production of immunoglobulins. Defects in cell-mediated immunity characterized by impaired Th1 CD4+ T lymphocytes and/or macrophage function results in increased risk of infections with intracellular bacteria, fungi, parasites, and viruses (Table 69.2).
TABLE 69.1 HOST DEFECTS PREDISPOSING TO COMPLICATIONS IN HEMATOLOGIC MALIGNANCIES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
either a primary or a secondary immune response, whereas those with CLL maintain secondary responses but cannot mount a primary response. Depressed cellular immunity is uncommon in AL16 except during maintenance therapy in ALL.17
TABLE 69.2 OPPORTUNISTIC INFECTIONS ASSOCIATED WITH DEFECTS IN IMMUNITY IN HEMATOLOGIC NEOPLASIA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
as examination of cerebrospinal fluid, may be necessary in selected patients. Noninfectious causes such as drug reactions, mucositis, graft-versus-host disease (GVHD) should be considered in patients with persistent fever. Superinfection with fungi or Clostridium difficile needs to be considered as well. Frequent reassessment of the patient’s clinical status will help determine whether there is a need for additional coverage or changes to the ongoing antimicrobial regimen.
TABLE 69.3 THE MASCC RISK INDEX SCORE: DETERMINING THE RISK OF SERIOUS COMPLICATIONS IN FEBRILE NEUTROPENIA | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
TABLE 69.4 EVALUATION OF FEVER IN IMMUNOCOMPROMISED PATIENTS | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
patients compared with controls, and thus concluded that cefepime remains a reasonable option for treating febrile neutropenia.28,29
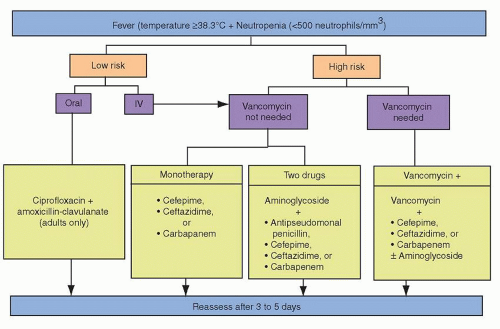 FIGURE 69.1. Empiric antibiotic regimens in febrile neutropenia. |
atypical fungi, and several clinically relevant Candida species (C. krusei, C. tropicalis, C. lusitaniae, and Torulopsis glabrata) due to the absent or poor activity of fluconazole against these organisms.
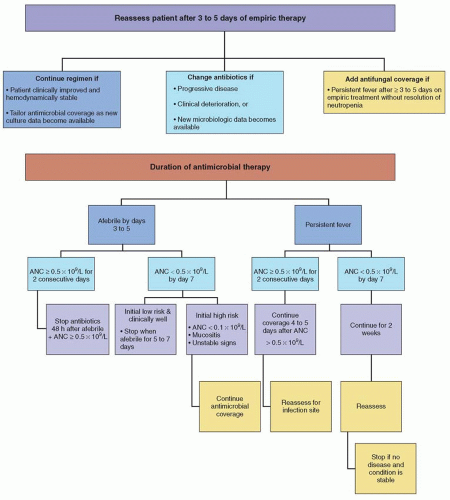 FIGURE 69.2. Common modifications of empiric antimicrobial therapy in the febrile neutropenic patient. |
factors to treat episodes of febrile neutropenia unless patients are at high risk for infection-related complications, such as those older than 65 years, or those with prolonged (>10 days) and profound (<0.1 × 109/L) neutropenia, active infection, hypotension, and/or multiorgan dysfunction39,40 (Fig. 69.3).
