The Postsurgical Breast
A wide variety of mammographic findings are seen after surgical procedures on the breast. Surgical procedures—including core needle biopsy, excisional breast biopsy, wide excision or segmental mastectomy, subcutaneous or modified radical mastectomy with reconstruction, reduction mammoplasty, and lumpectomy with radiation therapy—produce a spectrum of classical and unusual findings. Critical to an accurate analysis of a mammogram and to determination that findings are of postsurgical origin is knowledge of the history and clinical examination of the patient.
It is of help to place a wire or BB marker on the skin to avoid repeating films because of uncertainty about positions of scars. If this is not done, then it is absolutely necessary that the technologist be responsible for clearly marking the location and orientation of any scars on a drawing of the breast. The surgical site is sometimes demarcated with surgical clips, particularly in cases of lumpectomy performed for carcinoma. Additionally, it is equally important to document the location and size of any palpable masses and particularly their relationship to the surgical scar.
In interpreting a mammogram of a postsurgical breast, it is important for the radiologist to compare present studies with previous studies. Temporal changes are reflective of the normal evolution of postsurgical findings. Also, knowledge of the appearance of the original lesion in patients who have undergone lumpectomy and correlation with the specimen film is helpful to identify residual disease.
Postbiopsy Changes
Immediately after a needle biopsy of a breast lesion, there may be a small amount of air at the biopsy site, especially when a vacuum-assisted biopsy is performed. Occasionally, there also may be irregular increased density at the site from edema and hematoma formation. Unless there is significant bleeding during the biopsy, the changes are subtle. If there is a puncture of a vessel during a needle biopsy, a hematoma may form. If the hematoma dissects through the tissue, an amorphous ill-defined density is seen on mammography. If a hematoma is more localized, then the appearance is that of a relatively circumscribed mass (Fig. 12.1). These findings are typically observed immediately after the biopsy on the postprocedure mammogram. In most cases, however, there is no long-term mammographic finding after a needle biopsy.
The mammographic findings associated with excisional biopsy are localized to the area of the biopsy site. It is, therefore, important to correlate the position of the scar to the mammographic findings and to be aware of the temporal changes that are expected postsurgically. In a study of 1,049 breast biopsies, Sickles and Herzog (1) found mammographic abnormalities attributed to postsurgical changes in 474 (45%). Normal postsurgical changes include localized skin thickening or retraction, an asymmetric glandular defect, architectural distortion, contour deformity of the breast, hematoma or seroma, fat necrosis formation, parenchymal scarring (Figs. 12.2,12.3,12.4,12.5,12.6), calcifications of fibrosis (Figs. 12.7 and 12.8), fat necrosis and sutures, and opaque foreign bodies (1,2) (Figs. 12.9,12.10,12.11).
Skin thickening is localized to the biopsy site unless there is superimposed infection, in which case a more generalized thickening is present. A contour deformity may be associated with the skin thickening. Skin thickening is maximum on mammography during the first 6 months after biopsy and gradually diminishes. In a majority of patients who have undergone a lumpectomy or excisional biopsy for benign disease, the focal skin thickening is nearly inapparent on mammography after several years.
A hematoma may be seen at the biopsy site on a mammogram performed soon after biopsy. Postoperative hematoma or seromas are seen more commonly if a drain has not been placed and may actually be related to an improved cosmetic result with a lesser degree of contour
deformity (3). On mammography, fluid collections are usually relatively circumscribed medium- to high-density masses and may range from 2 to 10 cm in diameter. In a series of postlumpectomy patients who were referred for radiotherapy, Mendelson (3) found postoperative fluid collections in 47%. On ultrasound, hematomas or seromas are relatively smooth and anechoic but may contain some internal echoes or debris, depending on the degree of organization (4). Because fluid collections may contain debris even if they are not infected, the clinical findings are of more help to suggest the presence of superimposed infection.
deformity (3). On mammography, fluid collections are usually relatively circumscribed medium- to high-density masses and may range from 2 to 10 cm in diameter. In a series of postlumpectomy patients who were referred for radiotherapy, Mendelson (3) found postoperative fluid collections in 47%. On ultrasound, hematomas or seromas are relatively smooth and anechoic but may contain some internal echoes or debris, depending on the degree of organization (4). Because fluid collections may contain debris even if they are not infected, the clinical findings are of more help to suggest the presence of superimposed infection.
