Epidural spinal cord compression (ESCC), resulting from tumor growth in the spinal epidural space, is an important neurological emergency that can occur in patients with breast cancer. The incidence may be increasing as a result of earlier detection and improved systemic therapy (1). Since the prognosis for good functional outcome is primarily dependent on the degree of impairment at the commencement of treatment, clinicians who care for patients with breast cancer must remain vigilant about the possible presence of ESCC. More than 91% of patients with ESCC have symptoms for longer than 1 week before a diagnosis is made (2), with pain lasting for a mean duration of 6 weeks (3). Compromise of the conus medullaris and cauda equina by epidural metastasis is generally included in a discussion of ESCC because the natural history and management of these problems are similar to those of compression of the spinal cord itself. ESCC is discussed in more detail in several recent reviews (1, 4, 5)
INCIDENCE
The incidence of ESCC in patients with breast cancer is approximately 4% (2). There are approximately 12,700 cases of ESCC in patients with cancer diagnosed each year in the United States (1, 6). The median time from the diagnosis of breast cancer to the onset of ESCC is 42 months, with a range of 0 to 28 years (2). ESCC usually occurs in the setting of widely metastatic disease, although rarely ESCC may be the initial presentation of cancer. In some instances, biopsy of an epidural metastasis is required to establish the diagnosis of cancer.
PATHOLOGY
Epidural metastases most commonly result from hematogenous spread of metastases to the vertebral column (85%). They arise less commonly from metastases to the paravertebral space (5% to 10%) that either secondarily invade bone and then grow into the epidural space or invade the epidural space directly through the intervertebral foramen (Fig. 77-1). In rare instances, direct hematogenous spread to the epidural space or parenchyma of the spinal cord occurs (1, 4), but this presentation is more likely with lymphoma than with breast cancer. If ESCC develops as the first manifestation of cancer, the absence of bony or skeletal metastases makes breast cancer an unlikely diagnosis. The vertebral column is the most common site of metastases to bone (7). Vertebral metastases occur in up to 84% in patients with advanced breast cancer (4). This high incidence is related to the fact that cancers of the breast and pelvis are in communication with Batson’s vertebral plexus (8, 9), a low-pressure valveless venous system that fills when thoracoabdominal pressure is raised (e.g., by maneuvers such as coughing, straining, and lifting). The presence of growth factors in bone marrow may also be a contributing factor (9). Of patients with breast cancer and ESCC, 93% have known bone metastases at the onset of their neurologic deficit, with a median time from the first bone metastasis to ESCC of 11 months (range, 0 to 7.5 years). Breast cancer is commonly associated with multilevel vertebral metastases, and epidural tumor is multifocal in up to 29% of patients (10). As would be anticipated from their origin in the vertebral bodies, most epidural metastases are situated anterior or anterolateral to the spinal cord (1, 5), which has important implications for their surgical management. Sixty or 70 percent of epidural metastases arise in the thoracic spine, 16% to 22% in the lumbosacral spine, and 8% to 15% in the cervical spine (11). These figures are proportional to the volume of bone in each of these spinal regions (12).
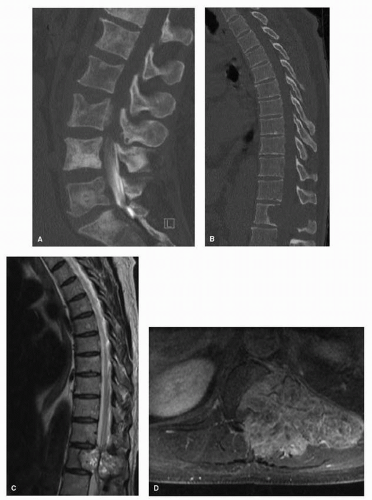
FIGURE 77-1(A) Sagittal postmyelogram CT demonstrating a complete block due to epidural compression from a breast metastasis. The block, located at the L3/4 disc space demonstrates the lower extent of the mass. This was predominantly an epidural mass which occurs in a small minority of cases. (B) Sagittal CT scan demonstrating lytic destruction of the T12 vertebral body due to a breast metastasis. Despite the extensive destruction there is no collapse of the vertebral body or kyphosis of the spinal canal. Destruction of the posterior elements is also seen. (C) T2-weighted sagittal MRI demonstrating the T12 breast metastasis and the severe spinal cord compression. The spinal fluid appears white on this sequence. The tapering of the spinal fluid on the sagittal image in the region of the mass is characteristic of compression from an extradural mass. (D) T2-weighted axial MRI demonstrating the T12 breast metastasis and the severe spinal cord compression. The axial image demonstrates significant paraspinal extension as well.
