of urinary and sexual HRQOL after treatment for prostate cancer (Table 11A.1).
TABLE 11A.1 VALIDATED HEALTH RELATED QUALITY OF LIFE QUESTIONNAIRES USED FOR PATIENTS WITH PROSTATE CANCER | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 11A.2 PROSPECTIVE, MULTICENTER, NONRANDOMIZED COHORTS REPORTING HRQOL OUTCOMES FOR PATIENTS TREATED FOR PROSTATE CANCER | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 11A.3 RANDOMIZED TRIALS REPORTING COMPARATIVE EARLY-STAGE PROSTATE CANCER HRQOL OUTCOMES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
that used the PCSI instrument to measure HRQOL in a dose-escalation RCT did not detect HRQOL differences with dose escalation (90,91). HRQOL consequences of ultraconformal therapy are largely unknown, as side effect characterization of these modalities has been limited to physician-reported RTOG toxicity data (92,93).
leads to worse bowel/rectal HRQOL problems than does prostatectomy and does not reduce or palliate preexisting urinary obstructive symptoms as effectively as does prostatectomy (Table 11A.4) (33). Newer radiotherapy techniques such as IMRT, ultraconformal radiotherapy, and proton therapy are focused on delivering greater levels of radiation to the prostate while avoiding exposure of adjacent tissues and consequent side effects; however, HRQOL outcomes have not yet been definitively compared to standard radiotherapy or brachytherapy.
TABLE 11A.4 PREVALENCE OF MODERATE TO SEVERE PROBLEMS IN SPECIFIC HRQOL DOMAINS AFTER EARLY STAGE PROSTATE CANCER TREATMENT OR SURVEILLANCE | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1. What is the rationale for surveillance?
2. What proportion of low-risk patients initially accept active surveillance?
3. What is the rate of reclassification to higher risk disease and the rate of definitive therapy?
4. Are there reliable criteria for detecting progression?
5. What are the psychological effects of surveillance, that is, living with untreated cancer? Can we measure and manage this?
6. What is the course of disease in patients managed this way?
7. What is the outcome of delayed treatment?
8. What are the major pitfalls of surveillance and how can they be avoided?
9. What is the role of 5ARIs and focal therapy in these patients?
TABLE 11B.1 SUMMARY OF SIX ACTIVE SURVEILLANCE SERIES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
biopsy grade. The frequency of upgrading and upstaging is considerable in some of these series (27,28). Catalona et al. reported that using three different criteria for active surveillance eligibility, 3% to 4% had a Gleason score of 8 to 10, 16% to 19% had positive surgical margins, 15% to 18% had extracapsular tumor extension, 3% to 5% had seminal vesicle invasion, and 0.4% to 1% had lymph node metastasis. These data underscore the importance of refining the assessment of extent of disease at baseline. However, the extremely favorable outcome of large cohorts of patients managed with active surveillance suggests that the downside risk of an initial approach of expectant management is low. Patients with more aggressive disease are, in most cases, identified in a timely fashion by repeat biopsy or PSA kinetics.
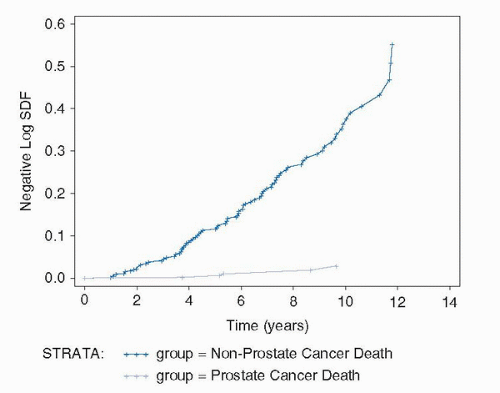 FIGURE 11B.1. Cumulative hazard ratio for nonprostate cancer to prostate cancer mortality. |
watchful waiting in Sweden. It found absolutely no significant psychological difference between the two groups after 5 years. Worry, anxiety, and depression all were equal between the two arms (34). The absence of any adverse psychological effect compared to patients treated radically has been reported by others (35). While surveillance may be stressful for some men, the reality is that most patients with prostate cancer, whether treated or not, are concerned about the risk of progression. Patients who have been treated curatively with surgery or radiation often remain focused on their PSA for many years, reflecting significant anxiety about recurrence. Patients who are educated to appreciate the very indolent natural history of most good-risk prostate cancers may avoid much of this anxiety. However, the long-term psychological effects of surveillance have not been studied in depth, and further studies in this area are a priority.
