ ].
Beclomethasone dipropionate (BDP) was among the first inhaled synthetic GCs for the treatment of asthma. Since then, seven other ICSs have received approval, as follows: budesonide (BUD), ciclesonide (CIC), flunisolide (FLU), fluticasone propionate (FP), fluticasone furoate (FF), mometasone furoate (MF), and triamcinolone acetonide (TAA) [ ]. These ICSs are derived from cortisol and have been structurally modified to enhance antiinflammatory effects, improve metabolic stability, and increase specificity for glucocorticoid receptors (GRs) through various chemical modifications.
ICSs currently have approval for use alone or combined with long-acting β2-adrenoceptor agonists (LABAs). Their administration is conducted via either liquid or dry powder aerosols via pressurized metered-dose inhalers (MDIs) or and breath-actuated dry powder inhalers (DPIs) as well as with nebulizers. Smaller particle size inhalers can be advantageous, as particles larger than 5 μm tend to get deposited in the upper respiratory tract, whereas finer particles reach the small airways, enhancing treatment efficacy [ ]. Thus, a careful choice of inhaler device based on particle size and, hence, drug deposition is crucial for patients suffering from asthma [ ].
With the exception of severe asthma cases that cannot be controlled by other means or when ICS are unavailable, oral GCs are not the typical choice for maintenance therapy.
GC use in mild and moderate asthma
Even thought asthma is a chronic inflammatory condition, the Global Initiative for Asthma (GINA) previously recommended the use of short-acting β2-AR agonists (SABAs) alone for step 1 patients [ ]. Patients suffering from mild asthma typically use SABAs depending on their needs, which is based on their perception of the symptoms [ ]. This approach stands in contrast to other steps for treatment of asthma while not addressing asthma’s inflammatory nature. In addition, overuse of SABAs is linked to a higher risk of mortality (GINA Guidelines).
The 2019 GINA guidelines’ recommended treatment for stage 1 asthma disease consists of dual therapy with ICs and formoterol, or ICs and SABA, or ICs/SABA with LABA as needed It is crucial to point out that the use of inhaled corticosteroids causes upregulation of β2-adrenergic receptors, thereby enhancing the effect of long-acting β2-adrenergic agonists.
Thanks to recent research, there have been modifications in the management of mild asthma, with emphasis being placed on the application of ICS/LABA combinations over SABA monotherapy to prevent severe exacerbations and improve treatment adherence. Studies have shown that as-needed use of inhaled combinations like BDP and albuterol, or BUD-FORM, can be as effective as regular ICS use for mild asthma. These combinations reduce the overall exposure to corticosteroids while effectively controlling symptoms and reducing exacerbations. Meta-analyses support these findings, suggesting that single maintenance and reliever therapy (SMART) with ICS/FABA is more effective than as-needed SABA alone. Furthermore, for mild persistent asthma without type-2 inflammation, the benefits of daily ICS use are minimal, highlighting the need for tailored treatment approaches based on patient-specific inflammatory profiles.
GC use in severe asthma
Chronic use of oral corticosteroids (OCS) remains crucial in managing severe asthma due to their unique antiinflammatory mechanisms. In cases of severe asthma, the regular use of oral corticosteroids (OCS) often proves to be the final treatment step after optimizing inhalation therapy. Recently, this empirical approach has been shifting toward more precise, trait-to-treat methods, facilitated by the advent of biologic drugs. Current asthma guidelines recommend progressively increasing GC therapy until optimal symptom control and prevention of exacerbations are achieved. Recent research highlights the importance of biomarkers in predicting dosage responses to GCs. While biomarkers like FeNO are effective in guiding inhaled corticosteroid (ICS) therapy, optimal biomarkers for OCS dosage and duration are still under investigation. Peripheral blood eosinophil counts have shown promise in adjusting OCS therapy, improving symptom control, and reducing exacerbations. Ongoing studies aim to refine OCS titration using various inflammation biomarkers to enhance treatment outcomes. Moreover, gene expression biomarkers in sputum have been identified as potential predictors of OCS response, offering a more precise approach to severe asthma management.