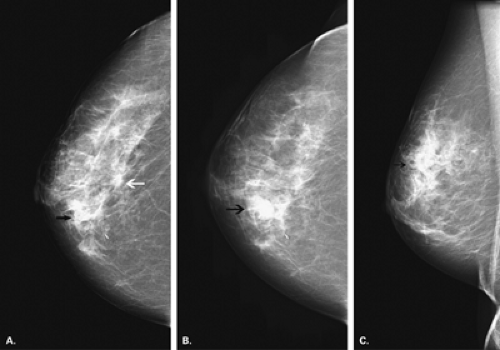 Figure 12.1 HISTORY: A 45-year-old woman for biopsy of multiple left breast lesions. MAMMOGRAPHY: Left CC view (A) immediately after needle biopsy and left CC (B) and ML (C) views 2 hours later. A spiculated mass is present centrally (white arrow), and an indistinct mass is located medially (arrow), both of which were biopsied. There are also faint, pleomorphic microcalcifications laterally that were biopsied. Following vacuum-assisted core needle biopsies, the medial area was associated with the interval development of a lobulated circumscribed mass, consistent with a hematoma. IMPRESSION: Hematoma following core needle biopsy of suspicious left breast lesion, multiple left breast lesions suspicious for carcinoma. HISTOPATHOLOGY: Invasive ductal carcinoma, multicentric. NOTE: The medial round mass represented a small hematoma secondary to core biopsy. |
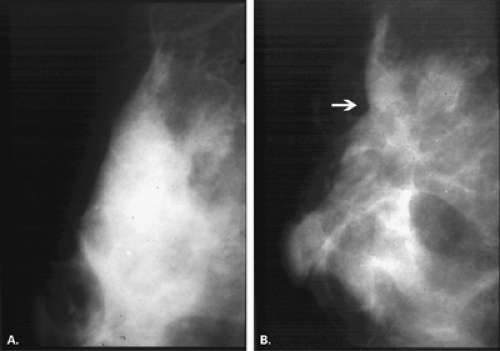 Figure 12.2 HISTORY: Routine mammography following surgical excision for left breast microcalcifications that were benign. MAMMOGRAPHY: Left MLO (A) and left MLO (B) 1 year later, following surgical excision. There is dense parenchyma with some fine punctuate and amorphous microcalcifications in a regional distribution (A). These were removed by surgical excision following needle localization. IMPRESSION: Contour defect following surgical excision or lumpectomy. |
Areas of architectural disturbance are a common finding after surgery and include asymmetric decrease in glandular tissue from resection that does not change over time (1), architectural distortion, and focal increased density or parenchymal scar and fat necrosis. As a hematoma resolves, it is usual to see some residual, irregular increased density and/or distortion. Architectural distortion was the second most common postsurgical finding after skin thickening by Sickles and Herzog (1) in the evaluation of 474 postoperative breasts.
The changes of increased density and architectural distortion are maximum at 0 to 6 months after surgery and gradually diminish over time (1). The presence of entrapped fat within the distortion is also suggestive of scar. Scars also tend to have a different shape on two views, appearing as a spiculated area of architectural distortion on one view and as much less distorted on the orthogonal view. Often the extension of the distortion to the skin scar is also noted.
