at lower risk of relapse may be offered surveillance with more confidence and those with risk factors may be more likely to be offered adjuvant radiotherapy or chemotherapy, but it must be stated that we do not know for sure the precise risk factors for relapse. With surveillance a significant proportion of patients may therefore avoid overtreatment.
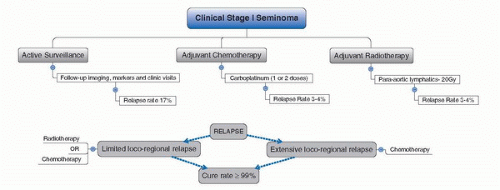 FIGURE 33A.1. Treatment algorithm after orchiectomy according to individual risk factors in patients with seminoma CSI. (Adapted from Krege S, Beyer J, Souchon R, et al. European consensus conference on diagnosis and treatment of germ cell cancer: a report of the second meeting of the European Germ Cell Cancer Consensus group (EGCCCG): part I. Eur Urol 2008;53:478.) |
TABLE 33A.1 SUMMARY OF SURVEILLANCE OUTCOMES FOR CSI SEMINOMA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 33A.2 PRINCESS MARGARET HOSPITAL STAGE I SEMINOMA SURVEILLANCE PROTOCOL | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
lymphatic drainage of the testis to include the ipsilateral pelvis and the paraaortic (PA) region. The decision to reduce fields from DL to PA was largely based on the Medical Research Council trial reported on by Fosså et al. in 1999. This trial randomized 478 men with stage I testicular seminoma to DL or PA radiotherapy of 30 Gy. The median follow-up was 4.5 years with nine relapses in each group, yet no pelvic recurrences in the DL versus four in the PA group. However, acute toxicity was less frequent and less pronounced in PA arm with sperm counts significantly higher in PA arm. They concluded that there was no difference in overall outcome with decreased morbidity in PA-only arm and thus recommended the PA field as standard. Overall, since the general adoption of the reduced PA field, this has not resulted in a reduction in survival rates, but interestingly, cases of recurrence at the edge of the traditional DL fields have been surfacing in the literature (35,36,37,38,39,40).
TABLE 33A.3 RATIONALE, ADVANTAGES AND DISADVANTAGES OF THE TREATMENT MODALITIES CURRENTLY AVAILABLE FOR CSI SEMINOMA | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
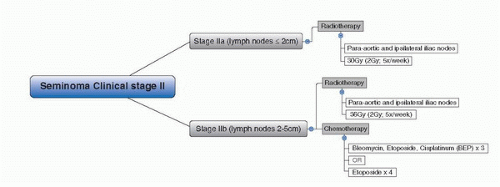 FIGURE 33A.2. Treatment algorithm after orchiectomy according to individual risk factors in patients with seminoma clinical stage II. (Adapted from Krege S, Beyer J, Souchon R, et al. European consensus conference on diagnosis and treatment of germ cell cancer: a report of the second meeting of the European Germ Cell Cancer Consensus Group (EGCCCG): part II. Eur Urol 2008;53:497.) |
normally low-burden retroperitoneal nodal disease, usually clinical stage IIA (nodes ≤ 2 cm) or stage IIB (nodes 2-5 cm). In stage IIA radiotherapy (infradiaphragmatic 35-40 Gy to include PA and ipsilateral iliac nodes) remains the preferred treatment option over chemotherapy. In stage IIB chemotherapy with three cycles of standard-dose BEP, or four cycles of EP, represents a treatment alternative to radiotherapy, particularly in patients with larger multinodal retroperitoneal disease (a small subset of the seminoma relapse patients) but may be associated with a higher risk of acute toxicity as compared to radiotherapy (19,66). However, one must also consider that recurrences do occur in the chemotherapy and radiotherapy arms meaning no guarantee of no relapse may be given if such treatment options are chosen.
diagnosis. In a prospective trial of centrally reviewed FDG-PET studies in 111 contemporary patients with CS I NSGCT on surveillance, relapse was observed in 33 of 87 patients who were PET negative with an estimated relapse-free rate of 63% (1). The investigators concluded that the FDG-PET is not sufficiently sensitive to accurately stage CS I NSGCT. De Wit et al. (2) also reported that FDG-PET yielded only slightly better results than computed tomography (CT) as a primary staging tool for low-stage NSGCT. Thus, there is currently no role for FDG-PET in the routine evaluation of NSGCT at the time of diagnosis. Abdominal-pelvic CT imaging remains the standard for staging NSGCT.
are frequently the earliest sign of relapse and these tests are low risk, relatively inexpensive, and widely available. Measurement of STM is typically performed every 1 to 2 months during year 1, every 2 to 3 months in year 2, every 3 to 6 months in years 3 to 5, and annually thereafter. The schedule of imaging tests is much more variable and surveillance schedules using less frequent cross-sectional imaging have reported similar outcomes compared to centers using more frequent imaging. The issue of greatest concern has been the hypothetical risk of the radiation from CT scans inducing secondary malignant neoplasms (31). A modeling study at Stanford estimated that very aggressive surveillance schedules such as the one recommended by the National Comprehensive Cancer Center Network would result in a 1.9% and 1.2% lifetime cancer risk for an 18- and 40-year-old, respectively (32,33). These numbers are significant relative to the <1% risk of dying of CS I NSGCT and this concern has led some centers to reduce the frequency and duration of CT imaging and/or to switch from CT to magnetic resonance imaging (14,17). Another approach has been the use of low-radiation-dose CT scans (30,34). Investigators at Princess Margaret Hospital have reported that radiation dose could be cut by 55% while maintaining adequate image quality in 99% of patients (34). A second concern is the cost of imaging studies. Given the very small number of relapses after 2 years of follow-up, demonstrating the cost-effectiveness or even any medical benefit from prolonged imaging schedules is difficult. The point at which additional imaging does more harm than good remains undefined. Long-term surveillance CT imaging entails exposing the whole population of patients to the radiation and costs of imaging in the hope of benefiting the few percent who will have late relapses with normal STM.
TABLE 33B.1 SURVEILLANCE OF CS I NSGCT OF THE TESTIS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