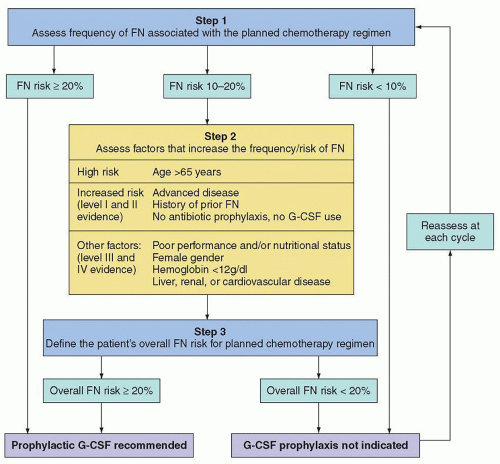 FIGURE 69.3. Algorithm to decide prophylactic G-CSF usage. FN, febrile neutropenia; G-CSF, granulocyte colony-stimulating factor. (With permission from Aapro MS, Bohlius J, Cameron DA, et al. 2010 update of EORTC guidelines for the use of granulocyte colony-stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur J Cancer 2011;47:8-32.) |
from a large meta-analysis found dexamethasone to not provide significant reductions in death or neurologic sequelae, although a statistically significant reduction in hearing loss was observed among surviving patients.97 ISDA guidelines for the management of bacterial meningitis support the incorporation of adjuvant dexamethasone in pediatric patients with H. influenzae type B meningitis and in adult patients with pneumococcal meningitis.95
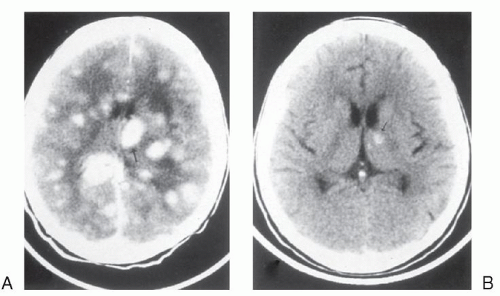 FIGURE 69.4. Central nervous system toxoplasmosis: magnetic resonance imaging study of the brain before therapy (A) and after therapy (B) with pyrimethamine and sulfadiazine. |
rates in patients refractory or intolerant to triazoles or amphotericin B.141 Posaconazole has been used successfully as salvage therapy for a variety of invasive fungal infections refractory to standard therapy.142 Posaconazole is currently approved by the FDA for prophylaxis of invasive Aspergillus and Candida infections, and in the European Union is indicated for treatment of invasive aspergillosis and other invasive fungal infections refractory to standard antifungal agents.143
TABLE 69.5 DIFFERENTIAL DIAGNOSIS OF PULMONARY INFILTRATE IN THE IMMUNOCOMPROMISED PATIENT | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||
sensitive and specific.144 Antibody detection may also be useful, but false-negative results may occur in immunocompromised patients.145 Biopsy specimens showing small intracellular or narrow budding yeast are suggestive of the diagnosis and should be confirmed by culture. IDSA guidelines recommend amphotericin B for severe pulmonary or disseminated histoplasmosis.145 Prolonged therapy with itraconazole may be initiated after stabilization of disease, and should be continued for the duration of immunosuppression.145
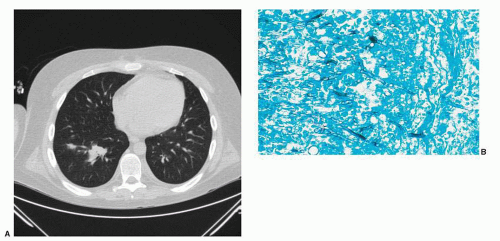 FIGURE 69.5. A: Chest CT of a hematopoietic cell transplant recipient who developed pulmonary Aspergillus infection after prolonged immunosuppression. B: Photomicrograph of the characteristic 45° angle branching of septate hyphal forms of Aspergillus. Gomori methenamine silver stain, × 400. (Courtesy of Margie Scott.) |
multidrug-resistant pathogens include previous antimicrobials in the preceding 90 days, hospitalization for 2 days or more in the preceding 90 days, residing within a nursing home, chronic dialysis, home wound care, and exposure to others with multidrug-resistant pathogens.70 Initial therapy for HAP depends on severity of illness of the patient, previous antimicrobial exposures and hospitalizations, and institutional antibiogram data. Empiric therapy should include an antipseudomonal beta-lactam plus an antipseudomonal fluoroquinolone, or an aminoglycoside plus either linezolid or vancomycin to cover MRSA with subsequent tailoring of regimen once culture data becomes available.70
