TECHNIQUE
Laparoscopic Distal Pancreatectomy
Setup, Access, and Initial Exposure
The patient is positioned supine with 15 degrees of reverse Trendelenburg. Whereas some advocate a right lateral decubitus position or place a bump under the left flank, we prefer a supine position that facilitates a right-to-left dissection. A total of four trocars are placed as depicted in Figure 8.1. A periumbilical incision is made, the trocar placed under direct vision, and a pneumoperitoneum established. The remaining three trocars are placed under laparoscopic visualization. The gastrocolic ligament is divided peripheral to the epiploic vessels using the harmonic scalpel, and the lesser sac is entered. The short gastric vessels are preserved, and the splenic flexure of the colon is mobilized inferiorly. Visual inspection of the anterior aspect of the pancreas is performed, and the lesion is identified either through palpation or through the use of laparoscopic ultrasonography. The stomach is sutured anteriorly to the retrocostal peritoneum to facilitate exposure.
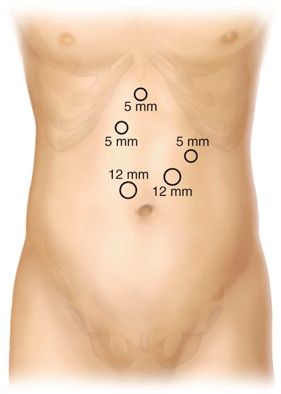
FIGURE 8.1 Trocar positioning for LDP.
Pancreatic Mobilization
The transverse mesocolon is dissected off the inferior border of the pancreas, and the pancreas is dissected out of the retroperitoneum in the anticipated area of transection. Early focus of dissection at the site of anticipated transection and splenic vessels allows excellent access and exposure for a safe dissection. In the event of bleeding during splenic vessel preservation, the vessels can be quickly ligated, reducing blood loss. The splenic vein is dissected off the posterior aspect of the pancreas. The splenic artery is identified and dissected either through an anterior approach at the superior border of the pancreas or via a posterior-inferior approach after elevating the pancreas out of the retroperitoneum. The latter approach is most commonly used when the parenchymal transection is anticipated to occur within the pancreatic body rather than the tail.
Pancreatic Resection
With the pancreas elevated off of the splenic vessels, the pancreatic parenchyma is then divided with either a linear stapler with biologic reinforcement or the harmonic scalpel. If spleen preservation is planned, the assistant retracts the pancreas anteriorly and laterally to expose the dissection plane between the pancreas and splenic vessels. Most tributary vessels can be divided with the harmonic scalpel. Larger vessels (≥2 mm) are ligated with suture or are clipped and divided. When planning splenectomy, the splenic vessels are ligated and divided near the pancreatic transection site prior to a right-to-left dissection with division of the short gastric vessels and splenic peritoneal attachments.
Specimen Retrieval
The specimen is placed in an endobag and removed via the periumbilical incision that is extended just long enough to accommodate the specimen. The specimen is inspected on the back table, and a separate pancreatic margin is harvested. We routinely use frozen section histology for evaluation of the primary lesion and the margin prior to termination of the procedure. The extraction site is closed with interrupted suture, leaving the cephalad two sutures untied. The trocar is reintroduced and the carbon dioxide (CO2) pneumoperitoneum reestablished.
Pancreatic Stump Management and Closure
When the transection is not performed with the stapler, our preferred method of pancreatic stump treatment is with saline-coupled radiofrequency energy source (Salient Surgical Technologies, Portsmouth, NH). The pancreatic resection bed and exposed splenic vessels are then reinspected, and hemostasis is ensured. Prophylactic operative drains are not routinely used in the author’s practice. The trocars are removed, and sites are closed with a 4-0 subcuticular monofilament absorbable suture.
Laparoscopic Pancreaticoduodenectomy
Setup, Access, and Initial Exposure
The patient is positioned supine in 15 degrees of reverse Trendelenburg. Initial access is gained through a left subcostal site using a 12-mm transparent, cone-tip trocar. A CO2 pneumoperitoneum to 15 mm Hg is established, and all visible peritoneal and visceral surfaces are inspected. Five additional 12-mm trocars are placed (Fig. 8.2).
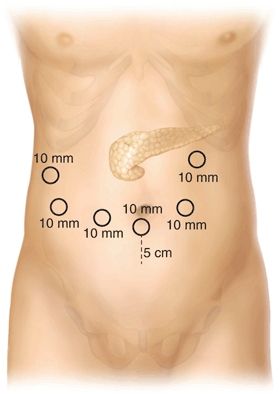
FIGURE 8.2 Trocar positioning for laparoscopic pancreaticoduodenectomy.
The gastrocolic ligament is divided with the harmonic scalpel (Ethicon Endosurgery, Cincinnati, OH), widely exposing the lesser sac. The gastroepiploic vessels are clipped and divided with the harmonic scalpel. The duodenocolic ligament is resected en bloc with the specimen to facilitate regional lymphadenectomy. A fan retractor is placed under the gastric antrum to provide exposure of the pancreatic head and neck.
Pancreatic Neck Dissection
The pancreatic neck is approached with the surgeon positioned on the left side of the patient. The common hepatic artery lymph nodes are removed, and the common and proper hepatic arteries are identified to verify tumor clearance. The portal vein is exposed at the cephalad border of the pancreatic neck and the superior mesenteric vein at the caudal border. The gastroduodenal artery is dissected, ligated, clipped, and divided. A plane between the posterior aspect of the pancreatic neck and the portal vein/superior mesenteric vein is developed. An articulating grasper is passed posteriorly and an umbilical tape is placed around the pancreatic neck and secured.
Duodenal Mobilization
The first portion of the duodenum is cleared, and the right gastric artery is ligated and divided. The duodenum is divided 2 cm distal to the pylorus using a linear stapler. The transverse colon is reflected cephalad, and the area of the ligament of Treitz is dissected mobilizing the third and fourth portions of the duodenum off of the aorta and inferior vena cava. The jejunum is divided 15 cm distal to the ligament of Treitz with the linear stapler, and the jejunal mesentery is then divided with the harmonic scalpel back to the uncinate process. The hepatic flexure of the colon is mobilized inferiorly, and the ascending and transverse colon are retracted inferiorly with a fan retractor. The surgeon moves to the patient’s right side, and the Kocherization of the duodenum is extended cephalad to the hepatic hilum.
Hepatic Hilar Dissection
A cholecystectomy is performed, leaving the cystic duct intact. The hilum of the liver is dissected, and the common hepatic duct is identified, ligated distally, and divided. All hilar lymphatic tissue is dissected inferiorly with the specimen. The lateral aspect of the portal vein is cleared caudally until the superior pancreaticoduodenal vein is identified, ligated, and divided. The jejunal stump is brought into the supramesocolic compartment, and the anterolateral aspect of the superior mesenteric vein is dissected proximally to the inferior border of the pancreas.
Pancreatic Head Resection
The pancreatic neck is divided with the harmonic scalpel, with the exception of the pancreatic duct, which is divided sharply with scissors. Using the umbilical tape for retraction, the pancreatic head and uncinate process are dissected off the portal vein, superior mesenteric vein, and superior mesenteric artery (SMA). The inferior pancreaticoduodenal artery and vein are ligated or clipped and divided with harmonic scalpel. Dissection of the uncinate is performed adjacent to the adventitia of the SMA to assure an appropriate oncologic margin.
Specimen Removal
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


