Advances in the biology of melanoma have provided insights about chemoresistance and its genetic heterogeneity in parallel with advances in drug design, culminating in recent major treatment breakthroughs. Although clinical benefit of targeted therapies has been unquestionable, future advances are only possible if we understand the interplay between genetic aberrations and role of other crucial nongenetic changes yet to be identified by such projects as the Cancer Genome Atlas Project in Melanoma. Combination therapies, either among small molecule inhibitors themselves and/or with immunotherapies, may be the optimal strategy to prevent development of drug resistance inherently linked with such targeted therapies.
Key points
- •
Although melanoma bears one of the highest number of mutations per given DNA length among other malignancies, the most abundant mutations primarily affect 2 major signaling pathways.
- •
Next-generation sequencing methodologies targeting a panel of cancer-related genes may better capture heterogeneity of melanoma and assist in treatment decisions.
- •
Several genetic aberrations (mutations, copy number aberrations) can coexist within a particular melanoma, which may be of prognostic and therapeutic significance.
- •
Although BRAF-mutant melanomas have been the most successful melanoma subset for targeted therapies, progress is ongoing for other melanoma subtypes as well (e.g., RAS mutant, ocular).
- •
Treatment strategies are more successful in preventing than treating secondary drug resistance; combination treatments among targeted therapies and/or with immunotherapies may be more successful than single-agent approaches.
Introduction
Similar to those for other cancers, targeted therapies for malignant melanoma (MM) have only been under investigation for a little more than a decade. Before 2010, treatment of MM had achieved minimal progress since the 1970s, when dacarbazine was approved, and when a “one-size-fits-all” approach with various chemotherapeutic approaches had been applied to nearly all cancers. In clinical trial after clinical trial, chemotherapies in MM were proved to be largely ineffective compared with dacarbazine. In fact, the minimal clinical benefit from systemic treatments was so predictable that clinical efficacy benchmarks were built around the statistical design for future phase II clinical trials in MM. During this frustrating era, few immunotherapies were proved to be promising with durable clinical benefit in a small subset of patients with MM or high risk for relapse melanoma. More than any other time from the past, treatment of MM is currently being shaped around targeted therapies administered in particular melanoma subgroups, given in precisely defined schedules, alone or in combination with other targeted therapies or various other immunotherapeutic approaches.
A Better Understanding of the Biology of Melanoma Was the Driving Force Behind the Clinical Development of Targeted Therapies
It is becoming increasingly understood that cancers have distinct aberrations in particular cellular processes, in particular DNA repair pathways, which make them either relatively sensitive or refractory to systemic chemotherapies. Melanoma has one of the highest mutation frequencies and frequently shows elevated expression of DNA repair proteins. Four important points are remarkable with respect to genetic aberrations in melanoma:
- 1.
Only a handful of genes are more frequently mutated ( Fig. 1 ) or show gene copy number alterations (amplifications or deletions, Fig. 2 ) than others, whereas the clinical importance of most other genetic aberrations is currently unclear.
Fig. 1
Frequency of somatic mutations that were previously identified in the work presented in the Hodis and colleagues article and applied in the publicly available cohort of cutaneous melanoma samples that has been collected as part of the Cancer Genome Atlas Project. Only 257 out of the so far (August 17, 2014) analyzed 375 samples that bear mutations ( green dots ) in any of these genes are shown. Neurofibromatosis 1 gene (NF1), HRAS, and KRAS are also presented to emphasize the 4 emerging subgroups on the basis of BRAF, RAS, and NF1 mutations, versus no mutation (triple wild-type group). Mutations highlighted with red border signify noncanonical mutations. Most genes, highlighted in red, are components of the BRAF/MEK/ERK, or PI3K/Akt signaling (see Fig. 3 for further details). Analysis was performed using the cBioportal for Cancer Genomics ( www.cbioportal.org ) in compliance with early publication of results from the website, as per Cerami and colleagues and Gao and colleagues.