Spinal cord damage in ESCC is due primarily to direct compression of the spinal cord by tumor and rarely to compression of radicular arteries that pass through the intervertebral foramen (4). Axonal swelling and white matter edema occur early in animal models of ESCC, whereas gray matter damage occur later (13). Prolonged cord compression results in necrosis of both gray and white matter. Early spinal cord damage is likely caused by venous stasis, whereas arteriolar compression by tumor is probably responsible for the late stage of tissue necrosis (13).
CLINICAL PRESENTATION
ESCC due to breast cancer occurs most commonly in the thoracic spine (9, 10, 25). The principal symptom of ESCC is pain (14) (Table 77-1). It is the initial symptom in 85% to 96% of patients and precedes other symptoms by a mean of 6 weeks (2, 15). Pain is of three types: local, radicular, and referred. Local back pain is usually a constant ache and occurs in almost all patients. Radicular pain is caused by involvement of nerve roots by the tumor mass and is typically described as a shooting pain. It is more common with cervical and lumbosacral lesions than with thoracic lesions (16). With cervical or lumbosacral epidural metastases, radicular pain is typically unilateral. With thoracic disease, however, radicular pain is commonly bilateral, producing a band-like pain or tightness that may be felt more at the lateral or anterior chest wall than in the back itself. Referred pain occurs at a distant site from the lesion and does not radiate. For example, T12-L1 vertebral lesions may be referred to both iliac crests or both sacroiliac joints, whereas C7-T1 lesions may be referred to the interscapular region or to both shoulders (17). The pain of epidural metastasis is often worsened by lying supine, possibly because of filling of vertebral veins in this position. Patients typically report that they are unable to sleep lying down and need to sleep sitting up; this information is often not volunteered by patients but must be sought by direct questioning. The pain tends to be most prominent at night and into the morning, with resolution or improvement over the course of the day (18). The Valsalva maneuver (coughing, sneezing, or straining at stool) exacerbates the pain of epidural metastases, as it fills vertebral veins and raises intracranial pressure, which is then transmitted to the already compromised spinal canal. Pain is also worsened by stretching maneuvers, such as neck flexion in the case of cervical or upper thoracic tumors and straight-leg raising with lumbosacral or thoracic lesions. Escalating back pain in patients with cancer is a particularly ominous indicator of the possibility of ESCC. Tenderness may be present over the vertebral column at the site of the lesion, and there may be referred tenderness at the site of referred or radicular pain. Pain that worsens substantially with movement of the neck or back may be a sign of mechanical instability of the spinal column, which can occur in the setting of vertebral or epidural metastases (18).
TABLE 77-1 Symptoms Associated with Epidural Spinal Cord Compression
Symptom
Frequency
Location
Back pain
95%
• Localized pain confined to the area with the metastases that progressively increases over time.
• Radicular pain due to invasion of the nerve roots, unilateral in the cervical and lumbosacral areas, bilateral in the thoracic region. Pain is worse with Valsalva and at night.
• Mechanical back pain due to pathological fractures, pain is exacerbated by any movement.
Weakness
35%-75%
• Upper motor neuron weakness—symmetric.
• Lower motor neuron weakness predominantly distal extremities affected and can be unilateral.
Inability to walk
50%-68%
• Tied in with weakness but can also be linked with ataxia due to sensory problems.
Sensory deficits
50%-70%
• Pain, numbness, ataxia.
Autonomic disturbance
50%-60%
• Bowel or bladder disturbance.
• High cervical cord metastases can cause respiratory problems.
Adapted from the data reviewed in Cole JS, Patchell RA. Metastatic epidural spinal cord compression. Lancet Neurol 2008;7(5):459-466, describing the frequency of symptoms associated with ESCC.
The spinal cord usually ends at the level of L1. Therefore, ESCC above L1 will produce a myelopathy, whereas lesions below this level result in a cauda equina syndrome. Myelopathic symptoms include limb weakness in a pyramidal distribution, numbness and paresthesia, and sphincter disturbance (urinary retention, urinary urgency, constipation, or fecal urgency). At the time of diagnosis, 76% of patients complain of weakness, 87% are weak on examination, 57% have autonomic dysfunction, 51% have sensory symptoms, and 78% have sensory deficits on examination (16). In many series, fewer than 50% of patients are ambulatory at diagnosis, and up to 25% are paraplegic (2, 3, 16); these figures are significant because prognosis is related to clinical deficit at presentation. Outcomes might be improved if patients were encouraged to seek treatment earlier.
