(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
The investing fascia of the thigh forms a strong layer, the fascia lata, thicker on the lateral aspect where it forms the iliotibial tract, and thinner on the medial and posterior aspects. Two intermuscular septa extend between the linea aspera and the fascia lata. The medial septum, between the vastus medialis and the adductors, is thinner and becomes somewhat stronger in the lower part of the thigh. The lateral septum separates the anterior compartment of the thigh from the posterior compartment (the vastus lateralis from the short head of the biceps femoris).
The muscles of the thigh may be divided into three groups: the anterior, medial, and posterior compartments. The anterior compartment consists of the quadriceps muscle (extensor of the knee) and the sartorius, both supplied by the femoral nerve. The medial compartment, consisting of the adductor group of muscles supplied mainly by the obturator nerve, adducts the thigh. (The femoral nerve supplies the pectineus, and the sciatic nerve supplies the ischiocondylar portion of the adductor magnus.) The posterior compartment, consisting of the hamstring muscles, helps to flex the knee. In the anterior compartment, the quadriceps is composed of four muscles, which join in the lower part of the thigh to form the quadriceps tendon inserting at the base of the patella and then extending over the patella into the ligamentum patellae to the tuberosity of the tibia. Of these four muscles, the rectus femoris arises by a strong tendon split into the straight head, attached to the anterior inferior iliac spine, and the reflected head, attached to the acetabular labrum. The other three muscles, the vastus lateralis, intermedius, and medialis, arise from the shaft of the femur and the corresponding intermuscular septa. The vastus lateralis arises from the superior part of the intertrochanteric line and then the lateral edge of the linea aspera; the vastus intermedius arises from the shaft of the femur, starting from the intertrochanteric line to below the middle femur; and the vastus medialis arises from the inferior (medial) end of the intertrochanteric line and the medial edge of the linea aspera. The articularis genus, consisting of muscular bundles arising from the distal anterior surface of the femur, inserts to a proximal reflexion of the synovial membrane of the knee joint; it is also supplied by the femoral nerve. The nerve supply to rectus femoris, intermedius, and lateralis branches off in a lateral direction from the femoral nerve a few centimeters below the inguinal ligament, while the branch to vastus medialis continues separately along the muscle to enter and innervate its lower third (Fig. 47.1).
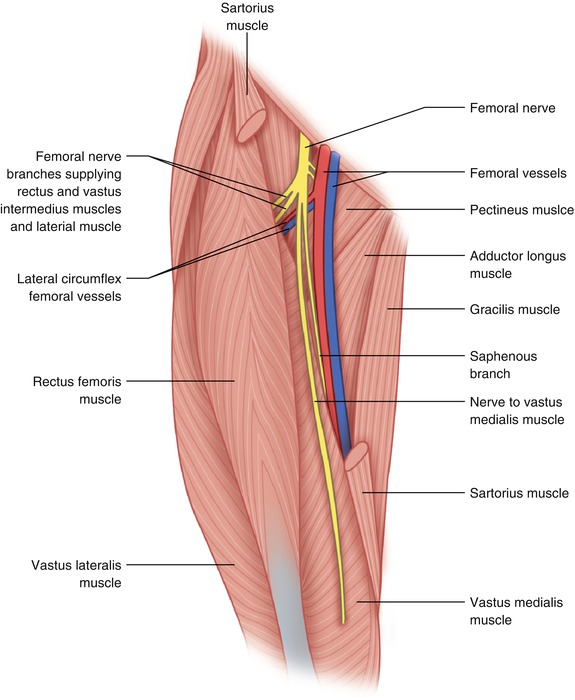
Fig. 47.1
Anatomy of the anterior thigh showing the separate innervation of vastus medialis
The blood supply of the quadriceps is mainly from the lateral femoral circumflex artery, a branch of the profunda femoris artery, and the corresponding vein (Fig. 47.2). The vastus lateralis and medialis are also supplied along their origin from the linea aspera by the perforators of the profunda artery. The lateral femoral circumflex vessels course transversely in the thigh from the profunda vessels, to behind the sartorius, and then behind the rectus femoris, where they divide into descending, transverse, and ascending branches. The descending branch supplies the rectus femoris, vastus intermedius, vastus lateralis, and vastus medialis. The vastus lateralis and vastus medialis are also supplied by the perforating branches of the profunda vessels. For a tumor located in the anterior compartment, it is usually possible to preserve at least one of the heads of the quadriceps (usually the vastus medialis or, less frequently, lateralis) with intact nerve supply (Figs. 47.3 and 47.4). For most cases in which the rectus femoris, vastus intermedius, and vastus lateralis are to be resected, one should be knowledgeable about the course of the nerve to the vastus medialis so that this muscle can be preserved with an intact nerve supply. This nerve is found in the femoral triangle deep to the sartorius and lateral to the femoral artery. Below the apex of the femoral triangle, the superficial femoral vessels and the saphenous nerve, the terminal sensory branch of the femoral, course in the so-called adductor canal. Also known as Hunter’s canal or the subsartorial canal, it has a triangular shape on cross-section and is bound by the vastus medialis laterally, the adductor longus and magnus posteriorly, and the sartorius anteriorly (the “roof” of the canal). More specifically, the roof of the canal consists of a dense membrane (vastoadductor), which extends between the adductors longus and, more distally, the magnus and vastus medialis at a deeper plane than the sartorius, which we may call the canal proper transmitting the femoral vessels through the adductor hiatus in the popliteal space. At the lower end of the canal proper, immediately above the hiatus tendineus, the saphenous nerve and the descending genicular artery exit the canal to assume more superficial positions. It is important to remember that the nerve to the vastus medialis is inside the canal with the expanded definition (the roof is the sartorius) but outside the canal with the restricted definition (the roof is the vastoadductor membrane).
