, Joong Mo Ahn2 and Yusuhn Kang2
(1)
Department of Radiology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, South Korea
(2)
Department of Radiology, Seoul National University, Bundang Hospital, Seongnam, South Korea
9.1 Enchondromatosis: Ollier Disease and Maffucci Syndrome
Enchondromatosis refers to nonhereditary sporadic skeletal disorders that present with multiple enchondromas. Ollier disease and Maffuci syndrome fall into this category. Ollier disease is a nonhereditary disorder characterized by multiple enchondromas, usually affecting the short and long tubular bones of the extremities (Figs. 9.1 and 9.2). Maffuci syndrome refers to enchondromatosis associated with multiple soft tissue hemangiomas in the soft tissue or viscera (Figs. 9.3 and 9.4). The diagnosis of enchondromatosis is made based on clinical features and characteristic imaging findings. Patients with enchondromatosis are at higher risk of developing secondary chondrosarcoma, compared to those with a solitary enchondroma, and are in need of regular follow-up.



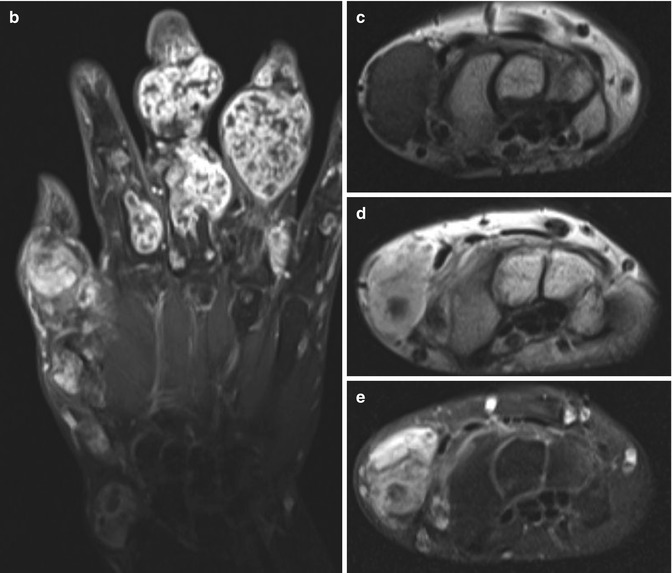


Fig. 9.1
Ollier disease. (a) Anteroposterior radiograph of the left hand shows multiple expansile osteolytic lesions in the phalanges of hand, with some showing chondroid mineralization. These lesions show typical features of chondroid matrix on magnetic resonance imaging. The lesions are isointense on T1-weighted image (b), hyperintense on T2-weighted fat-suppressed image (c), and show peripheral and septal enhancement (d)
Fig. 9.2
Ollier disease. Multiple enchondromas are noted at the right proximal femur (a), both proximal fibula (b), phalanges and metacarpal of hand (c), phalanges and metatarsal bones (d)
Fig. 9.3
Maffucci syndrome. (a) Anteroposterior radiograph of both hands show multiple enchondromas extensively involving the phalanges, metacarpal bones, and left distal radius and ulna. A magnified view of the left wrist shows a cluster of small round phleboliths (arrows), indicating the presence of soft tissue hemangiomatosis. (b) Coronal contrast-enhanced T1-weighted fat-suppressed image shows typical chondroid pattern of enhancement, peripheral and septal pattern with lobulated architecture. A soft tissue mass with intermediate signal intensity on T1-weighted image (c), bright hyperintensity on T2-weighted image (d), and strong enhancement on contrast-enhanced T1-weighted fat-suppressed image (e) is noted at the radial aspect of the left wrist. MR imaging findings are consistent with hemangioma
Fig. 9.4
Maffucci syndrome. Multiple enchondromas are present in the long bones and short tubular bones; multiple lesions in the tibia and fibula (a), phalanges, metatarsals and tarsal bones (b), radius and ulna (c) result in a skeletal deformity. (d) Characteristic phleboliths are noted along the radial side of the hand and along the thumb with prominent soft tissue shadow. The soft tissue lesion is consistent with hemangiomatosis on magnetic resonance imaging. (e) T1-weighted image shows soft tissue lesion with intermediate signal intensity intermixed with fat, and these lesions heterogeneously enhance on (f) contrast-enhanced T1-weighted fat-suppressed image (arrows on e, f)
9.2 Multiple Osteochondromas
(Synonyms: hereditary multiple exostoses, multiple cartilaginous exostoses, diaphyseal aclasis, osteochondromatosis).
Multiple osteochondromas (MO) is an autosomal dominant condition characterized by the development of two or more osteochondromas (Figs. 9.5 and 9.6). It is caused by a mutation in the tumor-suppressor genes EXT1 or EXT2. Osteochondromas grow and ossify during skeletal development and stop growing after skeletal maturity. MO may be associated with bony deformity, short stature, restricted joint motion, early osteoarthritis, and compression of peripheral nerves. Malignant transformation of osteochondroma to secondary chondrosarcoma has been reported to occur in 0.5–5 % of MO cases. Malignant transformation should be suspected when there is (a) newly developed pain, (b) interval growth of an osteochondroma in a skeletally mature patient, (c) irregularity of the lesion surface, (d) focal lucent regions within the lesion (d) erosion or destruction of adjacent bone, or (e) a soft tissue mass with irregular calcifications.
Fig. 9.5
Multiple osteochondromas. (a) Anteroposterior radiograph of the pelvis shows numerous sessile and pedunculated osteochondromas affecting the pelvic bone (arrows) and proximal femora. (b) Anteroposterior radiographs of both knee show numerous sessile and pedunculated osteochondromas affecting the distal femora, proximal tibia, and fibula. (c) A prominent pedunculated osteochondroma is noted at the proximal metaphysis of the femur. (d) Axial T1-weighted, (e) axial T2-weighted, and (f) axial contrast-enhanced T1-weighted fat-suppressed images are shown. The osteochondroma has medullary continuation with the mother bone, and has a cartilage cap (arrows in d–f) that is isointense on T1-weighted image, hyperintense on T2-weighted image
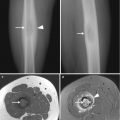
Fig. 9.6




Multiple osteochondromas. (a–c) Numerous sessile and pedunculated osteochondromas are noted at the proximal and distal metaphysis of both femora, proximal tibia and fibula, and left humerus
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