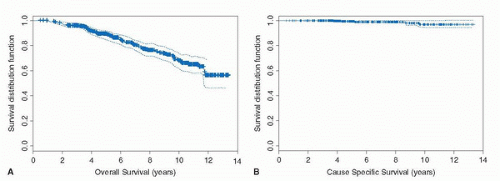 FIGURE 11B.2. (A) Overall survival in Toronto cohort. (B) Cause-specific survival in Toronto cohort. |
mortality of 3% at 15 years postrecurrence (19% × 13%). These patients were not offered salvage radiation therapy. In this case, the prostatectomy patients have been managed with early salvage radiation therapy, and the expectation is that half or more will have a complete response. Thus, the PSA failure rate in the treated patients, although high, is consistent with a prostate cancer mortality of about 2% in the 15-year time frame. Longer follow-up will be required to determine the true impact of the PSA failure rate in this cohort.
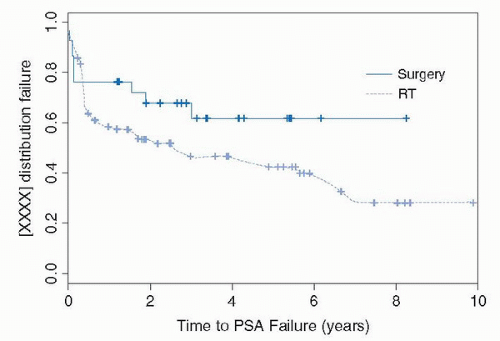 FIGURE 11B.3. PSA failure in 117 patients treated with surgery or radiation after a period of surveillance. |
Patient selection: Young age is not a contraindication. Rather, the longer the patient’s life expectancy, the more stringent the criteria should be. Men under 60, for example, are better candidates if they fulfill the Epstein criteria for insignificant prostate cancer (no more than one third of all cores positive, no more than half of any one core involved, and a PSA density <0.15). Men over 70, particularly with comorbidity, may have a PSA >10 or minor elements of Gleason 4 pattern and still be appropriate candidates. Patient choice is a key component of the decision making. Men under 70 with substantial Gleason 4 pattern (some would argue, any Gleason 4 pattern) (40) are not good candidates for surveillance.
A clear unmet need is more accurate prediction of an individual patient’s likely risk of disease progression at baseline. Advances in this field have already occurred in MR imaging of prostate cancer, and this will have an increasing role. Major progress is also being made in the molecular characterization of higher risk disease based on multiplex analysis of biopsy specimens and/or somatic single nucleotide polymorphism (SNPs) (41). All hold the promise of more accurate characterization of disease aggressivity in the near future. This remains an active area of research.
Education: The patient who is told he has prostate cancer often interprets this as meaning he has an aggressive lethal disease. This point is often reinforced by wellmeaning family and friends. Correcting this misconception is a major communication challenge. The key facts that should be provided to dispel this include the high prevalence of histologic prostate cancer (roughly equal to the patient’s age as a percentage), the high incidence to mortality ratio, the long natural history of favorable-risk disease (30-40 years from inception to lethal disease, when it occurs), and the side effects of therapy. Phrases like “part of the normal aging process” are convincing. The NNT in the ERSPC trial (2) and the nonprostate-to-prostate cancer mortality ratio of 19:1 in the Toronto cohort are useful facts for more sophisticated patients.
TABLE 11B.2 ACTIVE SURVEILLANCE: SUGGESTED CALENDAR FOR FOLLOW-UP
Follow-up schedule:
PSA, DRE q3mo × 2 yr, then q6mo assuming PSA is stable.
Confirmatory 10-12 core biopsy within first year, including anterolateral horn.
Repeat biopsy every 3-5 yr until age 80.
Intervention: For PSA doubling time <3 yr (in most cases, based on at least eight determinations) (about 20% of patients). Consider multiparametric MRI in uncertain cases, with targeted biopsy.