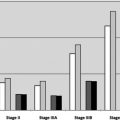
Fig. 2
Frequency of gene copy number alterations that were previously identified in the work presented in the Hodis and colleagues and applied in the publicly available cohort of cutaneous melanoma samples that has been collected as part of the Cancer Genome Atlas Project. Only 145 out of the so far (August 17, 2014) analyzed 375 sample that bear gene amplifications ( red bars ), or gene deletions ( blue bars ) in any of these genes are shown. Samples with BRAF ( red dots ), RAS ( green dots ), or neurofibromatosis 1 gene (NF1; purple dots ) mutations are also shown for associations. Analysis was performed using the cBioportal for Cancer Genomics ( www.cbioportal.org ) in compliance with early publication of results from the website, as per Cerami and colleagues and Gao and colleagues.
- 2.
Although most frequently mutated genes bear mutational “hotspots” (“canonical” mutations), increasing evidence suggests the presence of noncanonical mutations (see Fig. 1 ) that can only be identified using next-generation sequencing methodologies.
- 3.
The most frequently mutated genes are components of 2 principal signaling pathways, the Ras–Raf–MEK–ERK and the PI3K–mTOR signaling pathway ( Fig. 3 ). The activation status of these kinases within each of these pathways is not independent from each other and dynamically adjusts to environmental changes, including targeted treatments.
Fig. 3
Cellular processes disrupted in melanoma as a result of genetic aberrations (mutations or gene copy number alterations). See Figs. 1 and 2 for details regarding the type and frequency of genetic aberrations. Red lines indicate inhibition; blue and black indicate activation. mTOR, mammalian target of rapamycin; PTEN, protein tyrosine phosphatase; RTK, receptor tyrosine kinase.
- 4.
The most frequently occurring mutations BRAF and RAS proteins are paradoxically not related to sun exposure, can be found in early stages of melanoma, or even premalignant conditions, and are retained during later stages of melanoma.
- 5.
More than 1 mutation and/or gene copy alteration can coexist within a melanoma, which can have important clinical implications (see Figs. 1 and 2 ).
- 6.
Response to immunotherapies is independent from mutational status.
In preliminary analyses of mutations of more than 350 cutaneous melanoma specimens as part of the Cancer Genome Atlas, cutaneous melanomas can be conventionally classified in 4 different mutational groups (see Fig. 1 ) :
- 1.
“Hotspot” mutations in the BRAFV600 as well as immediately adjacent codons;
- 2.
“Hotspot” mutations of the RAS oncogenes (N-, K-, or H-RAS) with the predominance of those occurring in NRAS (>90%);
- 3.
Mutations of the neurofibromatosis 1 gene (NF1), an inhibitor of RAS signaling ( Fig. 4 ) without any concurrent hotspot mutations in the BRAF and NRAS (approximately 10%); and
Fig. 4
Simplified diagram on the regulation of the RAS superfamily of small GTPases and the role of neurofibromatosis 1 gene (NF1). RAS proteins become active versus inactive if bound to GTP and GDP, respectively. Extracellular growth factor signals ( red circle ) are transmitted through growth factor receptors ( light blue ) to guanine nucleotide exchange factors (GEF), which activate RAS ( red ) by exchanging GDP for GTP. In contrast, GTPase activating proteins, including NF1, tend to keep RAS proteins in their inactive state ( light blue ). Please note the promiscuity of RAS signaling, which activate several signaling pathways, including the MAPK as well as the PI3K-Akt pathway.
- 4.
No mutations in any of these genes.
Introduction
Similar to those for other cancers, targeted therapies for malignant melanoma (MM) have only been under investigation for a little more than a decade. Before 2010, treatment of MM had achieved minimal progress since the 1970s, when dacarbazine was approved, and when a “one-size-fits-all” approach with various chemotherapeutic approaches had been applied to nearly all cancers. In clinical trial after clinical trial, chemotherapies in MM were proved to be largely ineffective compared with dacarbazine. In fact, the minimal clinical benefit from systemic treatments was so predictable that clinical efficacy benchmarks were built around the statistical design for future phase II clinical trials in MM. During this frustrating era, few immunotherapies were proved to be promising with durable clinical benefit in a small subset of patients with MM or high risk for relapse melanoma. More than any other time from the past, treatment of MM is currently being shaped around targeted therapies administered in particular melanoma subgroups, given in precisely defined schedules, alone or in combination with other targeted therapies or various other immunotherapeutic approaches.
