TABLE 12A.1 SUMMARY OF MAJOR PROSPECTIVE TRIALS USING HORMONAL THERAPY AND RADIOTHERAPY | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||
significant difference in overall survival (p = 0.02) and PFS (p = 0.005) in favor of the combined arm; this difference was mainly caused by lymph node positive tumors. In conclusion, patients with pathologically or clinically involved pelvic lymph nodes should be considered for RT plus immediate long-term HT.
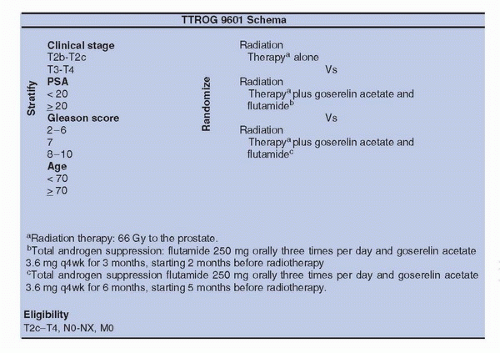 FIGURE 12A.1. Treatment schema for the Trans-Tasman Radiation Oncology Group and TTROG 96.01 randomized prospective Trial of radiation therapy and adjuvant hormonal therapy. (PSA, prostate specific antigen). |
alone was not assessed so far (Fig. 12A.2). The SPCG-7/SFUO-3 trial has included 875 patients with T1b-2, G2-3, or T3 of any WHO histological grade (1,2,3) (78% of T3) with baseline PSA < 70 ng/mL; patients were randomly allocated to endocrine treatment alone (3 months of total androgen blockade followed by continuous treatment using flutamide [439 patients]) or to the same endocrine treatment combined with RT (436 patients). After a median follow-up of 7.6 years, the cumulative incidence at 10 years for prostate cancer-specific mortality was 23.9% in the endocrine alone group and 11.9% in the endocrine plus RT group for a relative risk of 0.44 (0.30-0.66); the cumulative incidence for overall mortality was 39.4% and 29.6% with a relative risk of 0.68 (0.52-0.89) (26). In conclusion, in patients with locally advanced or high-risk localized prostate cancer, the combination of RT to HT halved the 10-year prostate cancer-specific mortality and decreased overall mortality with fully acceptable risk of side effects, compared to HT alone.
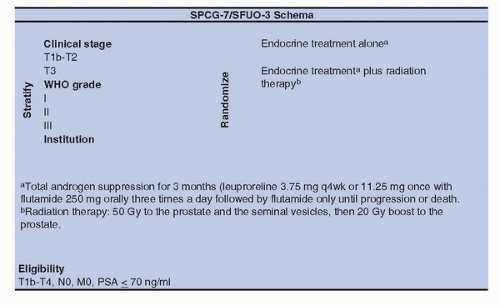 FIGURE 12A.2. Treatment schema for the Scandinavian Prostate Cancer Group Study and the Swedish Association for Urological Oncology and SPCG-7/SFUO-3 randomized prospective trial of radiation therapy and adjuvant hormonal therapy. (PSA, prostate specific antigen). |
done with PSA (lower than 20 ng/mL), histological grade, and nodal status. Patients were randomized between neodjuvant CAB, 2 months before conventional irradiation and 2 months during irradiation (66.6 Gy) versus irradiation alone. The 10-year overall survival was 62% for the combined approach versus 57% (p = 0.03). In conclusion, the addition of neoadjuvant and concomitant CAB—4 to 6 months—with irradiation (66.6-70 Gy) improved overall survival in men with intermediate-or poor-risk localized prostate cancer without moderate or severe comorbidity.
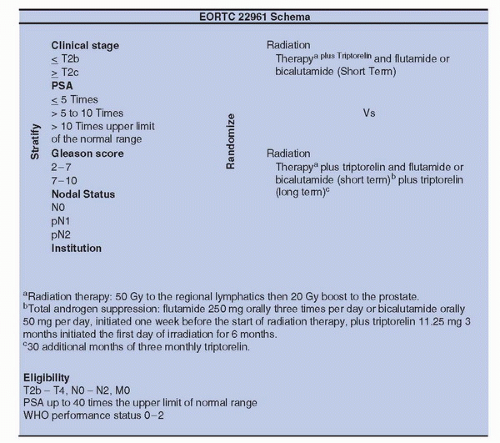 FIGURE 12A.3. Treatment schema for the European Organization for Research and Treatment of Cancer (EORTC) and EORTC 22961 randomized prospective trial of radiation therapy and adjuvant hormonal therapy. (PSA, prostate specific antigen). |
CAS. The hazard ratio (HR) for freedom from PSA failure was 0.67 (95% CI 0.53-0.85; p = 0.0007) for the dose escalated group and the 5-year control rate was 71% for the high dose compared to 60% for conventional dose group. Of note, there was also a trend for improved freedom from salvage AS, HR of 0.78 (0.57-1.07; p = 0.12); and metastases-free survival was 0.74 (0.47-1.18; p = 0.21) (41). We are eager to wait the results of EORTC trial 22991, which has accrued 820 patients, comparing 3D-CRT +/− IMRT alone with three levels of dose (70, 74, 78 Gy) versus the same regimen plus 6 months AS. In intermediate-risk localized prostate cancer, there is likely a room for dose escalation alone, provided the dose is ≥78Gy. The results of RTOG trial 94-08 in good and intermediaterisk localized prostate cancer have shown an improvement of 10-year overall survival (33) with 66.6 Gy plus 4 months of CAB, but we do not have data concerning a trial with a dose escalation RT alone arm.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


