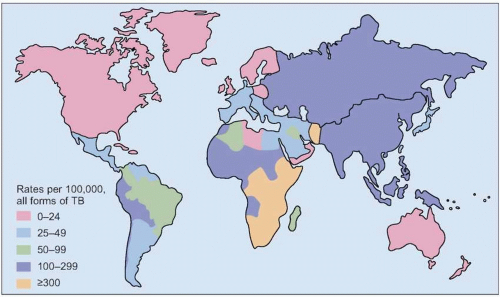
 Fig. 4.1 Estimated worldwide tuberculosis incidence rate 2004. (Adapted from WHO data.) |
Table 4.1 Persons at increased risk for developing active tuberculosis | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
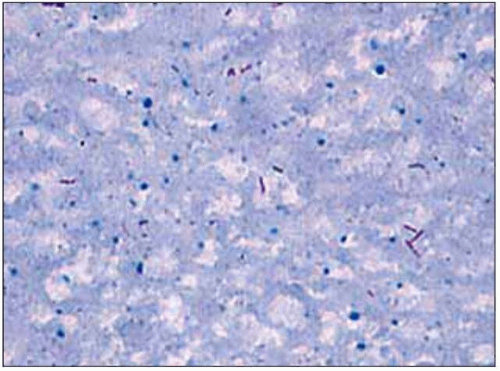 Fig. 4.2 Ziehl-Neelsen stain of sputum sample showing red acid-fast bacilli in a patient with cavitary pulmonary tuberculosis. |
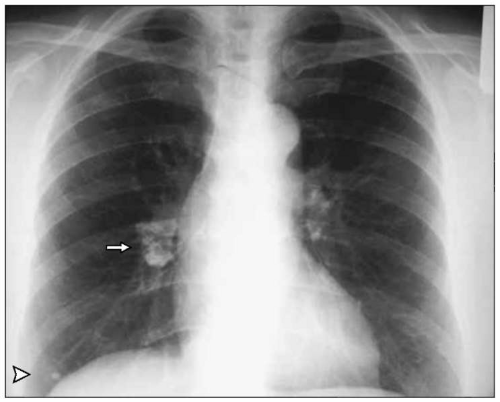 Fig. 4.3 A calcified Ghon focus is visible in the right lower lung field with associated hilar adenopathy. The combination of a Ghon focus (arrowhead) and a calcified draining lymph node is known as a primary (Ranke) complex (arrow). These radiographic findings are consistent with resolution of primary tuberculosis infection. (Courtesy of Dr Catherine Curley.) |
 Fig. 4.4 Chest radiograph showing apical scarring due to arrested tuberculosis (Simon’s foci) in an asymptomatic 55-year-old male. |
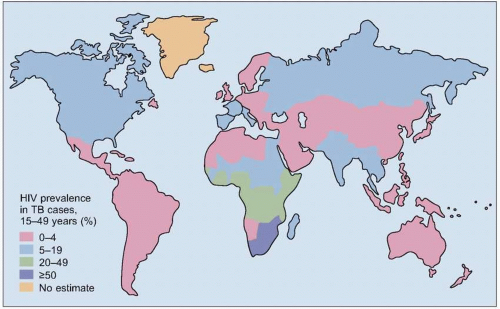 Fig. 4.5 Estimated prevalence rates of human immunodeficiency virus coinfection in patients with tuberculosis worldwide, 2004. (Adapted from WHO data.) |
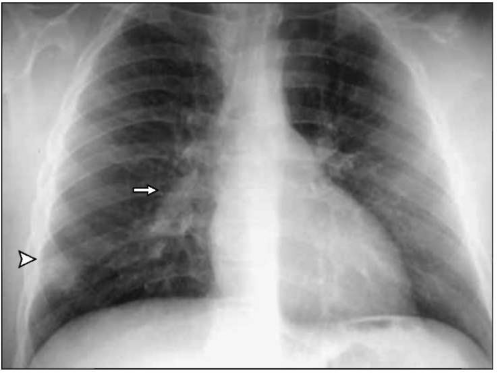 Fig. 4.6 Chest radiograph of a 4-year-old child presenting with low-grade fever and non-productive cough. There is a visible parenchymal infiltrate (Ghon focus) in the right lower lung field (arrowhead) and associated right hilar lymphadenopathy (arrow). The primary (Ranke) complex consists of the parenchymal lesion and the associated enlarged ipsilateral lymph nodes. (Courtesy of Dr Charles Daley.) |
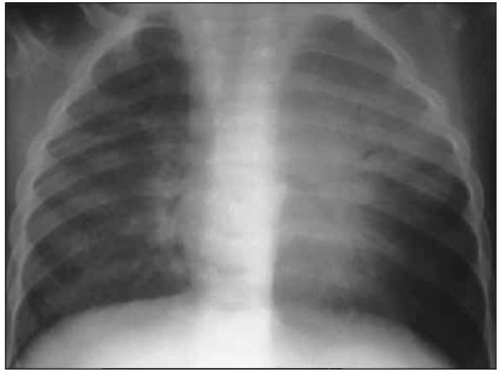 Fig. 4.7 Tuberculous pneumonia with left upper lobe infiltrate in a 4-year-old with fever and progressive primary tuberculosis. (Courtesy of Dr Charles Daley.) |
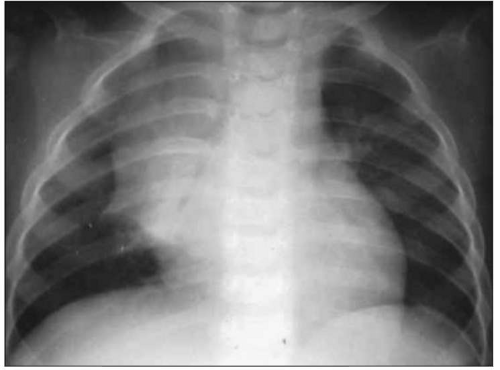 Fig. 4.8 Lobar collapse due to extrinsic bronchial compression from enlarged right hilar lymph nodes and endobronchial tuberculosis in a 5-year-old child with fever and chronic cough. (Courtesy of Dr Charles Daley.) |
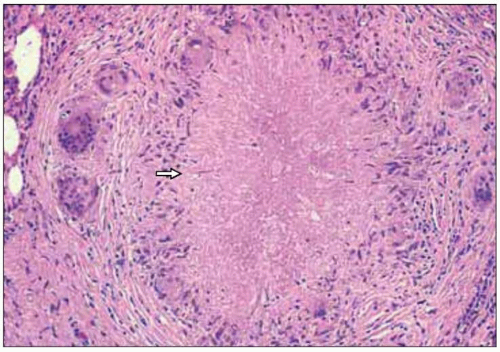 Fig. 4.9 Pulmonary granuloma (H&E, x100). Notice the area of central caseation (arrow) with a surrounding rim of lymphocytes, mononuclear cells, multinucleated giant cells, and fibrosis. |
