A variety of tumors and tumorous proliferations may involve the spleen, and there are several that are unique to this organ. This chapter focuses on the unique proliferations as well as other neoplastic causes of splenomegaly. Splenomegaly, however, is not restricted to neoplastic causes and may occur with secondary hypersplenism, which may be secondary to autoimmune or para-neoplastic causes, infectious processes, and passive congestion due to other nonneoplastic medical disorders.
PATTERNS OF TUMOROUS SPLEEN PROLIFERATIONS
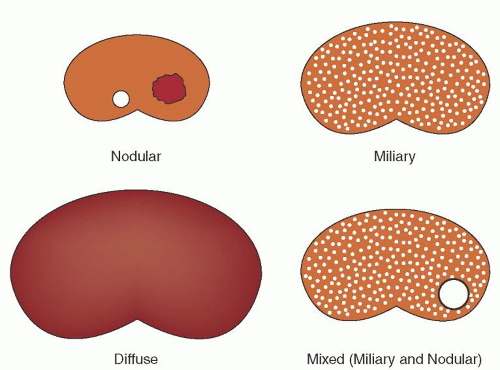
Although splenomegaly is often present with splenic neoplasia, some tumors and tumorous proliferations may be found incidentally in normal-sized spleens during radiologic staging or in spleens removed due to traumatic rupture or incidentally removed during other surgical procedures. The pattern of splenic infiltration may be helpful in the differential diagnosis of splenic tumors and the gross disease patterns tend to mimic histologic patterns (Fig. 66.1 and Table 66.1).1 The most common disease patterns are diffuse, miliary, and nodular disease. Diffuse disease generally results in splenomegaly with complete infiltration of the splenic parenchyma. This often imparts a glassy and homogeneous red appearance to the cut surface of the spleen. This usually is due to obliteration of the normal splenic white pulp by a cellular proliferation of the red pulp. This disease pattern has traditionally been attributed to leukemic infiltration, T-cell lymphomas, and histiocytic tumors. Many of the red pulp proliferations previously considered to be histiocytic, however, have now been shown to represent T-cell neoplasms. The miliary pattern shows small, punctate tan or white areas throughout the cut surface of the spleen. These usually represent expansion of the splenic white pulp, the normal B-cell compartment of the spleen. However, a similar gross appearance may occur with granulomatous infections. The white pulp expansion pattern most commonly occurs in florid reactive hyperplasia and with low-grade B-cell lymphomas. The nodular disease pattern is characterized by one or more distinct tumor nodules in the spleen which may be identified incidentally on imaging studies. These nodules are usually firm and tan or white in cases of large cell lymphoma, Hodgkin disease, or metastatic tumors, and are bloody with a beefy-red appearance in vascular proliferations. Cystic lesions of the spleen may also show a nodular pattern of involvement.
CYSTS AND ABSCESSES
Cysts of the spleen are found in <1% of splenectomy specimens.2 They occur most commonly in men in the third decade of life. They are usually asymptomatic; however, they may cause a splenic mass and be associated with abdominal pain. Splenic cysts may be essentially any size but are on average 10 cm in diameter.3 Splenic cysts may be designated as primary or secondary, also considered true and false cysts, respectively. Both types are usually unilocular, but some small primary cysts are multilocular. Primary cysts are reported to represent approximately 20% of all splenic cysts, but small primary cysts of the spleen are probably underrepresented in older studies and more extensive evaluation of nonparasitic cysts shows that the vast majority are true cysts.4, 5 Primary cysts have a firm, rough, and trabecular cyst wall that shows fibrosis and an epithelial lining on histologic examination (Fig. 66.2). The lining may be of mesothelial or squamous epithelium with the latter probably representing a metaplastic change.6 The epithelial lining of primary cysts may be patchy, with denuded areas present that may simulate a secondary cyst. Primary cysts can be further subdivided into parasitic and nonparasitic types. Primary parasitic cysts related to echinococcal infection (hydatid cysts) are common worldwide, but are uncommon in Western countries. Parasitic cysts are readily identified by the presence of parasite scolices in the cyst contents. Nonparasitic primary cysts appear to arise from congenital inclusions of capsular mesothelium.7 Small multilocular primary cysts of the spleen occurring at the splenic capsule have in the past been mistaken for lymphangiomas.8 Patients with primary cysts may have elevations of CA19-9 and carcinoembryonic antigen.9, 10 Primary cysts are usually treated with splenectomy, and partial resection by laparoscopic methods often leads to recurrence.11, 12
Secondary cysts are reportedly more common, representing approximately 80% of splenic cysts in most studies, but more detailed evaluation can confirm many of these as having a focal epithelial lining and thus they are really primary.4 The true secondary cysts are often associated with a history of abdominal trauma and are probably acquired after hematoma or infection. The cysts are unilocular and usually have a smooth lining. They differ histologically from primary cysts by the complete absence of an epithelial lining, and are thus unlikely to recur even if only partially resected. The cyst wall may contain hemosiderin or calcification.