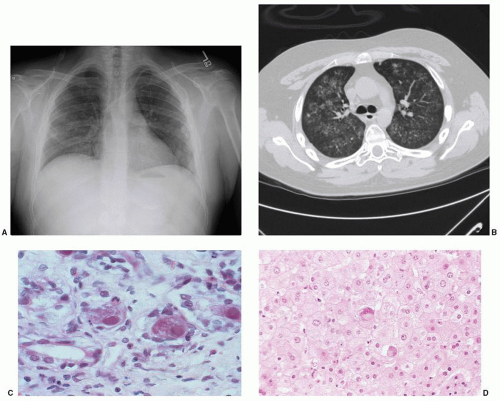 FIGURE 69.6. The spectrum of cytomegalovirus (CMV) disease in the abnormal human host. A: Chest radiograph demonstrating diffuse interstitial infiltrates in patient 60 days after cord blood transplant. B: Chest CT showing bilateral fine nodular infiltrates. C: CMV inclusion disease of the colon. Typical infected cells show cellular ballooning with dense primary nuclear inclusions surrounded by a thin, cleared rim; secondary inclusions appear as cytoplasmic granules after the nucleus has filled with virions. D: CMV hepatitis demonstrated on liver biopsy. Viral cytopathic effect may be difficult to establish, but rare viral inclusions with surrounding parenchymal changes are diagnostic of CMV. Hematoxylin and eosin stain ×400. (Photomicrographs courtesy of Margie Scott.) |
and a paralytic ileus. All patients should be assessed for C. difficile infection. Treatment requires broad-spectrum antibiotics with activity against aerobic gram-negative bacilli and anaerobes (e.g., ceftazidime plus metronidazole, imipenem, meropenem, or piperacillin/tazobactam) and supportive care, including intravenous fluids or parental nutrition and bowel rest. The majority of patients will respond to antibiotic therapy and supportive care without the need for surgery. Indications for surgery often include (1) persistent gastrointestinal bleeding after resolution of neutropenia, thrombocytopenia, and clotting abnormalities; (2) intraperitoneal perforation; (3) uncontrolled sepsis despite fluid and vasopressor support; and (4) an intraabdominal process (such as appendicitis) that would require surgery in the absence of neutropenia.163
Concurrent myalgias raise the possibility of Candida myositis. Biopsy and fungal staining of cutaneous lesions can provide an immediate clue to the diagnosis, prompting the early addition of antifungal therapy. Blood cultures are typically positive.
degree of HLA matching, stem cell source, and GVHD prophylaxis). The spectrum of pathogens to which HSCT recipients are most susceptible follows a time line corresponding to the predominant immune defects as outlined in Figure 69.7.
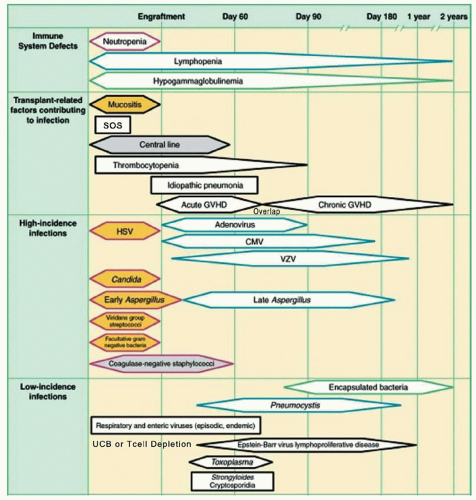 FIGURE 69.7. Phases of predictable opportunistic infections and complications among patients undergoing hematopoietic stem cell transplantation. CMV, cytomegalovirus; GVHD, graft-versus-host disease; HSV, herpes simplex virus; SOS, sinusoidal obstruction syndrome; UCB, umbilical cord blood; VZV, varicella zoster virus. Adapted from Van Burik J-AH, Freifeld AG. Infection in the severely immunocompromised host. In: Abeloff MD, Armitage JO, Niederhuber JE, et al., eds. Clinical oncology, 3rd ed. Philadelphia, PA: Churchill Livingstone; 2004:942. |
those due to gram-negative organisms, but has not been shown to definitively decrease infection-related mortality.81,176 Antibiotic prophylaxis has been found to significantly decrease the risk for all-cause mortality when compared with placebo or no treatment in neutropenic patients,81,191 IDSA and ASBMT guidelines do recommend prophylactic fluoroquinolone in high-risk patients with expected duration of neutropenia >7 days.182
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