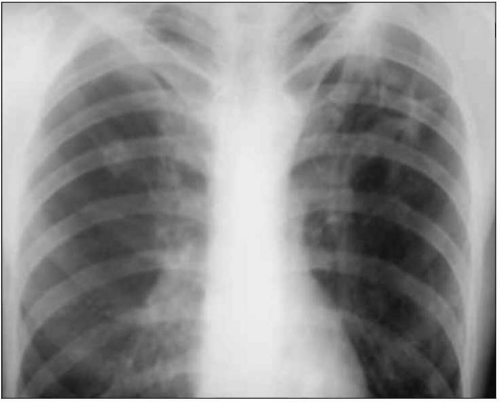 Fig. 4.10 Left upper lung cavity in patient with reactivation tuberculosis who presents with fever, productive cough, and weight loss. |
 Fig. 4.11 A chest radiograph from a 38-year-old male with 1 month of fever, weight loss, and productive cough. His chest radiograph shows a right upper lobe cavitary lesion with spreading throughout the right upper lobe and into the right lower lobe. This is an example of how caseous material and tubercle bacilli from an open cavitary lesion can spread endobronchially to other areas of the lung. |
 Fig. 4.12 Chest radiograph of a 48-year-old male presenting with wasting and a productive cough. It shows right upper lung involvement with a cavitary lesion and an air bronchogram. |
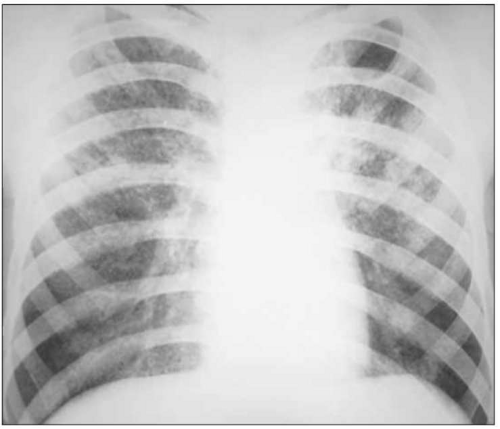 Fig. 4.13 Chest radiograph of a 34-year-old male with intermittent fever, weight loss, and no pulmonary symptoms. He was found to have miliary tuberculosis. Although the chest radiograph may be normal in a minority of cases, it usually shows classic miliary lesions, which are diffuse 1-2 mm rounded opacities (similar in size to millet seeds) scattered throughout all lung fields. Sometimes these lesions are best seen on a lateral view. Miliary tuberculosis is due to lymphatic and hematogenous seeding of tubercle bacilli to all areas of the lungs and other organs. |
 Fig. 4.14 Gross view of lungs from a fatal case of miliary tuberculosis. (Courtesy of Dr Rosana Eisenberg.) |
Table 4.2 Clinical and laboratory manifestations of active tuberculosis in early and late infection with human immunodeficiency virus | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
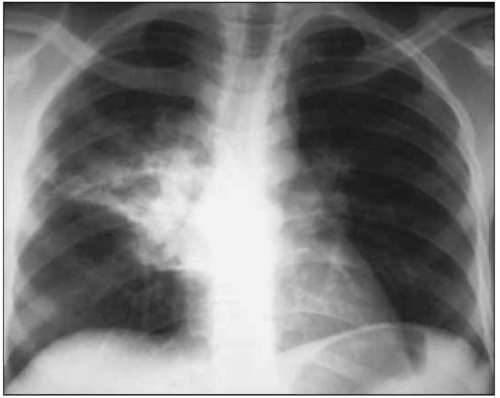 Fig. 4.15 Chest radiograph of a 28-year-old male with advanced acquired immunodeficiency syndrome (CD4+ count of 80/mm3) presenting with pleuritic right-sided chest pain and productive cough. A right mid-lung field infiltrate and associated hilar adenopathy are visible. |
 Fig. 4.16 Multilobar disease with associated hilar adenopathy in a patient with advanced human immunodeficiency virus/acquired immunodeficiency syndrome. |
 Fig. 4.17 Chest radiograph of a 35-year-old HIV-infected man with classic upper lobe fibrocavitary disease. Chest radiographic findings in patients with early HIV (CD4+ >200/mm3) are similar to findings in HIV-uninfected persons. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


