Breast cancer is still the most common cancer in women and nearly half of those diagnosed will die from it. The American Cancer Society estimates that in 2013 there will be 234,580 new cases of breast cancer and 40,340 deaths in the United States. (1). All oncologists do palliative care, but we can improve the end of life care of our patients by adapting some of the techniques of hospice and palliative medicine (2). In this chapter we will review the following: evolving models of care; predicting end of life; communication issues; incorporation of hospice and advance care planning into standard care; symptom and pain management; managing the time right before death; helping with caregivers; and end with a management summary.
EVOLVING MODELS OF CARE
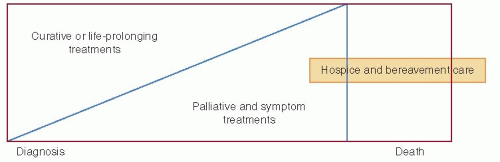
The models of care for breast cancer patients have changed in the past decades, both during active treatment and near the end of life. The current suggested model of care (3) is shown in Figure 73-1, and illustrates that disease-directed treatment is given concurrently with palliative care along the time course of treatment, with palliative care and hospice care assuming a greater role if the patient is dying.
The American Society of Clinical Oncology (4) and the National Comprehensive Cancer Center Network (NCCN) guidelines (5) now call for concurrent palliative care for all people with serious illness. The recommendations for concurrent care are based on the evidence from multiple randomized clinical trials and show benefits including better quality of life for patients and families; less aggressive end of life care including less death in the hospital; more deaths at the place of one’s choice; increased use of hospice; improved communication; improved symptom control; and possibly better survival with no trials showing worse survival.
PREDICTING END OF LIFE: WHY IT IS IMPORTANT, AND HOW TO PREDICT ACCURATELY
Nearly all modern-day breast and other cancer patients want to know their prognosis, treatment options, curability, and estimated length of survival. A consistent theme in a review of 46 studies is that most patients will want this information at the onset, but with some negotiation about the content and extent of the information as the disease progresses (6).
The reason to give people information about their prognosis is to help them with decision making. We have known for decades (7) that people who understood that they had less than 6 months to live, compared to those who do not, lived just as long and are far more likely to die a “good” death. Those who overestimated their survival and wanted life-extending treatments rather than symptom management are 1.6 times more likely to die on a ventilator or with resuscitation, and be readmitted to the hospital. All of these, including chemotherapy in the last weeks of life for breast cancer patients, are considered a sign of poor quality of care (8).
The American Society of Clinical Oncology has made recommendations that oncologists have frank, personalized discussions with patients about prognosis, treatment outcomes, and end of life care transitions, and that such discussions are particularly important near the end of life (9). As stated by ASCO, “Central to all of these goals is the need for realistic conversations about options and alternatives that should occur throughout the course of the patient’s illness. Such conversations may currently occur in less than 40% of patients with advanced cancer. All patients are owed comprehensive information about their prognosis and treatment options, with the amount of detail tailored to the individual patient. All patients must have a regular opportunity to make their preferences about how to live their final weeks and months clear to their oncologist. Given that the default care plan in the absence of these conversations is often further systemic therapy, there is a need to regularly and specifically address the question of whether further anticancer-directed therapy is consistent with the patient’s wishes and the current clinical picture. Only through these discussions do we have the opportunity to match patients’ goals with the actual care delivered.”
FIGURE 73-1 The changing patterns of care that incorporate palliative and end of life care.
The ability to predict when a person with breast cancer is potentially facing the end of life is straightforward, based on the available evidence. Any person with metastatic breast cancer is facing a terminal illness, and for most patients with HER-2 negative cancer the average survival is still less than 2 years. There is no known harm to addressing end of life issues earlier rather than later, other than the discomfort of raising the issues for patients, families, and healthcare professionals.