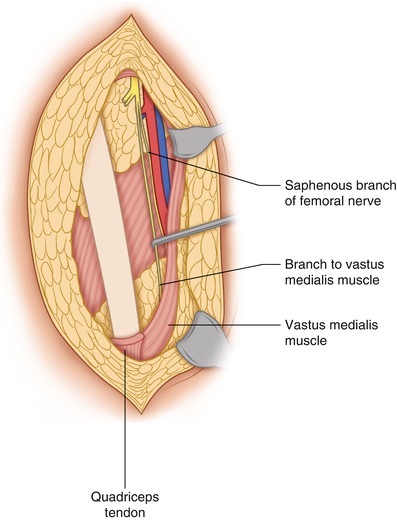
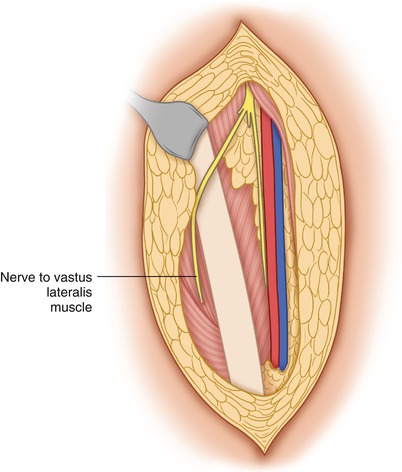
Fig. 47.2
Sarcoma of the anterior compartment of the right thigh is mobilized showing that its main blood supply is from the lateral femoral circumflex branches of the profunda vessels. It also shows the suitability of a rectus femoris myocutaneous flap in covering a defect in the ipsilateral groin and lower abdominal wall
Fig. 47.3
Following resection of the quadriceps minus the distal half of vastus medialis with intact innervation. The proximal half of the vastus medialis is removed with the specimen
Fig. 47.4
Following resection of the quadriceps minus the distal half of vastus lateralis with intact innervation
The vastus medialis is divided with the cautery or scalpel above the point of its innervation by its special nerve branch. After removal of the tumor en bloc with the rectus femoris, vastus intermedius, and lateralis, the stump of the quadriceps tendon is sutured to the adjacent edge of the vastus medialis with two or three figure-of-eight heavy, absorbable sutures so as to impart a straighter pull on the tendon with the contraction of the remaining medialis (Fig. 47.5). Preservation of the distal half of vastus medialis with its nerve supply maintains the function of knee extension without compromising the chance for cure (Figs. 47.6, 47.7, and 47.8).
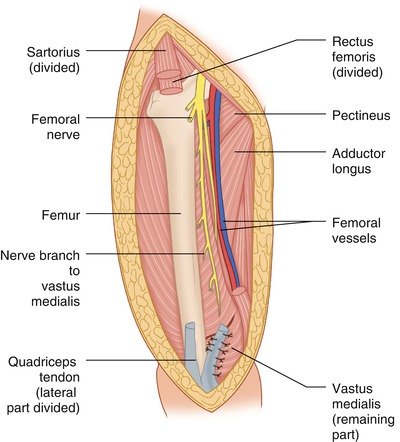
Fig. 47.5
Sutures may be placed between the stump of the divided quadriceps tendon and the adjacent vastus medialis to impart a straighter pull on the tendon, but this may not be necessary as some of our patients without this technical step were capable of performing straight-leg raising after some physical therapy
Fig. 47.6
CAT Scan image of soft tissue sarcoma of the left anterior thigh
Fig. 47.7




Operative field after resection of the sarcoma in Fig. 47.6. The nerve to vastus medialis encircled with vessel loops enters the lower portion of this muscle
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