Some secondary cysts of the spleen may represent resolved abscesses. Multiple small splenic abscesses usually do not develop associated fibrosis with resolution, but larger abscesses are often single and develop a wall of surrounding fibrosis virtually identical to that seen in secondary cysts. Although relatively uncommon, splenic abscesses are most often associated with sepsis or endocarditis. They may also occur following abdominal trauma, including splenic rupture, by contiguous spread of infection from other organs, or in association with functional asplenia in sickle cell anemia.13, 14, 15 Most splenic abscesses are due to polymicrobial infection, but common organisms include Streptococcus, Staphylococcus, Escherichia coli, and Salmonella.16
FIGURE 66.1. Gross patterns of splenic tumor involvement. Nodular tumor infiltrates may form solid firm masses or may be hemorrhagic masses. The miliary pattern shows small punctate white foci that usually correspond to expansions of the white pulp. The diffuse pattern shown is usually associated with massive splenomegaly and corresponds to a red pulp expansion. Mixed patterns may be seen when the spleen is involved by more than one process or when a low-grade lymphoma transforms to high-grade disease.
aMore than one pattern may occur with some diseases.
Partial splenectomy has been used successfully in the treatment of nonparasitic splenic cysts.17
VASCULAR PROLIFERATIONS
Vascular tumors are the most common tumors of the spleen. Vascular proliferations may be diffuse or may form a tumor mass. Peliosis is a rare, diffuse vascular proliferation that is usually an incidental finding occurring in adults.18, 19, 20 It may be associated with hepatic peliosis and may occur with anabolic steroid use, in association with malignancies, and following solid organ transplantation, as well as in patients with hepatic cirrhosis, tuberculosis, and aplastic anemia. Peliosis results in dilated vascular spaces, usually 1 mm or less in diameter, that involve the entire splenic parenchyma (Fig. 66.3). Splenic peliosis appears to be associated with an increased risk of splenic rupture.19, 21, 22
Hemangiomas are benign tumors that are also usually asymptomatic, but may cause splenomegaly, abdominal pain, and hypersplenism.2, 23, 24, 25 Most hemangiomas are localized and form single or multiple tumor nodules that contain cystic blood-filled spaces grossly. These spaces are lined by endothelial cells, and papillary projections may occur in areas with thrombi. The tumor nodules are usually surrounded by fibrosis and may show calcification. Plain abdominal radiographs, computed tomographic scans, and sonograms are nonspecific, but all show discrete solid and cystic masses, often with evidence of calcification.26, 27 Diffuse hemangiomatosis of the spleen is less common, is often associated with systemic hemangiomatosis, results in massive splenomegaly, and may be associated with coagulopathies.28, 29 Diffuse hemangiomatosis differs from peliosis by the presence of intervening fibrosis in hemangiomatosis, which is not a feature of peliosis.
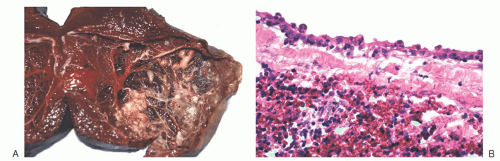
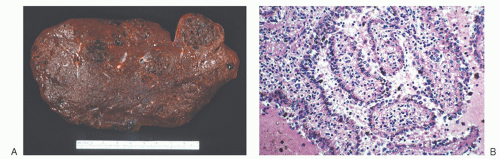
FIGURE 66.2. Primary cysts. A: Primary cyst of the spleen showing a trabeculated inner surface on gross examination. B: The cyst shows an epithelial lining on histologic sections, a feature that is definitional of a primary cyst.
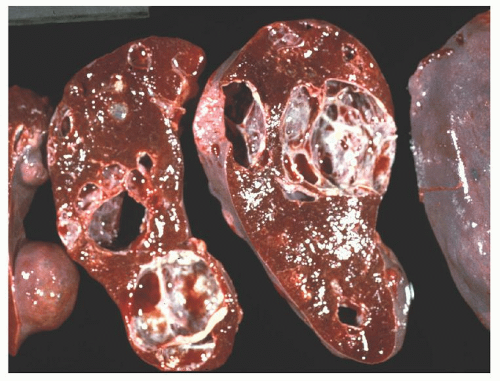
Localized lymphangiomas of the spleen may be difficult to distinguish from hemangiomas or primary cysts, but usually contain proteinaceous fluid rather than the blood of an hemangioma.2, 23, 30 Diffuse lymphangiomatosis may be localized to the spleen, but is usually a systemic process and most commonly occurs in children and young adults with massive splenomegaly.30, 31, 32, 33, 34 The splenic parenchyma is replaced by multiple cysts, up to 3 cm in diameter, imparting a spongy appearance (Fig. 66.4). The cysts are filled with thick pink to brown fluid. Large localized lymphangiomas and lymphangiomatosis of the spleen may be treated with splenectomy.30
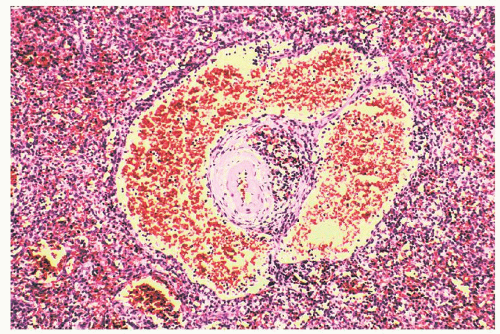
FIGURE 66.3. Splenic peliosis. Peliosis of the spleen shows expanded small vessels that diffusely involve the spleen without forming a nodular mass and without intervening fibrosis.