Signs of a myelopathy include paraparesis or quadriparesis, increased tone, clonus, hyperreflexia, extensor-plantar responses, a distended bladder, or a sensory level. A patch of hyperesthesia may be present at the upper aspect of the sensory level. The sensory, motor, and reflex levels are only an approximate indication of the site of pathology; because sensory fibers retain their somatotopic organization as they ascend in the cord, the actual site of cord compression may be several segments above the apparent sensory level. Furthermore, there may be multiple sites of epidural disease. The entire spinal cord should, therefore, be imaged in all patients with myelopathy.
The myelopathy may be incomplete, and it is a serious error to dismiss the possibility of ESCC on the basis that any particular sign is absent. Neither a sensory level nor an extensor plantar response is necessary to make the clinical diagnosis of ESCC. Dorsal column sensation (vibration and proprioception) and spinothalamic sensation (pain and temperature) must be assessed independently in all patients with cancer and back pain. Because the subjective appreciation of light touch involves both sensory pathways, lighttouch sensation may be reasonably well preserved, even in the presence of a clear cut sensory level for pain or vibration sense when these are tested separately. A hemicord or Brown-Séquard’s syndrome (characterized by ipsilateral weakness and proprioception loss, and contralateral loss of pain and temperature) may occur, although this is rare in ESCC (10, 16). In an oncologic population, Brown-Séquard’s syndrome is more typical of intramedullary cord metastasis or radiation myelopathy (19). Involvement of spinocerebellar tracts in the spinal cord can lead to lower extremity ataxia out of proportion to the degree of weakness. Dorsal column involvement can lead to a sensory ataxia with positive rombergism while sparing power and reflexes. Both of these clinical presentations may focus the attention of the unwary examiner on the cerebellum, thereby delaying diagnosis (20). Patients may also present with herpes zoster, presumably as a result of reactivation of latent virus by compression of the dorsal root ganglion by tumor (16).
ESCC at the conus medullaris and cauda equina produces different neurologic symptoms and signs, although pain is still a prominent feature, particularly with cauda equina lesions. Conus lesions typically present with early and marked sphincter disturbance and perineal sensory loss. Anal sphincter tone may be lax, and there may be an absent anal wink. Cauda equina lesions produce patchy lower motor neuron signs related to the lumbar and sacral nerve roots—hyporeflexia or areflexia, myotomal leg weakness, and dermatomal sensory loss; sphincter disturbance tends to occur late and to be less marked than in conus lesions. When the signs include a mixture of upper and lower motor neuron features or dermatomal sensory loss as well as a sensory level, the possibility of coexistent nerve root involvement and cord compression should be considered.
INVESTIGATIONS
Epidural spinal cord compression is a medical emergency requiring expeditious investigation of all patients in whom this diagnosis is suspected. Magnetic resonance imaging (MRI) is the test of choice, although rarely other modalities may be useful.
Plain X-Rays: From 94% to 98% of patients with epidural disease will have visible vertebral metastases on plain spine films (10, 21, 22, 23). However, these are now rarely performed given the widespread availability of MRI.
Radionuclide Bone Scan: Bone scintigraphy is more sensitive than plain radiography in the detection of epidural metastasis (24). Spinal metastases as small as 2 mm can be detected and will pick up bone metastasis 3 to 18 months before x-rays. However, it is poor in delineating the anatomy, and in cancers causing osteolytic lesions, it is less useful (23).
Positron Emission Tomography (PET)/CT: PET/CT is used to stage cancer, and is largely more sensitive and specific in detecting metastases relative to a bone scan (25).
Computed Tomographic (CT) Scanning: CT remains one of the best techniques in assessing the anatomy of the actual vertebral body prior to surgical stabilization (Fig. 77-1A, B). Its sensitivity is limited to about 66% and diagnostic accuracy to approximately 89% in detecting areas of vertebral destruction, assessment of extent of paravertebral soft-tissue extension and impingement of the actual spinal cord (26). If there is a contraindication to use MRI (pacemaker, noncompatible MR implants), CT myelography may still be employed to delineate the level of the block (27) (Fig. 77-1A).
Magnetic Resonance Imaging (MRI): Contrasted MRI is the gold standard investigation in detecting ESCC. MRI has a sensitivity of 98.5% and a specificity 98.9% with an overall accuracy of 98.7% (26) (Fig. 77-1C, D). If ESCC is suspected, the entire spine should be imaged since multifocal disease occurs frequently (28). MRI influences radiotherapy fields and in one study led to simulation alterations in 53% of patients, with 21% being major changes (28).
