Step 1
Surgical Anatomy
- ♦
The pancreas is a retroperitoneal organ in the upper abdomen that slopes upward from the C-loop of the duodenum to the splenic hilum. It is commonly divided into three regions: head, body, and tail.
- ▴
The pancreatic head is intimately attached to the medial duodenum. It lies anterior to the right renal artery and veins, inferior vena cava (IVC), and superior mesenteric vessels, although a small tongue of pancreatic tissue, called the uncinate process , lies behind the superior mesenteric vessels as they emerge from the retroperitoneum. Anterior to the pancreatic head lies the first part of the duodenum and the transverse mesocolon. The common bile duct runs in a posterior groove in the head of the pancreas and passes through the pancreatic parenchyma to join the main pancreatic duct before entering the duodenum at the ampulla of Vater ( Fig. 15-1 ).
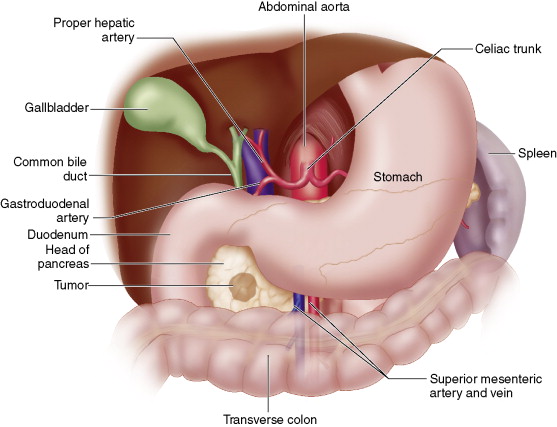
Figure 15-1
- ▴
The body of the pancreas is covered by the transverse mesocolon and stomach; it is in posterior contact with the aorta, left crus of the diaphragm, and left kidney and adrenal gland.
- ▴
The tail of the pancreas lies in the splenic hilum.
- ▴
- ♦
The blood supply to the pancreas comes from branches of the celiac and superior mesenteric arteries. The celiac axis gives rise to the common hepatic artery, which branches into the gastroduodenal and proper hepatic arteries. The gastroduodenal artery passes behind the first portion of the duodenum and branches into the anterior and posterior superior pancreaticoduodenal arteries.
- ▴
The superior pancreaticoduodenal arteries form arcades with the inferior pancreaticoduodenal arteries, which arise from the superior mesenteric artery (SMA). These arcades give off many smaller branches that supply the duodenum and head of the pancreas.
- ▴
An important arterial variation is a replaced right hepatic artery that arises from the SMA; this may be present in up to 20% of patients. Recognizing a replaced right hepatic artery is important to avoid its injury.
- ▴
The body and tail of the pancreas are supplied by the splenic artery and inferior pancreatic artery, which arises from the SMA. Connecting the splenic and inferior pancreatic arteries are three vessels that run perpendicular to the long axis of the pancreas: dorsal pancreatic, great pancreatic, and caudal pancreatic arteries.
- ▴
- ♦
Venous drainage of the pancreas runs parallel to the arterial supply, usually superficial to the arteries in the pancreatic parenchyma. The superior pancreatic head drains into the portal vein, and the inferior pancreatic head drains into the inferior mesenteric vein and superior mesenteric vein (SMV). The pancreatic body and tail drain into the splenic vein.
- ♦
Lymphatic drainage of the pancreas is diffuse along a complex network of lymphatic channels. Lymph nodes are found in peripancreatic locations along the veins, although lymphatic drainage also communicates with nodes in the transverse mesocolon and mesentery of the proximal jejunum.
- ♦
Innervation of the pancreas is from vagal and splanchnic nerves; pain is mediated by the latter in sensory fibers that travel to the celiac ganglia.
Step 2
Preoperative Considerations
- ♦
Neuroendocrine tumors of the pancreas arise from pancreatic islet cells, which comprise 1% to 2% of the pancreatic mass. Approximately 95% of islet cell tumors are insulinomas, gastrinomas, or nonfunctioning tumors. The remaining 5% produce glucagon, somatostatin, vasoactive intestinal peptide (VIP), or other pancreatic peptides.
- ♦
Once the biochemical diagnosis has been established, the tumor should be localized with radiologic studies. If there is concern about resectability of a tumor in the pancreatic head, a high-quality pancreatic protocol computed tomography (CT) scan is the best tool for determining tumor involvement with the portal and mesenteric vessels.
- ♦
The surgical approach to pancreatic neuroendocrine tumors is influenced by a number of factors, including tumor location and size, whether the tumor is benign or malignant, and whether the disease is sporadic or occurring with the multiple endocrine neoplasia type I (MEN-I) syndrome. Patients with MEN-I frequently have multiple islet cell tumors.
- ♦
Most insulinomas (95%) are benign, whereas a majority of gastrinomas (60%), glucagonomas (75%), somatostatinomas (>75%), and 50% of VIPomas are malignant. Primary tumors may occur in the duodenum as well as in the pancreas.