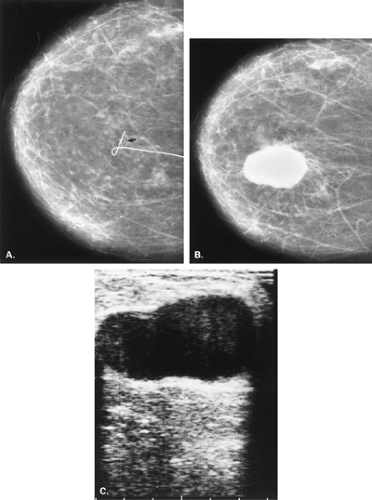 Figure 12.3 HISTORY: A 48-year-old gravida 2, para 2 woman 6 months after left breast biopsy, presenting with no new palpable findings. MAMMOGRAPHY: Left CC view from a needle localization (A) and left CC view (B) and ultrasound (C) 6 months after biopsy. On the initial film (A), a needle localization wire is marking a cluster of microcalcifications (arrow) for biopsy. The histopathology was benign. On the subsequent study (B), there is a large, high-density, partially circumscribed mass at the biopsy site. On ultrasound (C), the mass is complex, appearing circumscribed with some acoustic enhancement. The features are typical of a postoperative hematoma or seroma, and a fluid collection of this size may not be palpable. The patient was followed without aspiration of the seroma. IMPRESSION: Large postoperative hematoma or seroma. |
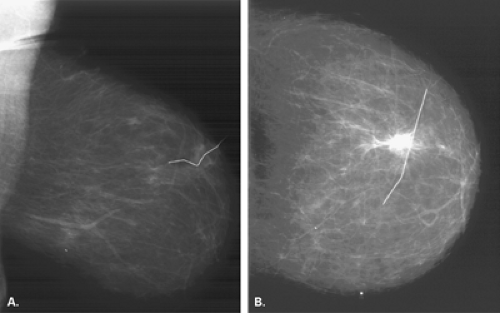 Figure 12.4 HISTORY: A 51-year-old woman status post–benign right breast biopsy. MAMMOGRAPHY: Right MLO (A) and CC (B) views show an essentially fatty-replaced breast. The postsurgical site is indicated by a wire marker. This appears dense and spiculated on the CC view but is more amorphous and vertically oriented on the MLO view. The differing appearance on the two projections is typical of a scar. IMPRESSION: Postsurgical scar. |
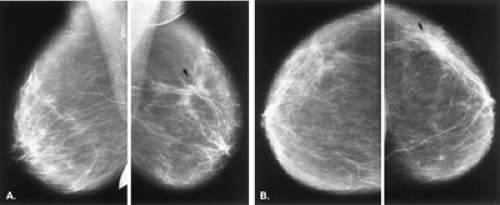 Figure 12.5 HISTORY: A 72-year-old gravida 2, para 2 woman for follow-up 1 year after a right breast biopsy that showed fibrocystic change. MAMMOGRAPHY: Bilateral MLO (A) and CC (B) views. There is an irregular density in the right upper-outer quadrant (arrows). On the MLO view (A), the lesion appears somewhat less dense and spiculated than on the CC view (B). The difference in shape of such a density suggests more likely a benign rather than a malignant etiology. This density was confirmed to be in the location of the scar from the previous biopsy. IMPRESSION: Irregular density consistent with fat necrosis and scar after excisional biopsy. |
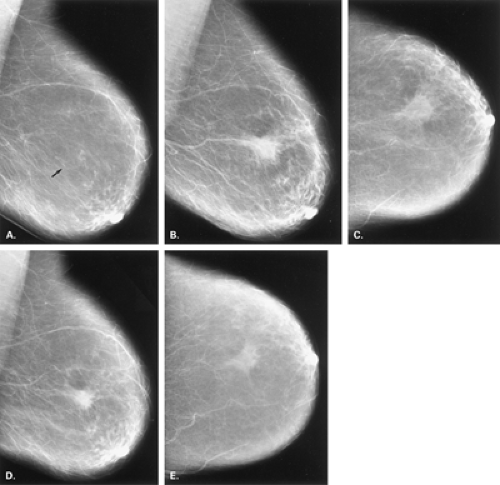 Figure 12.6 HISTORY: A 55-year-old gravida 0 woman for follow-up mammography after a benign biopsy in the right breast. MAMMOGRAPHY: Right MLO film (preoperative) (A), right MLO (B) and CC (C) view 6 months after biopsy, and right MLO (D) and CC (E) views 12 months after biopsy. The preoperative film (A) demonstrates a small cluster (arrow) of microcalcifications that were biopsied and found to be benign. On the initial postoperative study (B and C), there is a 3-cm ill-defined area of increased density in the right middle-outer quadrant. On the CC view (C), the area is of lower density than would be expected for a neoplastic process. Because the location of the biopsy was in this area, the density is most consistent with scar and fat necrosis. Six months later (D and E), the area of that fat necrosis has decreased in size, as would be expected for normal postoperative changes. IMPRESSION: Postoperative fat necrosis and scar, decreasing in size. |
