Transformed lymphoma is a complex syndrome that encompasses an array of different underlying low-grade lymphoproliferative conditions transforming into more aggressive disease as manifest by morphologic, clinical, and genetic features. Over the last decade, advances in chemoimmunotherapy have led to new options. Knowledge surrounding the genetic changes driving the process of transformation is leading to novel targeted therapies. This article focuses on the transformation of chronic lymphocytic leukemia and follicular lymphoma into diffuse large B-cell lymphoma.
Key points
- •
Transformation is a common occurrence among patients with indolent lymphoma and often carries a poor prognosis.
- •
Traditionally transformed lymphoma has been considered difficult to treat and associated with poor prognosis.
- •
Increasing knowledge of the genetic drivers of this event is leading to new therapeutic approaches.
Introduction
Transformed lymphoma is a complex syndrome that encompasses an array of different underlying low-grade lymphoproliferative conditions transforming into more aggressive disease as manifest by morphologic, clinical, and genetic features. Traditionally, transformed lymphoma has been considered difficult to treat and associated with poor prognosis. However, over the last decade, advances in chemoimmunotherapy have led to new options for affected patients and better outcomes. In more recent years, utilization of knowledge surrounding the genetic changes driving the process of transformation is leading to the development and application of novel targeted therapies. Such therapies are typically not associated with the same toxicities that have accompanied high-dose chemotherapy and stem cell transplantation (SCT) and, therefore, are often suitable for use in patients who have multiple comorbidities or are of advanced age. However, there is an ongoing unmet need for novel therapies among some patients with transformed lymphoma because many of the genetic aberrations seen converge on currently untargetable pathways, such as CDKN2A, MYC, or loss of TP53.
This article focuses on 2 of the more common scenarios: (1) the transformation of chronic lymphocytic leukemia (CLL) to diffuse large B-cell lymphoma (DLBCL), a process known as a Richter transformation (RT); and (2) the transformation of follicular lymphoma (FL) into DLBCL. For completeness, a variety of other less common situations in which transformation is recognized are described.
Introduction
Transformed lymphoma is a complex syndrome that encompasses an array of different underlying low-grade lymphoproliferative conditions transforming into more aggressive disease as manifest by morphologic, clinical, and genetic features. Traditionally, transformed lymphoma has been considered difficult to treat and associated with poor prognosis. However, over the last decade, advances in chemoimmunotherapy have led to new options for affected patients and better outcomes. In more recent years, utilization of knowledge surrounding the genetic changes driving the process of transformation is leading to the development and application of novel targeted therapies. Such therapies are typically not associated with the same toxicities that have accompanied high-dose chemotherapy and stem cell transplantation (SCT) and, therefore, are often suitable for use in patients who have multiple comorbidities or are of advanced age. However, there is an ongoing unmet need for novel therapies among some patients with transformed lymphoma because many of the genetic aberrations seen converge on currently untargetable pathways, such as CDKN2A, MYC, or loss of TP53.
This article focuses on 2 of the more common scenarios: (1) the transformation of chronic lymphocytic leukemia (CLL) to diffuse large B-cell lymphoma (DLBCL), a process known as a Richter transformation (RT); and (2) the transformation of follicular lymphoma (FL) into DLBCL. For completeness, a variety of other less common situations in which transformation is recognized are described.
Richter transformation
Predisposing Factors for Richter Transformation Among Chronic Lymphocytic Leukemia Patients: Clinical and Genetic
RT is defined as the transformation of CLL into an aggressive lymphoma, most commonly DLBCL. Cumulatively, over the natural history of patients’ course with CLL, RT occurs in between 5% to 20% of cases and is a well-recognized and feared complication due to its poor prognosis (when compared with de novo DLBCL or CLL alone). Importantly, this inferior prognosis seems only to apply to cases in which the DLBCL is clonally related to the underlying CLL (eg, by demonstrating a shared immunoglobulin variable heavy chain [IGVH] usage). DLBCL arising in patients with CLL in whom there is not a clonal relationship to the preceding CLL (up to 20% of cases) has been reported to have a more favorable outcome.