GC use in asthmatic exacerbation
Periods of deterioration of asthma symptoms and reduced lung function are known as acute asthma exacerbations. Exacerbations often initially manifest as asthma, or else they occur in patients with a known diagnosis caused by such triggers as nonadherence to controller medications, allergens, air pollution, bacterial or viral upper respiratory infections, other irritants, or unknown stimuli [ ]. Almost all patients experiencing a significant asthma exacerbation should be administered oral GCs [ ]. The risk for another severe exacerbation within the following 2 weeks may be considerably decreased via a brief course of GCs (e.g., prednisone 40–60 mg/day for 5–7 days) while also reducing the occurrence of severe persistent symptoms that are typically observed at a 2-week follow-up call [ , ]. Alternatively, similar effectiveness to a 5-day use of prednisone (50–60 mg/day) has been shown by administration of oral dexamethasone (12–16 mg) in 1-2 doses [ , ].
IC adverse events
Among the local side effects of ICS are reflex cough, dysphonia, pharyngitis, bronchospasm, and oropharyngeal candidiasis, these being principally on account of the drugs’ local immunosuppressive action. The probability of pneumonia related with ICS use in asthma patients remains unclear, though there is a known increased risk among those with chronic obstructive pulmonary disease (COPD) [ ]. Interestingly, Rank et al. observed that patients who discontinued low-dose ICSs exhibited a notably higher risk of asthma exacerbation in contrast to those who kept on their ICS regimen over a 6-month period [ ].
Systemic side effects are less common with ICSs compared with systemic GCs: these lead to reduced bone density, osteoporosis, growth suppression, HPA axis suppression, glaucoma, cataracts, skin thinning, and bruising. The severity of HPA axis suppression is influenced by the dose, duration, and timing of ICS administration [ ]. We will discuss the systemic adverse effects of GCs administered orally or intravenously in a subsequent chapter.
GC uses in rheumatic diseases and other inflammatory joint diseases
GCs number among the highly potent antiinflammatory treatments employed for management of chronic inflammatory diseases, allergies, and autoimmune conditions such as multiple sclerosis, asthma, rheumatoid arthritis (RA), and systemic lupus erythematosus [ , ]. GCs are regarded as immunomodulatory agents rather than mere immunosuppressants due to their complex interactions with immune cells. Their antiinflammatory effects are primarily accomplished via suppressing proinflammatory cytokines and transcription factors, such as NF-kB and AP-1, while activating antiinflammatory genes including GILZ (TSC22D3) and DUSP-1 [ ]. Despite these benefits, GCs can also induce proinflammatory effects, including NLRP3 expression, which constitutes a major component of the inflammasome. GCs’ impact on the immune system varies according to exposure period: that is, whereas protracted use may result in immunosuppression, short-term use is likely to activate the immune system.
Long-term high-dose GC treatment exerts essential immunosuppressive and antiinflammatory effects for the relief of symptoms among those with chronic autoimmune or inflammatory diseases. However, these benefits are often accompanied by severe adverse effects, sometimes necessitating additional therapies or discontinuation of GC use. For conditions like asthma, topical administration of GCs can mitigate some side effects, but systemic therapy at high doses still poses significant risks. However, efforts to develop “dissociated steroids” involving the transrepression of activated monomeric GR rather than dimer transactivation with the aim of reducing side effects have yet to yield successful alternatives.
Local application of GCs in rheumatic-skeletal diseases
In rheumatic and joint diseases, GCs can be applied orally, intravenously, or intraarticularly. We have discussed previously oral and intravenous pathways. In this segment, we will analyze intraarticular application. Intraarticular GCs should be considered for persistent nonbacterial joint arthritis. There are several factors such as the volume of synovial fluid, arthritis activation, the joint being treated (location, size, weight bearing or nonweight bearing), and the application of arthrocentesis (aspiration of synovial fluid). The choice of dose and injection technique of GC is pivotal for the effectiveness of treatment [ ].
Among other GCs, triamcinolone hexacetonide is noted for its low solubility and prolonged effect [ ]. Although definitive evidence-based recommendations are lacking, it seems prudent to avoid overuse of the treated articulation for a few days, even once pain relief has been achieved. It has been observed that resting the injected joint by using a splint or cast for 3 weeks for nonweight-bearing joints and 6 weeks for weight-bearing joints is beneficial [ ]. There is as yet no alternative to GCs for intraarticular therapy.