An unenhanced MRI scan can establish the diagnosis of ESCC. However, a contrast-enhanced scan should also be obtained to look for leptomeningeal metastasis, which may mimic the presentation of ESCC. The entire spine should be imaged, as epidural disease may be present at multiple levels, and the spinal level indicated by clinical examination may be several segments below the level of the lesion (29). It is important to obtain axial scans in addition to sagittal images. A “screening” midline sagittal scan is inadequate; multiple sagittal scans using thin slices should be performed. Coronal images of the spine are not required routinely. Adequate analgesia (including corticosteroids) should be administered before the MRI is performed because the patient must lie motionless for the scan, and lying flat may worsen the back pain. If the patient cannot tolerate the full procedure, or if there is not enough time to perform an MRI of the entire spine, the area of interest should be imaged first, followed at a later time by imaging of the remainder of the spine. When ordering radiologic investigations, a clear distinction should be made between the suspected neurologic level of involvement and the suspected vertebral level; the discrepancy between these is greatest at the inferior end of the spinal cord. Because the spinal cord terminates at the first lumbar vertebra, all of the lumbar segments and some of the sacral segments of the cord are usually situated within the thoracic spine.
EVALUATION OF INDIVIDUAL CONDITIONS
Isolated Back Pain
In patients with breast cancer and isolated back pain without neurologic abnormalities, plain spine radiographs are occasionally the appropriate first line of investigation. Definitive imaging of the epidural space should be performed if plain films are abnormal. In patients with a clinical picture that is strongly suggestive of epidural metastasis (e.g., back pain that is significantly exacerbated by lying flat and worsened by the Valsalva maneuver), MRI of the spine with contrast should be performed. In patients with local back pain with characteristics that are not strongly suggestive of epidural metastasis, definitive imaging of the epidural space is not indicated if a plain radiograph is normal.
Radiculopathy
Radiculopathy is associated with a high incidence of epidural metastases. In one series of patients with cancer and back pain, 27 of 43 (63%) patients with radiculopathy and without signs of spinal cord involvement were found to have epidural metastases, compared with 27 of 61 (44%) patients with local back pain alone (27). When plain radiographs were abnormal, epidural metastases were found in 20 of 22 (91%) patients with radiculopathy. Similarly, in patients with abnormal findings on plain radiographs, Graus et al. found epidural metastases in 47 of 67 (70%) patients with radiculopathy, compared with 12 of 35 (34%) patients with local back pain alone (30). Importantly, in the series by Graus et al. (30) and Rodichok et al. (27), epidural metastases were found in 9% to 33% of patients with radiculopathy and normal findings on plain radiographs.
Given the high incidence of epidural metastases in breast cancer patients with radiculopathy, it is reasonable to proceed straight to MRI in all patients. It is important to remember that in the thoracic spine, which is the most common site of ESCC in breast cancer, radiculopathy commonly presents as bilateral, band-like dermatomal pain and that, in some situations, lateral or even anterior chest pain may be more prominent than back pain.
Plexopathy
The possibility of epidural metastasis must be considered in patients with breast cancer and a malignant brachial plexopathy because tumor may infiltrate directly along the plexus to the epidural space. Brachial plexus lesions present with pain (usually in the shoulder girdle with radiation to the elbow, medial side of the forearm, and medial two digits) as well as weakness and sensory symptoms in a segmental distribution. Clinical clues to the presence of epidural metastases in the setting of brachial plexopathy include a panplexopathy (as compared to the more usual lower plexopathy with involvement of C7, C8, and T1 nerve roots) and the presence of Horner’s syndrome (indicating more proximal involvement). The presence of back pain also suggests that the tumor has grown proximally, but back pain may be absent with epidural extension. Patients with brachial plexopathy require imaging of the brachial plexus with CT or MRI and, if vertebral body collapse or erosion is present, at the C7-T1 levels. If a paraspinal mass is seen definitive imaging of the epidural space should be performed. If MRI is used to image the brachial plexus, the cervical and upper thoracic spine can be imaged at the same time.
Only gold members can continue reading. Log In or Register to continue
 Breast Cancer Screening
Breast Cancer Screening
 Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
 Postmastectomy Radiation Therapy
Postmastectomy Radiation Therapy
 Preoperative Chemotherapy for Operable Breast Cancer
Preoperative Chemotherapy for Operable Breast Cancer
 Palliative Care in Breast Cancer
Palliative Care in Breast Cancer
 Nursing Care in Patient Management and Quality of Life
Nursing Care in Patient Management and Quality of Life