Performance status remains one of the best predictors of survival of less than 6 months, regardless of whether Karnofsky (score <60) or ECOG (score >2) is used, and the predictive value has not changed much in the past 30 years. Salpeter and colleagues (10) also note uniform average survival of less than 6 months with any of the following: poor performance status, multiple brain metastases, leptomeningeal disease, spinal cord compression, peritoneal disease and ascites, and progressive disease on chemotherapy, as shown in Table 73-1. All of these are common occurrences in breast cancer and should trigger the recognition that the disease course has changed from stability to predictable end of life.
There are other prognostic aids in common use by palliative care specialists and increasingly by oncologists. The Palliative Performance Scale gives 100 to 0 (PPS, 100 is normal function, 0 is death) scores based on routine clinical observations and is reliable, valid, and accurate. In Ontario, 25% of cancer patients died within 6 months of their first clinical encounter, and the PPS was highly predictive of death (11). For each 10-point decline in the PPS, the hazard of death increased by a factor of 1.7. The PPS is being tested as a referral trigger for palliative care and hospice consultation.
COMMUNICATION ISSUES AND THE SUBSEQUENT PATTERNS OF CARE
Despite our ability to predict with reasonable certainty, and a decades-long emphasis on honest prognostic information, ASCO notes that fewer than 40% of patients receive such information. Only 37% of dying patients remembered a conversation with their oncologist about dying (12). In a more recent study, only 22% of oncologists documented any “end of life” conversations, most such conversations were held by doctors other than the oncologist, and only 33 days before death (13). Half of all oncologists prefer to wait till “no more treatment options are left” before having these conversations (14). Nearly three-quarters of lung and colorectal cancer patients with incurable disease thought a person like themselves could be cured (15). The available data suggests that breast cancer patients have just as many unmet communication needs.
We have listed, in Table 73-2, some of the barriers that oncologists perceive. The skills to conduct these difficult discussions, such as how to be empathic listeners and to break bad news effectively, are readily learnable from programs such as Oncotalk (16). Other options include the free Education in Palliative and End-of-life Care (EPEC®)-Oncology course (http://www.cancer.gov/aboutnci/epeco) available from the National Cancer Institute.
Negotiating the palliative care conversation can be difficult, and introducing hospice services can be particularly stress-producing. We have created a guide for carrying out such discussions as shown in Table 73-3. The discussion goes easier if we have a script, just like with adjuvant treatment or lumpectomy versus mastectomy.
Goals of care and hospice discussions can be challenging for both patients and providers. Here are some tips for enhancing the quality of these conversations: First, listen for clues. Knowing they have a serious illness, most patients have thought about death and dying and are looking for permission to openly speak about it. Listen closely to the responses patients give you as their comments about mortality are not always straightforward. When given a vague statement (“I’ve been thinking about life and what this all means.”), rather than overlooking the comment ask, “Tell me more about what you mean.” Second, restate the patient’s goals. Restating, or summarizing, patient’s comments minimizes misconceptions, emphasizes the goals as important to the provider, and demonstrates attentive listening. This also provides patients with the opportunity to clarify and elaborate on their goals. Finally, Ask, Tell, Ask. (Always ask people how much they want to know, and what they do know. Then tell them, in understandable words. Ask “Now that we have discussed this, what is your understanding of your situation?”)
In reality, this is not one talk but a series of discussions at predictable transition points (17). We have outlined these in Figure 73-2.
To date, every study shows that most breast cancer patients want to have all the available information, and will tell us if they do not. Most of us use Adjuvant!, the decision-making tool that has been shown to be useable, well accepted, and lead to better decision making. Most of us print the decision aids to share with the patient. The same types of decision aids have been tested in metastatic breast cancer with good acceptance, no distress, and no harm. They want to know the details, and the survival, so that they can plan just like with adjuvant treatment.