Role of GCs in rheumatoid arthritis treatment
Rheumatoid arthritis (RA) is a chronic, inflammatory, symmetric, condition that targets the peripheral joints. Its precise cause remains unknown. Characterized by polyarthritis, the condition typically results in the deterioration of cartilage and bone within the joints. Early treatment of RA focuses on minimizing disease activity and achieving clinical remission. Without appropriate treatment, RA can lead to significant physical disability, such as the risk of joint destruction, which severely impacts daily activities and job performance. In addition, unmanaged RA inflammation is associated with increased risks of cardiovascular diseases, osteoporosis, and certain cancers, such as lymphoma [ ].
In RA and other inflammatory diseases, production of CRH and ACTH is lowered compared with noninflammatory states as a result of permanent stimulation of the HPA axis [ ]. The current hypothesis is that the body lowers cortisol secretion to manage stress and inflammation. It is therefore evident that exogenous GC administration is necessary for the control of RA [ ].
Use of GCs in RA began during the mid-20th century, marking a significant achievement in the management of this chronic condition. Hydrocortisone, which revolutionized the field of treatment options for RA, has greatly helped with symptom relief. By the beginning of 20th century, GCs became the second therapeutic option after nonsteroidal inflammatory drugs (NSAID) [ ]. However, the therapeutic effectiveness of GCs in RA has often been viewed as limited because the positive effects tend to dissipate quickly after discontinuation of the treatment. Meanwhile, other second-line RA treatments, including methotrexate (MTX) and sulfasalazine (SSZ), have been gaining recognition for their strong efficacy, particularly when used in combination.
In 2015, the American College of Rheumatology (ACR) issued guidelines recommending the use of low-dose, short-term GCs for patients who did not reach target disease control despite treatment with disease-modifying antirheumatic drugs (DMARDs) or biological therapies [ ]. The 2021 ACR update further underlined the fact that long-term GC use might result in side effects, featuring increased probability of infections, osteoporosis, and cardiovascular events. More specifically, the ACR 2021 recommendations for treatment of rheumatoid arthritis (RA) underscored the benefit of starting a conventional synthetic DMARD (csDMARD), without using long-term GCs, in patients who were new to DMARDs and who presented with mid-range-to-high disease activity. The latter approach is today strongly recommended in preference to starting a csDMARD with long-term GCs [ ]. For short-term GC use (less than 3 months), it is conditionally recommended a csDMARD be initiated without GCs in newly diagnosed patients. In addition, for patients currently on GCs, the recommendations suggest adding or switching to other DMARDs to achieve target disease control rather than continuing GC use alone. Furthermore, combining DMARDs with or without intraarticular GCs is preferred over using intraarticular GCs alone in patients not meeting treatment targets with DMARDs alone.
Similarly, the recommendations of the 2019 update of the European League Against Rheumatism (EULAR) for management of RA also emphasize the importance of tapering GCs as soon as clinically possible. The guidelines advise clinicians to consider GCs, particularly for initiating or changing csDMARD treatments, but only for short-term use to minimize adverse events. What is critical is to determine how quickly GCs can be tapered and what precisely constitutes “short-term” use, with a strong emphasis on discontinuing GCs within 3 months whenever possible.
Low-dose (less than 7.5 mg prednisone or its equivalent) GCs in combination with DMARDs are commonly used in managing RA. GCs are useful in that they are able to provide a “bridging-therapy” before the therapeutic effects of the slow-acting DMARDs begin to manifest [ ]. Moreover, use of GCs has shown significant improvements in clinical measures and acute phase reactions. Very low doses (namely, less than 5 mg of prednisone or its equivalent) have been effective in maintaining remission with minimal side effects [ ]. A prospective study is currently being conducted to further evaluate the risk-benefit ratio of this approach. Multiple studies have demonstrated that low-dose GCs may exhibit a disease-modifying effect in early RA, with the beneficial effects in joint damage persisting for 4 years, even after a 2-year treatment period with these low doses.
Overall, despite the advances and new therapeutic agents (c/b/ts DMARDS) for treatment of RA, not all patients’ needs are currently being fulfilled. The role of GCs remains essential, especially at the onset of therapy and also when disease flares.
GC use in systemic lupus erythematosus
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder of unknown etiology that can impact nearly any organ system. A hallmark of the disease is the positive value of antinuclear antibodies (ANA) in ELISA method, reflecting significant immunologic dysregulation. Clinically, SLE manifests with a wide variety of symptoms, from moderate joint and skin issues to severe involvement of the kidneys, hematologic system, or central nervous system. Some patients may exhibit only a limited set of symptoms, which can mimic other autoimmune, infections, or hematologic conditions, complicating the diagnostic process further.