Rossi and colleagues followed 185 CLL subjects from the time of CLL diagnosis to more accurately define the incidence and risk factors for RT. In this cohort, 17 subjects were diagnosed with an RT with an actuarial incidence of 13.6% and 16.2% at 5 and 10 years, respectively, with no further cases diagnosed beyond 82.5 months. Among those subjects who developed RT, the median time to RT was 23 months from the diagnosis of CLL. In univariate analysis, lymph node bulk (≥3 cm), higher numbers of nodal groups involved (≥3), elevated serum levels of lactate dehydrogenase (LDH), diffuse bone marrow involvement, and more advanced Binet stage were all associated with a greater risk for transformation. However, on multivariate analysis, only lymph node bulk remained independently associated with risk of transformation. Other traditional clinical prognostic markers were not found to be associated with greater risk for transformation, including advanced age, poor performance status, Rai stage, cytopenias, lymphocyte count, splenomegaly, percentage bone marrow infiltration, and β 2 -microglobulin (β 2 M). Importantly for therapeutic purposes, fludarabine exposure was not significantly associated with an increased risk of transformation.
Numerous pathologic and genetic features have been associated with an increased risk of RT. The most potent of these seem to be (1) an unmutated IGVH, (2) the presence of NOTCH1 mutations, and (3) stereotypy of the B-cell receptor. IGVH 4–39 usage has also been associated with an increased risk of RT (particularly when occurring in cases with a NOTCH1 mutation). Other features that have been associated with an increased risk of RT include CD38 expression, ZAP-70 expression, high-risk fluorescence in situ hybridization (FISH) lesions (eg, deletion 17p, deletion 11q), and trisomy 12 ( Box 1 ).
Clinical
Lymph node bulk ≥3 cm
Univariate and multivariate
≥3 nodal groups
Univariate
Elevated LDH
Univariate
Diffuse marrow involvement
Univariate
Advanced Binet stage
Univariate
Immunophenotypic
High CD38 expression
High ZAP-70 expression
Genetic
Unmutated IGVH
NOTCH1
Stereotypy of B-cell receptor
IGVH 4–39 usage especially with NOTCH1 mutation
Deletion 17p
Deletion 11q
Trisomy 12
Presentation of Richter Transformation: Clinical and Genetic Landscape at Transformation
Recognition of RT can be challenging. In advanced cases, patients can present with a fulminant illness characterized by florid B symptoms (including fatigue, reduced energy, reduction in performance status, significant unintentional weight loss, fevers, night sweats, malaise) and rapidly increasing lymphadenopathy and splenomegaly. In other cases, however, the presentation can be more subtle and even not recognized by less vigilant clinicians without a proactive approach to looking for the condition on lymph node biopsy or PET.
Typical features of patients with newly diagnosed RT were reported in 1 study of 39 subjects with RT. In this study, the clinical features at diagnosis included B symptoms (59%), progressive lymphadenopathy (64%), extranodal disease (41%), and elevated LDH (82%), These features have been consistently noted in case series of RT since the late 1970s; other features reported include hepatosplenomegaly.
Genomic analysis of paired samples suggests that, in most cases, the aggressive clone in RT directly evolves from the original CLL clone through acquisition of additional genetic lesions (linear evolution). These genetic lesions converge on dysregulation of cell cycle control and activation of MYC. There are 2 predominant pathways through which this cell cycle/MYC dysregulation may occur:
- 1.
Aberrancies of TP53, CDKN2A/B, and MYC. Acquired abnormalities in TP53 (either mutation or copy number loss) are a hallmark of CLL with poor prognosis. Although TP53 abnormalities can clearly exist within the CLL compartment without overt RT, TP53 abnormalities are acquired around the time of transformation in a proportion of patients. In contrast, abnormalities in CDKN2A/B (typically copy number changes) are almost never observed in the CLL compartment and seem to be an RT-specific phenomenon. In addition, abnormalities in MYC (either translocations, copy number amplifications, or mutations) tend to coexist with TP53/CDKN2A/B abnormalities and, in most cases, seem to occur around the time of transformation.
- 2.
Trisomy 12/NOTCH1 mutations. The presence of trisomy 12 and mutations that truncate the PEST domain of NOTCH1 result in a fertile ground for the development of RT. Unlike MYC/CDKN2A/B aberrancies, trisomy 12 and NOTCH1 mutations precede the development of RT in most cases (often by many years). Notably, up-regulation of cell cycle–associated genes by gene expression profiling has been observed in trisomy 12 and NOTCH1-mutated CLL. In addition, NOTCH1 signaling has been observed to induce MYC expression in T-acute lymphoblastic leukemia.