TABLE 73-1 Predicting Survival of Breast Cancer Patients with Metastatic Disease
Setting
Prediction Models
Comment
HER-2 not amplified
1st line modern treatments gave median survival of 19-22 months 2nd line modern chemotherapy gave median survival 16-18 months. (RIBBON-2 Trial) 3rd line chemotherapy with best option eribulin gave median survival of 13 months, versus 10 months with other regimens
Since treatment is not curative, discussing advance directives at the start of metastatic cancer is appropriate. Remember that these figures are from clinical trial patients with ECOG 0-1 and no comorbidities.
Triple negative
11-12 months overall survival in contemporary US patients treated at the best centers
Specific situations with less than 6 months
Any metastatic cancer with
KPS <60 ECOG performance status ≥2 Peritoneal or leptomeningeal metastases Hypercalcemia >11.2 mg/dL Spinal cord compression with decreased ability to walk Serum C-reactive protein >10 mg/L and serum albumin <3.5 g/dL
See review by Salpeter et al., 2012 and the supplemental data file available at http://online.liebertpub.com/doi/suppl/10.1089/jpm.2011.0192/suppl_ file/Supp_Data.pdf
Any metastatic cancer with brain metastases and 1 or more of the following presentations
KPS <80 (ECOG performance status ≥2) ≥2 brain metastases plus extracranial metastases Triple negative cancer
Any metastatic breast carcinoma with 3 or more of these presentations
KPS <80 (ECOG performance Status ≥2) Serum lactate dehydrogenase >500 IU/L Any liver metastasis At least 2 sites of metastases Disease-free interval from initial presentation to metastatic disease of <24 months. Recurrent or refractory disease after initial chemotherapy Triple negative cancer
Data from Phase III trial of doxorubicin, paclitaxel, and the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer: an intergroup trial (E1193). Sledge GW, Neuberg D, Bernardo P, et al. J Clin Oncol 2003;21(4):588; Hayes DF. Systemic treatment for metastatic breast cancer: combination chemotherapy. Up to Date, 2012; Brufsky AM, Hurvitz S, Perez E, et al. RIBBON-2: a randomized, double-blind, placebo-controlled, phase III trial evaluating the efficacy and safety of bevacizumab in combination with chemotherapy for second-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol 2011;29(32):4286-4293. Epub 2011; Cortes J, O’Shaughnessy J, Loesch D, et al. Eribulin monotherapy versus treatment of physician’s choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet 2011;377(9769): 914-23; O’Shaughnessy J, Schwartzberg LS, Danso MA, et al. A randomized phase III study of iniparib (BSI-201) in combination with gemcitabine/carboplatin (G/C) in metastatic triple-negative breast cancer (TNBC). J Clin Oncol 2011;29:(suppl; abstr 1007).
INCORPORATION OF HOSPICE AND ADVANCE CARE PLANNING INTO STANDARD CARE
Best use of hospice requires a basic understanding of the Medicare (and most insurer) hospice benefits. The hospice provider is paid about $150 a day that must include all the services provided. Inpatient hospice is reimbursed at about $500 a day and must cover all the services provided. Currently, inpatient hospice is tightly regulated and patients must have a very high likelihood of dying within 7 to 14 days. There are a few communities with “expanded access hospice” that allow chemotherapy and radiation therapy, but these must still be covered within that $150 per diem, plus charity.
The easiest way to ensure timely hospice referral is to get palliative care involved by consultation. Hospitals with an active palliative care program referred 33% of hospiceappropriate patients to hospice, while hospitals without a program referred only 1%. More use of palliative care would save New York $84 to 234 million dollars (18), allow the end of life care to mirror what people choose—if given the choice, (19) and possibly increase survival (20).
Only gold members can continue reading. Log In or Register to continue
 Breast Cancer Screening
Breast Cancer Screening
 Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
 Postmastectomy Radiation Therapy
Postmastectomy Radiation Therapy
 Preoperative Chemotherapy for Operable Breast Cancer
Preoperative Chemotherapy for Operable Breast Cancer
 Management Summary for the Care of Patients with Metastatic Breast Cancer
Management Summary for the Care of Patients with Metastatic Breast Cancer



