Thus, long-term follow-up for breast cancer patients at risk of LRR is warranted.
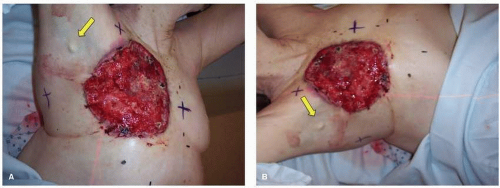 FIGURE 69-1 (A) and (B) An advanced CWR in a patient who was not a candidate for surgical resection due to her elderly age and poor performance status. The CWR was ulcerated at presentation and continued to grow despite chemotherapy. Only superficial debridement was performed. Note the arrow highlighting the large, fixed palpable lymph node in the axilla. |
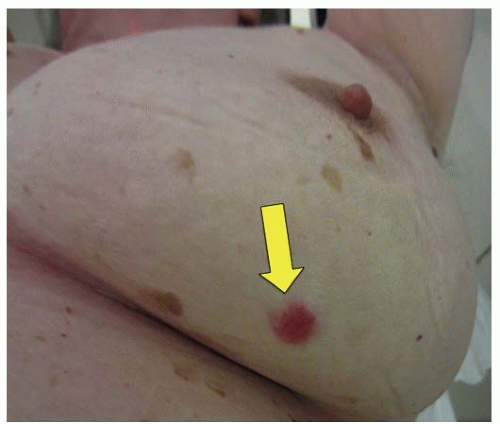 FIGURE 69-2 Ipsilateral breast tumor recurrence in a patient previously treated with breast conservation. Despite the patient’s other skin lesions, the index of suspicion remained high, and a biopsy confirmed a local recurrence in the previously treated breast. The tumor recurrence was located in a separate quadrant remote from the primary tumor. |
as the primary tumor (11). Detection of IBTR by mammography alone can be challenging due to post-operative and post-radiation scar tissue development, but detection of IBTR is higher when recurrent tumors are associated with calcifications.
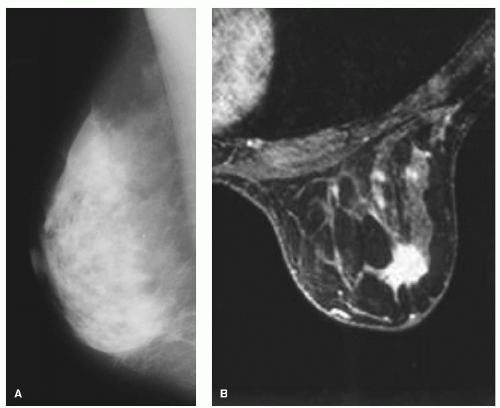 FIGURE 69-3 Imaging of an ipsilateral breast tumor recurrence in a patient previously treated with breast conserving surgery and radiation. Given the density of the breast and scar tissue, mammogram was unable to detect recurrence. MRI was more sensitive in discerning density and scar tissue from tumor. |
delivered twice daily over 1 week) as a faster alternative to conventionally fractionated whole breast radiation. While the existing data on definitive partial breast irradiation cohesively suggest excellent local-regional control comparable to that of whole breast radiation, prospective data with longterm outcomes and safety are lacking (14). Irrespectively, given the limited tolerance of normal tissue after these definitive doses of radiation to the breast, IBTRs occurring in previously radiated BCT patients are often treated with mastectomy, which is generally felt to be the standard management approach. For patients who have not been treated with radiation therapy as a component of their initial treatment, a repeat breast conservation procedure with excision of the recurrence followed by a course of radiation therapy can be considered. It remains uncertain whether mastectomy after IBTR improves outcomes compared with lesser surgery. A number of studies comparing mastectomy and breast conservation as treatment for IBTR are detailed in Table 69-1. Together, these studies suggest that the rates of recurrence are greater after a second local excision compared with mastectomy, but whether this ultimately translates to improved survival outcomes remains unclear (15).
TABLE 69-1 Surgical Treatment of IBTR | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
local excision followed by partial breast irradiation utilizing 3D-conformal external beam radiation techniques to deliver 45 Gy in 1.5 Gy fractions bid. The primary endpoint being evaluated is adverse effects after re-irradiation, with secondary endpoints including in-breast recurrence rates, mastectomy-free survival, overall survival, monitoring/correlating circulating tumor cells with relapse, and cosmesis (Fig. 69-4).
TABLE 69-2 Results of Re-irradiation Using a Partial Breast Technique after Repeat Breast Conservation for Local Relapse | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:
 Breast Cancer Screening
Breast Cancer Screening
 Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
 Postmastectomy Radiation Therapy
Postmastectomy Radiation Therapy
 Preoperative Chemotherapy for Operable Breast Cancer
Preoperative Chemotherapy for Operable Breast Cancer
 Management Summary for the Care of Patients with Metastatic Breast Cancer
Nursing Care in Patient Management and Quality of Life
Management Summary for the Care of Patients with Metastatic Breast Cancer
Nursing Care in Patient Management and Quality of Life
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