A Better Understanding of the Biology of Melanoma Was the Driving Force Behind the Clinical Development of Targeted Therapies
It is becoming increasingly understood that cancers have distinct aberrations in particular cellular processes, in particular DNA repair pathways, which make them either relatively sensitive or refractory to systemic chemotherapies. Melanoma has one of the highest mutation frequencies and frequently shows elevated expression of DNA repair proteins. Four important points are remarkable with respect to genetic aberrations in melanoma:
- 1.
Only a handful of genes are more frequently mutated ( Fig. 1 ) or show gene copy number alterations (amplifications or deletions, Fig. 2 ) than others, whereas the clinical importance of most other genetic aberrations is currently unclear.
Fig. 1
Frequency of somatic mutations that were previously identified in the work presented in the Hodis and colleagues article and applied in the publicly available cohort of cutaneous melanoma samples that has been collected as part of the Cancer Genome Atlas Project. Only 257 out of the so far (August 17, 2014) analyzed 375 samples that bear mutations ( green dots ) in any of these genes are shown. Neurofibromatosis 1 gene (NF1), HRAS, and KRAS are also presented to emphasize the 4 emerging subgroups on the basis of BRAF, RAS, and NF1 mutations, versus no mutation (triple wild-type group). Mutations highlighted with red border signify noncanonical mutations. Most genes, highlighted in red, are components of the BRAF/MEK/ERK, or PI3K/Akt signaling (see Fig. 3 for further details). Analysis was performed using the cBioportal for Cancer Genomics ( www.cbioportal.org ) in compliance with early publication of results from the website, as per Cerami and colleagues and Gao and colleagues.
Fig. 2
Frequency of gene copy number alterations that were previously identified in the work presented in the Hodis and colleagues and applied in the publicly available cohort of cutaneous melanoma samples that has been collected as part of the Cancer Genome Atlas Project. Only 145 out of the so far (August 17, 2014) analyzed 375 sample that bear gene amplifications ( red bars ), or gene deletions ( blue bars ) in any of these genes are shown. Samples with BRAF ( red dots ), RAS ( green dots ), or neurofibromatosis 1 gene (NF1; purple dots ) mutations are also shown for associations. Analysis was performed using the cBioportal for Cancer Genomics ( www.cbioportal.org ) in compliance with early publication of results from the website, as per Cerami and colleagues and Gao and colleagues.
- 2.
Although most frequently mutated genes bear mutational “hotspots” (“canonical” mutations), increasing evidence suggests the presence of noncanonical mutations (see Fig. 1 ) that can only be identified using next-generation sequencing methodologies.
- 3.
The most frequently mutated genes are components of 2 principal signaling pathways, the Ras–Raf–MEK–ERK and the PI3K–mTOR signaling pathway ( Fig. 3 ). The activation status of these kinases within each of these pathways is not independent from each other and dynamically adjusts to environmental changes, including targeted treatments.
Fig. 3
Cellular processes disrupted in melanoma as a result of genetic aberrations (mutations or gene copy number alterations). See Figs. 1 and 2 for details regarding the type and frequency of genetic aberrations. Red lines indicate inhibition; blue and black indicate activation. mTOR, mammalian target of rapamycin; PTEN, protein tyrosine phosphatase; RTK, receptor tyrosine kinase.
- 4.
The most frequently occurring mutations BRAF and RAS proteins are paradoxically not related to sun exposure, can be found in early stages of melanoma, or even premalignant conditions, and are retained during later stages of melanoma.
- 5.
More than 1 mutation and/or gene copy alteration can coexist within a melanoma, which can have important clinical implications (see Figs. 1 and 2 ).
- 6.
Response to immunotherapies is independent from mutational status.
In preliminary analyses of mutations of more than 350 cutaneous melanoma specimens as part of the Cancer Genome Atlas, cutaneous melanomas can be conventionally classified in 4 different mutational groups (see Fig. 1 ) :
- 1.
“Hotspot” mutations in the BRAFV600 as well as immediately adjacent codons;
- 2.
“Hotspot” mutations of the RAS oncogenes (N-, K-, or H-RAS) with the predominance of those occurring in NRAS (>90%);
- 3.
Mutations of the neurofibromatosis 1 gene (NF1), an inhibitor of RAS signaling ( Fig. 4 ) without any concurrent hotspot mutations in the BRAF and NRAS (approximately 10%); and