For grade progression to Gleason 7 with substantial proportion of 4 pattern (5% of patients).
These are guidelines and should be modified according to patient age and comorbidity.
(c) Follow-up: Table 11B.2 contains a suggested schedule for follow-up. It is the responsibility of the physician and the patient to maintain regular follow-up on surveillance, to monitor PSA kinetics, and have periodic repeat biopsies. A key task is to reassure the patient as to the indolent course of the disease.
suggesting that patients with high-risk prostate cancer may be the ones most likely to profit from extended PLND, especially those with micrometastatic disease. In the case of more extensive lymph node metastases, androgen deprivation therapy (ADT) may be of additional benefit (15). This chapter critically analyzes past and more contemporary literature pertaining to anatomic extent, indications, as well as the diagnostic and therapeutic benefit of PLND.
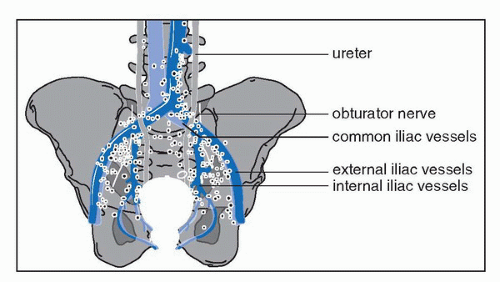 FIGURE 11C.1. Anatomic localization of primary lymphatic landing sites (sentinel nodes) by fusion of SPECT and CT or MRI in a 3D reconstruction model and confirmed by surgical removal. |
oxide nanoparticles as a contrast agent at MRI (LNMRI), however, may improve the detection of lymph node metastasis (9,11). Reported rates of sensitivity are 90% to 100% and of specificity 80% to 90% for LNMRI. However, the limitations of these studies are that most patients underwent a limited PLND, primarily removing the suspicious nodes. This falsely increases the sensitivity because other nodes potentially harboring small metastases were not removed and consequently not recognized. In addition the interpretation of LNMRI studies, for which a high interobserver variability has been reported, requires considerable experience and time. A recently proposed technique of MRI enhanced with ultrasmall superparamagnetic particles of iron oxide combined with diffusion-weighted MRI was found to be a fast and accurate method for detecting lymph node metastasis in prostate and bladder cancer, but needs to be confirmed in larger patient groups by other authors (12).
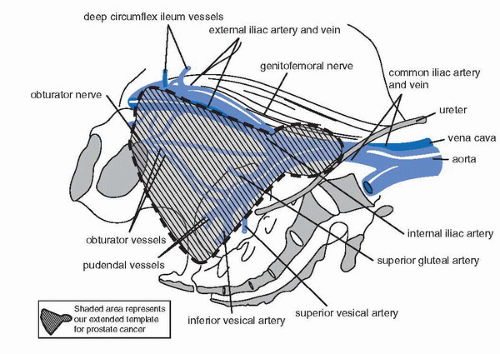 FIGURE 11C.2. Anatomical extent for our recommended extended PLND during radical prostatectomy where in addition to lymphatic tissue removed from the obturator fossa and the external iliac vein, the template also encompasses tissue on the medial and lateral aspects of the internal iliac vessels as well as along the common iliac vessels up to the ureteric crossing. |
follow-up of 5 years, there was no significant difference in BCR-free survival rates (86% and 88%). After reevaluation at a later time point, they again found no significant difference in the 10-year BCR-free survival rates (84% and 88%) (32). In a multicenter study comparing survival rates after no or limited PLND, again no difference in BCR-free survival rates was found (33). These studies, however, are limited by the fact that patients underwent a limited PLND only, the patients included were at low risk of dying of prostate cancer, and the number of patients included was too small for a statistically valid equivalence study. These data are not strong enough to rule out that a more extensive PLND may have been of benefit in some of these patients.
In patients with palpable and multiple nodal disease, however, it still remains to be seen if PLND, whether extended or not, represents more than just tumor mass reduction. Patients with gross nodal disease or with a PSA doubling time <12 months may profit from ADT.
TABLE 11C.1 SURVIVAL RATES IN PATIENT WITH PROSTATE CANCER AND LYMPH NODE METASTASIS WITHOUT IMMEDIATE HORMONAL THERAPY | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