GCs are crucial in managing severe manifestations of lupus, particularly in life-threatening situations or when organ viability is at risk. In cases such as renal involvement with acute kidney injury (AKI) secondary to lupus nephritis, diffuse alveolar hemorrhage, thrombotic microangiopathy, and pneumonitis or vasculitic neuropathy, high-dose GCs are often administered. Methylprednisolone at doses ranging from 250 to 1000 mg is typically given for 1–5 days to rapidly control inflammation and prevent further organ damage. This intensive GC therapy can stabilize patients with severe lupus flares and improve their prognosis by mitigating the acute inflammatory response.
GC use in other joint inflammatory diseases
Psoriatic arthritis (PsA) is an inflammatory musculoskeletal condition linked to psoriasis. Firstly believed to be a form of rheumatoid arthritis, it was later identified as a separate clinical entity [ , ]. Historically, the absence of rheumatoid factor (RF) was essential for diagnosis, but it has been observed that over 10% of individuals with uncomplicated psoriasis and up to 15% of the general community may have RF in their serum. In addition, there have been instances of positive cyclic citrullinated peptide (CCP) antibodies in PsA patients. Consequently, expression “usually seronegative” arthritis is more appropriate for describing PsA [ , ].
Although intraarticular GCs are sometimes administered, it is essential to avoid injections administered via psoriatic plaques. For such procedures, triamcinolone, at a dose of 40 mg for large joints and 20 mg for small joints, is normally used. Injecting GCs into tendon insertions must be avoided given the likelihood of tendon rupture, while data supporting the efficacy of this approach are currently lacking.
When managing PsA, oral GCs should be avoided since they may trigger psoriatic flares. In rare cases where patients experience severe flares that are unresponsive to NSAIDs and conventional or biologic DMARDs, may be prescribed. In situations where GCs are necessary for other medical conditions, a collaborative approach to management is essential to mitigate risks.
There are till now no randomized clinical trials specifically evaluating GCs for the management of juvenile idiopathic arthritis. Childhood Arthritis and Rheumatology Research Alliance (CARRA) consensus treatment plans and the 2013 American College of Rheumatology (ACR) guidelines have provided some treatment recommendations [ , ]. Oral GCs are usually administered during the early stage of the disease to maintain the patient’s functionality to perform daily tasks: this approach also applies to children who have not shown effective response to initial therapies. It is important to use GCs sparingly in juvenile idiopathic arthritis to minimize their toxicity.
It is not recommended that routine intraarticular GC injections be administered in osteoarthritis (OA) due to GCs’ short duration of effect (typically about 4 weeks) and potential harmful effects on hyaline cartilage, which possibly accelerates the progression of the disease [ ]. This practice is limited to patients with knee OA who experience mild to severe pain and have contraindications to or have not found relief from other treatments. When used, triamcinolone or methylprednisolone is to be preferred, typically at 40 mg doses, though other formulations such as betamethasone may also be effective. Serial injections, administered every 3 months, are discouraged due to potential negative impacts on cartilage health, although what is the therapeutic value of these effects is as yet unclear.
In summary, GC therapy is essential in managing multiple types of arthritis, like psoriatic arthritis and RA, along with other inflammatory joint diseases. While GCs have shown their efficaciousness in reducing inflammation and alleviating symptoms, their use must be carefully managed to minimize potential adverse effects. For more detailed information about their use, refer to Table 4.4 .
Table 4.4
General use of GCs in rheumatology. Initial dosages (low, moderate, high, very high, and pulse) explained in Table 4.3 .