- ♦
Pancreatic islet cell tumors can usually be managed with enucleation or distal pancreatectomy. However, tumors in the head of the pancreas that are large or potentially malignant may require pancreatoduodenectomy.
- ♦
The surgeon should be prepared to perform intraoperative ultrasound, because pancreatic neuroendocrine tumors may be neither palpable nor visible during exploratory laparotomy.
Step 3
Operative Steps
Incision and Exposure
- ♦
Two types of incision may be used: a vertical midline incision that begins at the xiphoid and extends below the umbilicus or a bilateral subcostal incision. Both incisions can provide adequate visualization of the upper abdomen.
- ♦
The peritoneal cavity is entered and the round ligament is identified, divided between clamps, and securely ligated. Increased liver mobility may be achieved with division of the falciform ligament over the dome of the liver. A self-retaining retractor may be inserted to provide optimal exposure.
- ♦
The abdominal cavity is explored to exclude extrapancreatic metastatic disease that would contraindicate pancreatoduodenectomy.
- ♦
A Cattell-Braasch maneuver is performed by mobilizing the right colon and small bowel. The lateral peritoneal attachments of the right colon are incised, along with the visceral peritoneum to the ligament of Treitz. The right colon and small bowel are retracted cephalad, exposing the underlying duodenum and pancreatic head. The middle colic vein is ligated and divided distal to its junction with the SMV ( Fig. 15-2A ).
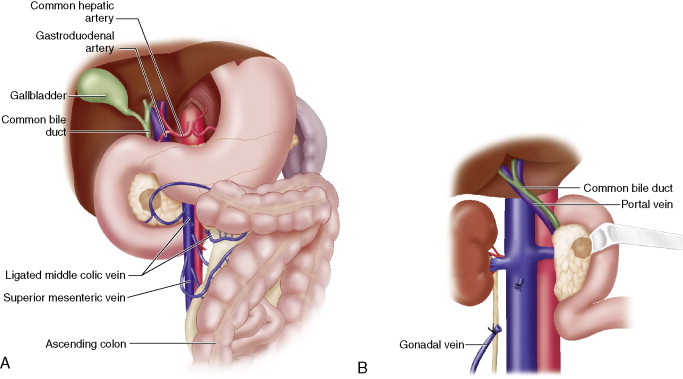
Figure 15-2
- ♦
The duodenum and head of the pancreas are mobilized using the Kocher maneuver. The duodenum is grasped with Babcock forceps and retracted medially as the lateral peritoneal attachments of the duodenum are incised. The right gonadal vein is ligated and divided at its junction with the IVC. Dissection proceeds to the left lateral edge of the aorta, taking care to avoid injury to the IVC and left renal vein. At the completion of the Kocher maneuver, the left hand may be inserted behind the pancreatic head to assess the relationship of the tumor to the SMA (see Fig. 15-2B ).
Details of Procedure
- ♦
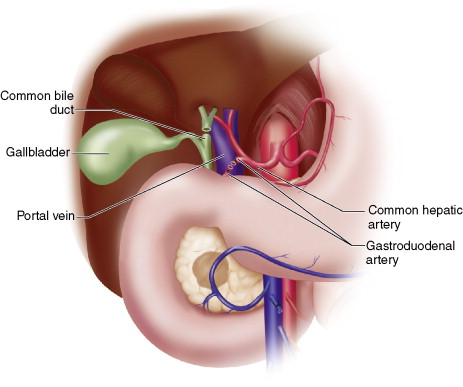
Dissection of the porta hepatis begins with exposure of the common hepatic artery proximal and distal to its junction with the gastroduodenal artery. The gastroduodenal artery is ligated and divided at its origin. The gallbladder is dissected free from the liver, and the common hepatic duct is transected just proximal to the cystic duct. The common hepatic artery is retracted medially, exposing loose connective tissue over the anterior wall of the portal vein. This loose connective tissue is divided caudally to the junction of the portal vein and neck of the pancreas. Care must be taken to avoid injury to the portal vein at this time ( Fig. 15-3 ).
Related posts:
 Minimally Invasive Parathyroidectomy
Minimally Invasive Parathyroidectomy
 Surgical Anatomy, Intraoperative Neural Monitoring, and Operative Management of the RLN and SLN
Surgical Anatomy, Intraoperative Neural Monitoring, and Operative Management of the RLN and SLN
 Thyroidectomy for Large or Substernal Goiters
Thyroidectomy for Large or Substernal Goiters
 Minimally Invasive Parathyroidectomy : Gamma Probe Guided *
Minimally Invasive Parathyroidectomy : Gamma Probe Guided *
 Laparoscopic Pancreatic Enucleation or Resection for Neuroendocrine Tumor
Laparoscopic Pancreatic Enucleation or Resection for Neuroendocrine Tumor
 Thyroidectomy for Nodules or Small Cancers
Thyroidectomy for Nodules or Small Cancers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