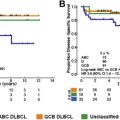
The resultant clonally related DLBCL in RT is genetically distinct from both de novo DLBCL and clonally-unrelated DLBCL that arises concurrently in patients with CLL. RT is almost always of nongerminal center type when classified by immunohistochemistry. Despite this, it does not display the typical mutational profile of an activated B-cell–subtype DLBCL. The significantly inferior prognosis when compared with de novo DLBCL and the genetic differences, justify its consideration as a distinct entity.
Natural History and Prognosis of Richter Transformation
The median survival reported in the literature after the diagnosis of RT varies from 8 months to 16.5 months ; however, the event of RT is universally considered to convey a far inferior prognosis than would be expected among the group of CLL patients as a whole. The variability in prognosis may in part relate to institutional and clinician-specific approaches to active surveillance for the condition, such as early lymph node biopsy potentially introducing lead-time basis into many estimates of survival.
A retrospective study of 148 patients with proven RT treated at the MD Anderson Cancer Center identified the following clinical and laboratory features as risk factors for adverse outcome in RT: poor performance status, elevated LDH, thrombocytopenia, bulky lymphadenopathy (≥5 cm), and more than 2 prior lines of therapy. The investigators found that the more of these adverse prognostic factors were present, the worse the survival. Using these prognostic factors the investigators developed a scoring system in which patients with zero to 1 risk factors had a median survival of 1.1 years, whereas those with 3 risk factors had a median survival of 0.33 years.
More systematic elucidation of the genetic features predicting for outcome in confirmed cases of RT is important, given the range of survival reported in the disease, to better target therapy to more precise prognostic information.
Therapeutic Options for Richter Transformation
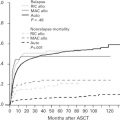
Tsimberidou and colleagues, retrospectively report on the outcomes of 148 RT patients managed at the MD Anderson Cancer Center of whom 130 received active disease-directed treatment. The therapies used varied widely but included nucleoside-analog–based purine (18%); alternating fractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone with high-dose methotrexate and cytarabine (hyper-CVAD) and variants (16%); cyclophosphamide, adriamycin, vincristine and prednisolone (CHOP)-like therapy (8%); and other therapies (19%), including cytarabine, ifosfamide, and etoposide. Notably, approximately 60% of these patients were managed in the pre-rituximab (R) era, potentially limiting the applicability of these findings in the current therapeutic environment. Among patients treated with chemotherapy alone, 11% achieved a complete remission (CR) and 66% had no response to therapy. The outcomes were only slightly better among the immunochemotherapy cohort, with 13% achieving CR and 63% having no response. Among this group of patients with RT, 20 received SCT. Patients receiving SCT were treated with a variety of regimens, including chemotherapy and chemoimmunotherapy, and most patients did not obtain a CR before transplant. For the patients who went into allograft while in CR or PR, the 3 year survival was approximately 75%, in contrast to 27% among the patients who achieved CR or PR with initial therapy but did not proceed to allograft and 21% among the patients who underwent transplant with relapsed or refractory RT. Indeed, receipt of an allogeneic stem cell transplant was independently associated with prolonged survival in RT. This suggests that the specific initial therapy is less important than the ability to achieve disease response and proceed to allograft as consolidation.
Notably, the chemotherapeutic regimens used in the MD Anderson cohort were relatively intensive and many patients presenting with RT are unfit for such regimens, and given that the median age at diagnosis of CLL is 72 years, most patients developing RT will unfortunately not be eligible for allogeneic SCT. The patients who did not receive allograft had a poor prognosis, highlighting the urgent clinical need for novel agents to manage this disease with less toxicity and greater efficacy.
One of the challenges in evaluating novel therapies in RT is that in many studies specifically exclude transformed lymphoma, including RT, meaning that there is limited evidence available. However, extrapolating from early phase data on Burton tyrosine kinase inhibitor (BTKi) ibrutinib, 7 out of 11 subjects whose CLL progressed on this agent developed RT. Because many of these events occurred early in the study, it has been hypothesized that they represent residual nonresponsive disease that was present at study entry. In contrast, the BCL2 inhibitor venetoclax has been tested in phase I studies among 7 subjects with RT with an overall response rate (ORR) of 43%.
