(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
Sarcomas arising in one of the digits are rare. They are usually treated with amputation of the involved digit.
Sarcomas arising in the area of the metacarpals, if they are not too extensive, may be treated with resection of the metacarpal close to the tumor, the adjacent soft tissues, and the corresponding digit. The case being illustrated was that of a patient with a recurrent sarcoma located in the radial side of the second metacarpal, close to the dorsal surface. At the previous operation, a sarcoma close to the periosteum of the second metacarpal had been locally excised.
Through a small incision, histological confirmation of the local recurrence was first obtained (Fig. 3.1). A V-shaped incision from the base of the second metacarpal to the web space between the first and second and the second and third digits was performed (Fig. 3.2). Medial and lateral flaps of the skin were then raised sufficiently to provide a wider margin on the deeper tissues. The extensor tendon to the involved digit was divided proximally. Muscular attachments on the sides of the base of the second metacarpal were detached and a right-angle clamp was passed around the bone at this level to facilitate the passing of a Gigli saw, which was used to divide the metacarpal (Fig. 3.3). A V-shaped incision was also made on the palmar surface of the hand, replicating the incision of the dorsal surface (Fig. 3.4). On the dorsal aspect, in the web space between the first and second metacarpals, the origin of the first dorsal interosseous muscle was detached from the ulnar side of the first metacarpal (Fig. 3.5). The second dorsal interosseous was also divided between the second and third metacarpals.
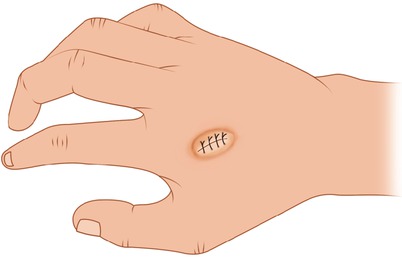
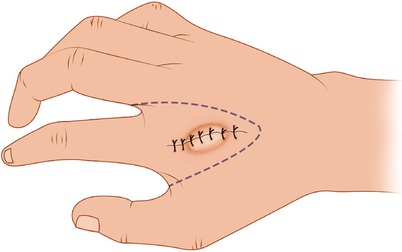
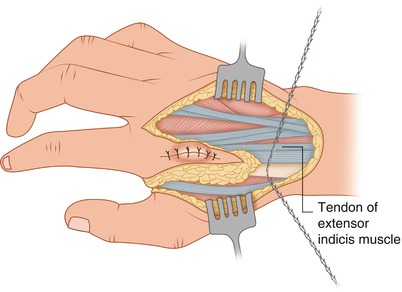
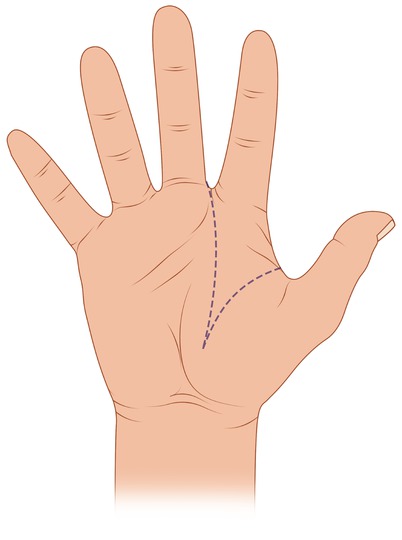
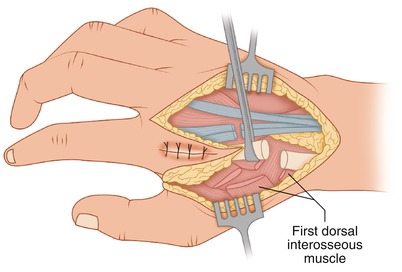
Fig. 3.1
Sarcoma at the second metacarpal
Fig. 3.2
A V-shaped incision allows removal of the second metacarpal with adjacent soft tissues
Fig. 3.3
The second metacarpal is divided at its base with a Gigli saw
Fig. 3.4
A V-shaped incision is made in the palmar aspect of the hand
Fig. 3.5
The first dorsal interosseous muscle is divided
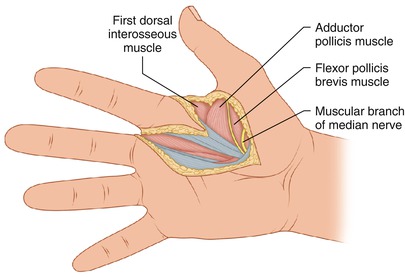
On the palmar surface of the hand, medial and lateral flaps of the skin and subcutaneous tissue were raised for about 2 cm on either side, to provide exposure. The palmar aponeurosis was incised, and the motor branch of the median nerve was identified and dissected laterally (Fig. 3.6). The sensory branches of the median nerve to the second digit were divided proximally. The flexor tendons also of the second finger were divided proximally.