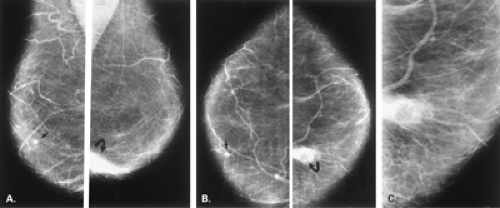 Figure 12.7 HISTORY: A 32-year-old gravida 0 woman who had had breast reduction 3 years ago, presenting with a firm irregular nodule in the right lower-inner quadrant. MAMMOGRAPHY: Bilateral MLO (A), CC (B), and enlarged (2÷) right CC (C) views. The breasts show fatty replacement. In the right lower-inner quadrant, there is an irregular area of increased density associated with a radiolucent mass containing eggshell calcification in the wall (curved arrow). A radiolucent lesion is typical of an oil cyst and is most consistent with posttraumatic changes from reduction mammoplasty. The area was biopsied because of clinical concern about the palpable findings. Incidental note is also made of a small degenerating fibroadenoma in the left middle-inner quadrant (arrow). IMPRESSION: Fat necrosis, oil cyst. HISTOPATHOLOGY: Fat necrosis. |
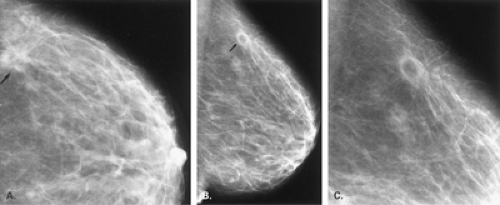 Figure 12.8 HISTORY: A 78-year-old gravida 2, para 2 woman after right breast biopsy for microcalcifications that were found to be epithelial hyperplasia, presenting for routine follow-up. MAMMOGRAPHY: Right enlarged (2÷) CC view (A) 6 months postoperatively and right MLO (B) and enlarged XCCL (C) views 12 months postoperatively. On the initial study (A), there is an irregular area (arrow) of increased density in the outer aspect of the breast. This corresponded in location to the scar and was presumed to represent fat necrosis. Six months later (B and C), the density has resolved and has been replaced by a lucent mass with a calcifying rim (B, arrow), consistent with an oil cyst. IMPRESSION: Postoperative fat necrosis evolving into an oil cyst. |
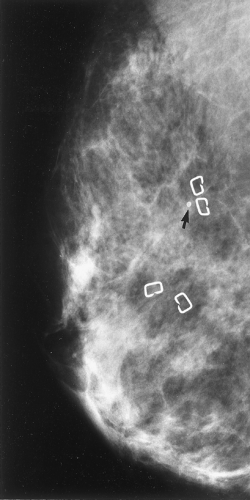 Figure 12.9 HISTORY: A 52-year-old woman 5 years after treatment for intraductal carcinoma of the left breast with lumpectomy and radiation therapy. MAMMOGRAPHY: Left MLO view. The breast is moderately dense. Surgical clips have been placed at the lumpectomy site to outline the tumor bed for radiation therapy planning. A single calcification of fat necrosis (arrow) is noted at the tumor bed. IMPRESSION: Foreign bodies: surgical clips marking tumor bed. |
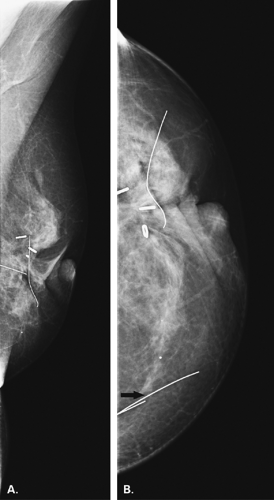 Figure 12.10 HISTORY: A 64-year-old woman status postlumpectomy and radiotherapy for right breast ductal carcinoma. MAMMOGRAPHY: Right MLO (A) and CC (B) views show marked distortion and skin retraction related to postsurgical scarring. Surgical clips demonstrate the tumor bed, and wires have been placed on the skin to mark the surgical scars. In the medial aspect of the breast is a segment of the hook wire (arrow) used during a prior needle localization. The wire was present for three subsequent years and has not been associated with any side effects. IMPRESSION: Posttreatment changes, retained segment of localization hook wire. |
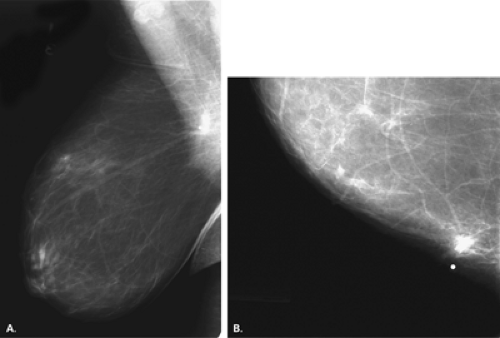 Figure 12.11 HISTORY: A 24-year-old woman with acute leukemia and neutropenia, presenting with a 2 ×2-cm tender mass in the left upper-inner quadrant. (A BB was placed over the palpable lesion for mammography). MAMMOGRAPHY: Left MLO view (A) and left enlarged (2÷) CC view (B). There are scattered fibroglandular densities present. Far posteriorly in the upper inner quadrant in the area of palpable mass is a tubular intraparenchymal artifact. Some surrounding increased density is present (A and B). This tubular structure is the tip of a catheter for chemotherapy, which had been removed several months earlier. The tip was severed and remained in the breast and had not been clinically evident until the surrounding inflammation occurred. IMPRESSION: Catheter tip with surrounding inflammatory changes. |