Although hemangiomas and lymphangiomas of the spleen are similar to those of other sites, there are two unique vascular proliferations of the spleen. Littoral cell angioma is a tumor presumably derived from the normal splenic lining cell, also known as the littoral cell.24, 35 These tumors may occur at any age and usually cause mild to moderate splenomegaly. Many tumors, however, are found incidentally. The tumor forms multiple spongy dark red nodules that can measure up to 9 cm in diameter (Fig. 66.5). Histologically these tumors differ from hemangiomas in that the vascular spaces are lined by plump cells with nuclear enlargement and often show papillary areas and lining cells sloughing into the vascular spaces. The lining cells of littoral cell angioma have a unique immunophenotype, expressing vascular, histiocytic, and dendritic-associated markers CD31, CD68, CD163, and CD21. In contrast to hemangiomas and normal sinus lining cells, the lining cells of littoral cell angioma do not express CD34 or CD8. Most cases of littoral cell angioma are treated with splenectomy without recurrence, but there are two reports of late abdominal and liver metastasis after 4 and 8 years.36, 37 Both cases showed solid foci of clear cells and probably represent littoral cell hemangioendotheliomas.
Sclerosing angiomatoid nodular transformation (SANT) is the other vascular proliferation unique to the spleen.38, 39, 40 To date, SANT has only been reported in adults, usually presenting as an incidental mass, and less commonly with splenomegaly or abdominal pain. It usually forms a single fibrotic nodule that contains vascular spaces, including slitlike spaces, fibrosis with spindled cells, and splenic sinus lining cells without nuclear atypia, mitotic figures, or necrosis. Cases of this type have been interpreted in the past as epithelioid and spindled hemangioendotheliomas or as inflammatory pseudotumors (see below), but they have not recurred or metastasized after splenectomy. SANT is now felt to be a reactive fibrous entrapment of altered red pulp, presumably following some form of splenic injury, rather than a true neoplasm. More recent reports have described an increase in IgG4-positive plasma cells in SANT and some studies suggest an association with Epstein-Barr virus (EBV) in this proliferation.39, 41, 42 However, the EBV-positive cases appear to be overlap proliferations with splenic inflammatory pseudotumor and SANT is typically EBV-negative.43
FIGURE 66.5. Littoral cell angioma. A: Multinodular hemorrhagic lesions of the spleen in littoral cell angioma. B: Microscopically, there are papillary vascular spaces with plump lining cells and histiocytes.
FIGURE 66.4. Lymphangiomatosis. Cut surface of a spleen. Multiple, variably sized cysts are present.
Angiosarcoma of the spleen occurs most commonly in adults and is usually associated with splenomegaly, abdominal pain, and cytopenias.24, 44, 45, 46 Splenic rupture is common in these patients. Because most angiosarcomas involving the spleen are high-grade sarcomas with dissemination, it is often difficult to determine whether the splenic tumor is primary or secondary. The tumor forms an infiltrating mass that may have areas of cystic hemorrhage. The histologic appearance may be varied; however, angiosarcomas characteristically show cytologic atypia, high mitotic activity, and necrosis. Many cases may be difficult to differentiate from other high-grade sarcomas, and immunohistochemical detection of vascular antigen expression, such as CD31, CD34, and von Willebrand factor, is necessary to diagnose such cases. High-grade angiosarcomas involving the spleen have a generally poor prognosis, with most patients dying of disease within 1 year of diagnosis; however, rare cares with long-term survival following splenectomy have been reported.46
Low-grade angiosarcomas, also known as epithelioid hemangioendotheliomas, are much less common than high-grade tumors.47, 48, 49 These are reported to occur in both children and adults, but some of the adult cases have features similar to those more recently described for SANT (see above). Patients usually present with anemia and may have hyper- or hyposplenism. These tumors are better circumscribed than high-grade angiosarcomas with more bland epithelioid cells, vascular spaces, and prominent fibrosis. They also usually lack necrosis. The cells may show intracellular lumina and will express vascular-associated antigens. These tumors may be incidental findings, are usually localized to the spleen, and do not tend to recur after splenectomy.
Only gold members can continue reading. Log In or Register to continue
 The Diagnostic and Therapeutic Approach to Hematologic Problems
The Diagnostic and Therapeutic Approach to Hematologic Problems