Chronic Lymphocytic Leukemia Transformed to Prolymphocytic Leukemia
B prolymphocytic leukemia (B-PLL) is a monoclonal B cell neoplasm in which greater than 55% of the circulating malignant cells in the peripheral blood are prolymphocytes (large lymphocytes with prominent nucleolus). The disease can arise de novo or in the context of pre-existing CLL in which the prolymphocytes can be shown to be genetically transformed with clonal differentiation from the underlying CLL. Transformed B-PLL is immuno-phenotypically distinct from both de novo B-PLL and the underlying CLL. A possible genetic contributor to prolymphocytic transformation of CLL was the observation of high levels of activation-induced cytidine deaminase and aberrant somatic hypermutation in patient samples with transformed disease.
Although there is a spectrum of disease with prolymphocytes ranging from 55% to 100% of the circulating malignant cells, increasing circulating prolymphocyte percentage in CLL is often accompanied by worsening clinical symptoms requiring therapy. Similarly to CLL that undergoes RT to DLBCL, transformation to B-PLL represents a change in the clinical behavior of the CLL to a disease that is less chemotherapy responsive and carries an inferior prognosis.
Chronic Lymphocytic Leukemia Transformed to Hodgkin Lymphoma
Transformation of CLL to Hodgkin lymphoma is well described but much less common than the more typical RT to DLBCL, with only 86 cases described in the literature as of 2012. This phenomenon is predominantly seen in older men and usually occurs within 5 years of the original CLL diagnosis. Like RT to DLBCL, the occurrence of HL in patients with CLL portends a poor prognosis. However, it is not as profoundly adverse as DLBCL RT, with a mean survival of only 2.1 years, despite treatment in most cases with multiagent chemotherapy, such as adriamycin, bleomycin, vinblastine, and dacarbazine (AVBD). However other case series have shown inferior survival with 50% cumulative survival at 12 months reported. Survival is even worse among patients whose CLL has previously been treated with fludarabine-containing regimens (mean survival of only 0.7 years).
As with most cases of transformed lymphoma, Hodgkin lymphoma arising in the setting of CLL has been shown to be clonally related to the underlying CLL. Sequencing of IGVH in microdissected Reed Sternberg cells has demonstrated that the Hodgkin lymphoma is clonally identical to the underlying CLL in some cases. Although subject numbers remain limited, 1 study has found that most cases of CLL transformed to HL, and have evidence of Epstein Barr virus infection and unmutated IGVH.
Transformed follicular lymphoma
Incidence and Risk Factors for Transformation in Follicular Lymphoma
Transformation of FL (typically to DLBCL) is a clinicopathological diagnosis characterized by histologic change in the lymphoma from small centrocyte cells with a follicular growth pattern to that of a disordered large cell growth pattern. The definition implies that the DLBCL is clonally related to the FL. Accompanying transformation, the lymphoma typically develops the clinical behavior of an aggressive lymphoma-producing B symptoms, rapid enlargement of lymph nodes, and evidence of rapid cell turnover (eg, elevated LDH).
The reported incidence of transformed FL (t-FL) in the literature varies widely but is thought to be approximately 2% to 3% per year, implying that the cumulative incidence increases with duration of FL. Some groups, however, report a plateau in the incidence of transformation beyond 15 to 20 years. Disappointingly, this incidence seems unaltered in the post-R era, suggesting that the risk of transformation is an inherent characteristic of the natural history of FL and not altered by more potent therapeutic intervention, at least those currently applied. Furthermore, the outcomes of early therapeutic intervention studies on the incidence of transformation have been contradictory. Some studies suggest benefit in terms of the risk transformation among patients whose FL was treated early and aggressively to maximize disease control. Other studies, however, have demonstrated that the chemotherapy regimen used (eg, chlorambucil versus multiagent CHOP) and the degree of response to therapy (eg, partial remission [PR] versus CR) have no effect on the risk of transformation.
A variety of risk factors have been associated with the development of transformed disease in FL on either univariate or multivariate analysis. Frequently, reported risk factors include elevated LDH, advanced age, high Follicular Lymphoma International Prognostic Index (FLIPI) or International Prognostic Index (IPI), grade 3 FL histology, cytopenias, extranodal disease, more than 3 nodal areas involved, and elevated β 2 M ( Box 2 ).
Clinical
Elevated LDH
Advanced age
High FLIPI score
Grade 3 histology
Cytopenias
Extranodal disease
≥3 nodal areas
Elevated β 2 M
Genetic
TP53 mutation
BCL6 translocations
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