This table has been modified from .
| Arthritides | Oral dose | IV dose | Intraarticular injection | ||
|---|---|---|---|---|---|
| Low | Moderate | High | Pulse therapy or very high dose | ||
| Gout arthritis | – | b | b | – | b |
| Juvenile idiopathic arthritis | – | a | a | – | a |
| Psoriatic arthritis | – | a | – | – | b |
| Reactive arthritis | – | – | – | – | a |
| Rheumatic fever | – | a | a | – | – |
| Rheumatoid arthritis | b | b | a | a | b |
| Acute calcium pyrophosphate crystal arthritis | – | – | – | – | b |
| Osteoarthritis | – | – | – | – | a |
| Collagen disorders | |||||
| Dermatomyositis, polymyositis | – | – | c | a | – |
| Mixed connective tissue disease | – | a | – | a | a |
| Polymyalgia rheumatica | – | c | – | a | – |
| Sjogren’s syndrome | – | – | a | – | – |
| Systemic lupus erythematosus | – | b | a | a | – |
| Systemic vasculitis | |||||
| In general | – | – | 3 | 1 | – |
(−), Rare use; a, infrequent use; b, frequently used, added to basic therapeutic strategy; c, basic therapeutic strategy.
Adverse outcomes of glucocorticoid therapy
Glucocorticoids (GCs) are widely recognized thanks to their known potent immunosuppressive and antiinflammatory properties, making them a cornerstone in the management of multiple inflammatory and autoimmune conditions. However, it is known that their administration is accompanied by elevated risk for common and severe side effects, this in particular in the case of long-term and high-dose therapy [ , ]. The incidence of short-term symptomatic toxicity is relatively low, and discontinuation for these reasons is uncommon. Moreover, as mentioned, prolonged use and higher dosages create the conditions for great frequency and severity of adverse effects, as detailed in multiple studies [ , ]. The fact is that in spite of more than six decades of clinical use, there are still very limited solid data concerning the toxicities associated with long-term GC therapy, very few systematic reviews and clinical trials having been published that have analyzed high-quality evidence on this topic. Currently, there are merely a few retrospective and observational studies [ ].
Patients on prolonged GC therapy frequently report adverse effects such as weight gain, skin bruising, sleep disturbances, and mood changes, with these symptoms showing a positive correlation with GC exposure. Moreover, more serious adverse reactions associated with GC use include Cushingoid appearance, dyslipidemia, hyperglycemia or diabetes, cataracts, glaucoma, suppression of the HPA axis, osteoporosis and fractures, cardiovascular diseases, myopathy, psychiatric disturbances, immunosuppression, and various gastrointestinal and dermatological issues. Table 4.5 summarizes all the major adverse events of GC use.
Table 4.5
Major AE associated with GC use.
| Major side effects associated with GC use | |
|---|---|
| Endocrinology and metabolism | Adrenal crisis |
| Exogenous (iatrogenic) CS and weight gain | |
| Dyslipidemia | |
| Hyperglycemia | |
| Growth suppression (in children and adolescents) | |
| Myoskeletal | Osteoporosis |
| Osteonecrosis | |
| Myopathy | |
| Cardiovascular | Fluid retention |
| Hypertension | |
| Premature atherosclerotic disease and major CVD | |
| Arrhythmias (atrial flutter and AF) | |
| P.E. and VTE | |
| Gastrointestinal | Peptic ulcer, gastritis, and upper gastrointestinal bleeding |
| Visceral perforation | |
| Steatohepatitis | |
| Ophthalmologic | Cataracts |
| Elevated intraocular pressure-glaucoma | |
| Dermatologic | Acne, hirsutism, facial erythema |
| Skin thinning and ecchymoses | |
| Neuropsychiatric | Insomnia |
| Depression-mania | |
| Psychosis | |
| Memory impartment | |
| Immunologic system | Infections |
| Decreased response to vaccinations | |
Related posts:
 Cushing syndrome in pediatrics: From molecular pathogenesis to therapeutic management
Cushing syndrome in pediatrics: From molecular pathogenesis to therapeutic management
 Endogenous Cushing’s syndrome: Causes and genetics
Endogenous Cushing’s syndrome: Causes and genetics
 Identification of Cushing’s syndrome (CS) and its history from Harvey Cushing to today
Identification of Cushing’s syndrome (CS) and its history from Harvey Cushing to today
 Cushing syndrome in pregnancy
Cushing syndrome in pregnancy
 Adrenal tumors causing Cushing syndrome: Genetics, molecular advances, diagnosis, and treatment
Adrenal tumors causing Cushing syndrome: Genetics, molecular advances, diagnosis, and treatment
 Surgical issues for a patient with Cushing’s syndrome: Techniques, complications, and recovery
Surgical issues for a patient with Cushing’s syndrome: Techniques, complications, and recovery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