When one is interpreting a spiculated density as a postsurgical change, it is important to review the mammogram before biopsy to confirm that the lesion removed was in fact in the area of concern and, if nonpalpable, was present in the specimen. The most helpful factor that can aid one in making the diagnosis of “postsurgical change” on subsequent studies is a mammogram at 3 to 6 months after biopsy (1). This is particularly important when the biopsy demonstrated an atypical lesion.
Calcifications of fat necrosis form at variable times after biopsy but usually later than 6 months. These calcifications are typically ringlike, with lucent centers, and may be small (liponecrosis macrocystica calcificans) or larger oil cysts (radiolucent masses with eggshell calcifications). Occasionally, fat necrosis may be associated with clumps of irregular but rather coarse microcalcifications. Other forms of calcification that occur postoperatively include ringlike dermal calcifications in the scar, particularly in keloids. Calcified sutures, which are in linear or knot
shapes, are observed postoperatively but more frequently in patients treated with radiotherapy (5).
shapes, are observed postoperatively but more frequently in patients treated with radiotherapy (5).
Foreign bodies left in the breast include surgical clips (often used for marking a tumor bed for location of a boost dose of radiotherapy) and sutures that may calcify. Inadvertent transection of a needle localization wire and lack of its retrieval will result in the observation of a small segment of wire in the breast. Another cause of an iatrogenic foreign body in the breast is the inadvertent severing of the tip or cuff of a central venous catheter for chemotherapy, which may be embedded in the upper inner aspect of the breast (6).
Reduction Mammoplasty
Breast reduction is performed for cosmetic reasons (to treat macromastia) or to achieve symmetry of the contralateral breast after the patient has undergone mastectomy with reconstruction. The surgical procedure involves elevation of the nipple, resection of glandular tissue, and skin removal (7). If there is a nipple transposition procedure, the nipple-areolar complex remains attached to the lactiferous ducts, and the whole complex is transposed upward. In a transplantation procedure, the nipple-areolar complex is severed from the ducts and is transplanted upward (7).
Mammographic findings vary with the type of procedure performed. In patients with a transposition, the subareolar ducts are in a normal relationship with the nipple-areolar complex, but there is a disruption of this orientation after transplantation procedures. Miller et al. (7) found parenchymal redistribution, with most of the fibroglandular tissue below the level of the nipple, as the most common finding in 24 patients who had undergone reduction mammoplasties. Elevation of the nipple was also a common finding, along with thickening of the skin of the lower aspect of the breast and the areola (7). There may be disorientation of the normal parenchymal pattern, with swirled patterns of tissue distribution (8). The scars on the skin may be evident on the mammogram as circumlinear densities traversing the inferior aspect of the breast (Figs. 12.12,12.13,12.14,12.15,12.16,12.17,12.18,12.19).
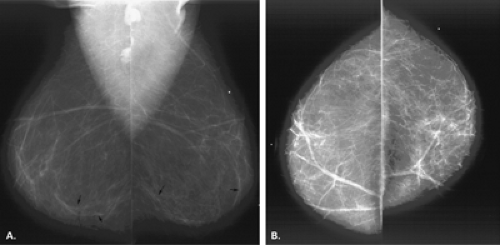 Figure 12.12 HISTORY: A 55-year-old woman who is status postreduction mammoplasty. MAMMOGRAPHY: Bilateral MLO (A) and CC (B) views show fatty-replaced breasts. There is mild distortion of the tissue with linear swirling inferiorly (arrows). The breasts have a flattened appearance on the MLO views, and the nipples are located more superiorly than in the normal state. This combination of findings is typical of postsurgical changes from reduction mammoplasty. IMPRESSION: Postoperative changes secondary to reduction mammoplasty. |
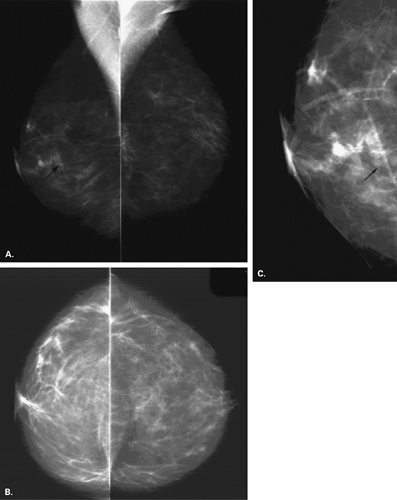 Figure 12.13 HISTORY: A 47-year-old woman is status postreduction mammoplasty, for routine screening. MAMMOGRAPHY: Bilateral MLO (A) and CC (B) views show scattered fibroglandular densities. The breasts have a somewhat flattened appearance on the MLO views, and the nipples are situated higher than in the normal state. There are linear densities (arrows) inferiorly, best seen on a left MLO enlarged image (C); these represent the scar lines related to the reduction procedure. IMPRESSION: Postoperative changes from reduction mammoplasty. |
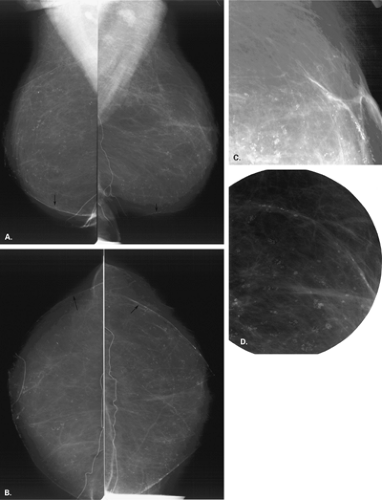 Figure 12.14 HISTORY: A 54-year-old woman status postreduction mammoplasty, for screening mammography. MAMMOGRAPHY: On MLO (A) and CC (B) views, the breasts are primarily fatty replaced. There is some distortion of the architecture, with linear structures (arrow) traversing the inferior aspects of the breasts, consistent with postsurgical scars. The nipple areolar complex is located higher than usual. Extensive calcifications are present bilaterally, which on magnification views (C, D) are lucent centered and grouped as well as extending along the scar lines. IMPRESSION: Postreduction mammoplasty changes with extensive dermal calcifications. |
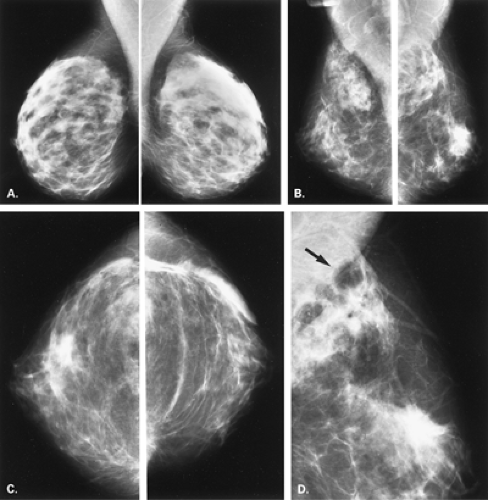 Figure 12.15 HISTORY: A 36-year-old woman who underwent reduction mammoplasties, for routine follow-up. MAMMOGRAPHY: Baseline preoperative bilateral MLO views (A), MLO (B) and CC (C) views 1 year postoperatively, and enlarged (2÷) right MLO view (D) 2 years postoperatively. On the baseline mammogram (A), the breasts are composed of dense, symmetrical fibroglandular tissue. After reduction (B and C), a large amount of fibroglandular tissue has been removed, and there is disorientation of the remaining tissue and elevation of the nipple, consistent with normal changes after the procedure. This pattern should suggest to one the findings of a reduction procedure, even without knowledge of the clinical history. One year later (D), there has been interval development of multiple oil cysts (arrow) and some smaller coarse calcifications of fat necrosis in the upper outer quadrant. IMPRESSION: Postreduction changes, with development of fat necrosis. (Case courtesy of Dr. Cherie Scheer, Richmond, VA. ) |
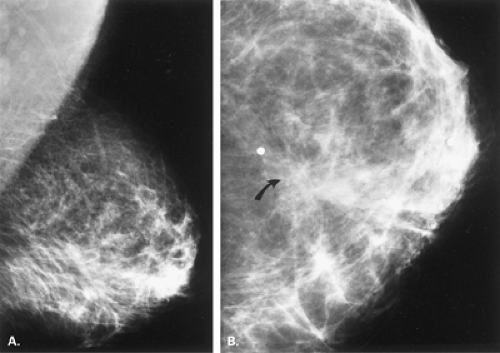 Figure 12.16 HISTORY: A 44-year-old gravida 3, para 3 woman after left mastectomy and reduction mammoplasty on the right. MAMMOGRAPHY: Right MLO (A) and CC (B) views. There is distortion of normal architecture with disturbance of the normal orientation of the ducts toward the nipple. In the lower central aspect of the right breast, there is focal irregular increased density (B, arrow) along the direction of the reduction scar (marked by BBs). This finding is typical of the fat necrosis and scarring that is seen after reduction mammoplasty. IMPRESSION: Postoperative changes after reduction mammoplasty. |
Mandrekas et al. (9) described fat necrosis in 1.7% of patients following breast reduction. These patients all presented with a palpable mass that was located deep in the breast near the pectoralis major muscle. The lesion resembled a cancer on mammography and ultrasound.
Brown et al. (10) found that periareolar soft tissue changes and inferior pole alterations were present at 6 months in nearly all of 42 patients following breast reduction, and these findings regressed on subsequent studies. In 50% of patients, calcifications occurred after 2 years. In 10% of patients, there was evidence of fat necrosis on mammography.
Calcifications are a common finding in patients who have had breast reductions (3). Dermal calcifications, which are smooth and round, may occur in the areola (7) or in scars. Areas of fat necrosis are more common in patients who have undergone reduction than those who have had routine biopsies. Calcifications may be eggshell shaped in the walls of oil cysts or may be irregular (11) or even lacy in appearance (Fig. 12.20). The calcifications may be extensive and have a coarse pleomorphic appearance, sometimes raising a concern for cancer because of the pleomorphism. Importantly, these calcifications are oriented in the direction of the scars, and correlation with this distribution is helpful in confirming their etiology. Even sutural calcification may be identified after reduction procedures (8) (Fig. 12.21).
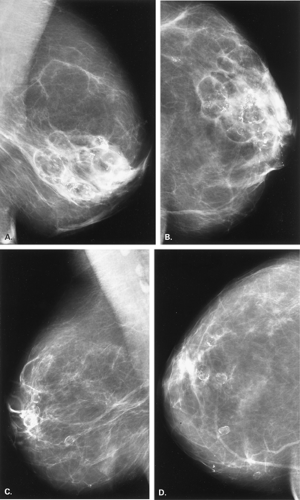 Figure 12.17 HISTORY: A 45-year-old woman after bilateral reduction mammoplasties, with firm nodularity in both subareolar areas. MAMMOGRAPHY: Right MLO (A) and CC (B) views and left MLO (C) and CC (D) views. The breasts show primarily fatty replacement. There are extensive areas of calcification in both breasts, more prominent on the right than on the left. Many of the calcifications are thin eggshell or rimlike in areas of liponecrosis macrocystica (fat necrosis). On the right (A and B
Get Clinical Tree app for offline access
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|
