(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
Internal hemipelvectomy involves the removal of the innominate bone, with adjacent muscles if involved, with preservation of the ipsilateral lower extremity. It is performed for malignant tumors arising in the innominate bone or involving it by direct extension. Obviously, the tumors requiring internal hemipelvectomy are less extensive than tumors in this area that require external hemipelvectomy.
The patient is placed in a lateral or semilateral position. The lower extremity is covered with a sterile stockinette up to the proximal thigh. The lower abdomen and buttock are prepped and draped in the field. The incision is determined by the boundaries of this operation: the sacroiliac joint posteriorly, the pubic symphysis anteriorly, and the greater trochanter laterally. It assumes the shape of a reverse Y (Fig. 43.1), the long limb being the iliac crest. The incision is started from the posterior superior iliac spine and is carried to the anterior superior iliac spine. From this point, it is continued medially along the inguinal ligament to the pubic symphysis, and laterally to the greater trochanter and below it for about 5 cm. The incision should be modified to include a previous biopsy site if one is present. The fascia is exposed, and initially the fascia of the external oblique aponeurosis is divided posteriorly along the iliac crest, as well as the internal oblique and transversus abdominis muscles (Fig. 43.2), allowing entry into the retroperitoneal space (Fig. 43.3). The inguinal ligament is divided off the anterior superior iliac spine, and then the lateral third of the inguinal ligament is separated from the iliac fascia. Below the inguinal ligament, the femoral artery and vein are exposed. As the lateral third of the inguinal ligament is separated from the iliac fascia, the inferior epigastric artery and then the inferior epigastric vein are exposed (Fig. 43.4), ligated, and divided. The deep iliac circumflex artery and vein (which are enclosed in a sheath formed by the iliac and transversalis fascia on their way toward the anterior superior iliac spine) are ligated and divided lateral to the iliofemoral vessels. The reason for their ligation is that the iliofemoral vessels should be completely free, so they can be retracted to provide exposure of the origin of the adductors and rectus femoris, which must be divided. Often a small tributary to the external iliac vein, the pubic vein, is found coming from the wall of the lesser pelvis and also needs to be ligated and divided once the exposure is provided. The inguinal ligament is divided again at the pubic tubercle so that the entire length of the inguinal ligament is freed from its origin to its insertion, remaining in contact with the anterolateral abdominal wall muscles. Medially, the incision continues above the pubic crest to divide the anterior rectus sheath and then the rectus abdominis muscle. The retroperitoneal space is entered posterolaterally and the peritoneum is displaced off the surface of the external iliac vessels. After the inferior epigastric vessels are ligated and divided and the rectus abdominis muscle and its anterior sheath are divided off the pubic crest, the exposure of the retroperitoneal space is greatly improved (Fig. 43.5). The superior aspect of the pubic symphysis is exposed. With further dissection, staying on the surface of the bone, the inferior aspect of the pubic symphysis is dissected and the pubic symphysis is now exposed both superior and inferior to the pubic arch. A right angle clamp is passed around it, and then a Gigli saw, which helps divide the pubic symphysis (Fig. 43.5). The iliac fascia is incised longitudinally lateral to the point at which the external iliac artery becomes the common femoral artery. The femoral nerve, usually covered with a small amount of adipose tissue, is identified and traced proximally as it dips between the fibers of the iliacus and psoas muscles to well above the level of the sacroiliac joint.
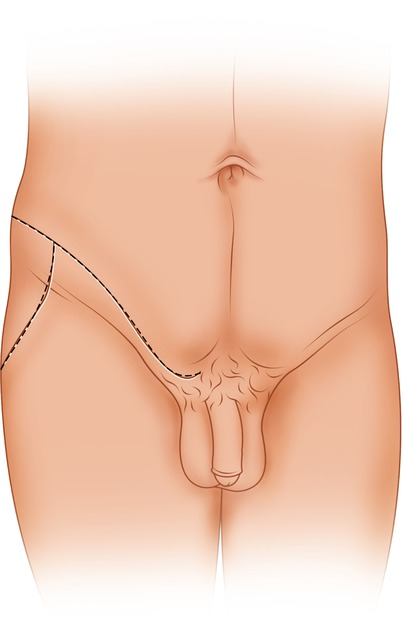
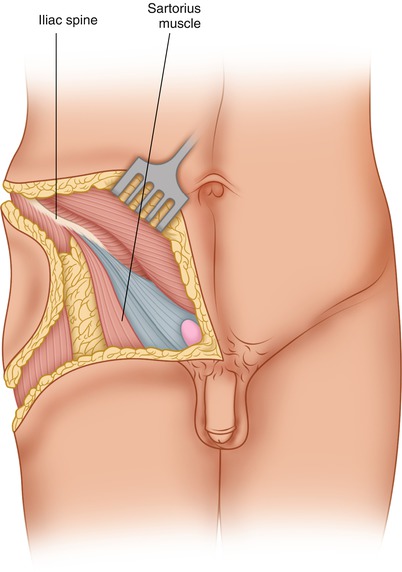
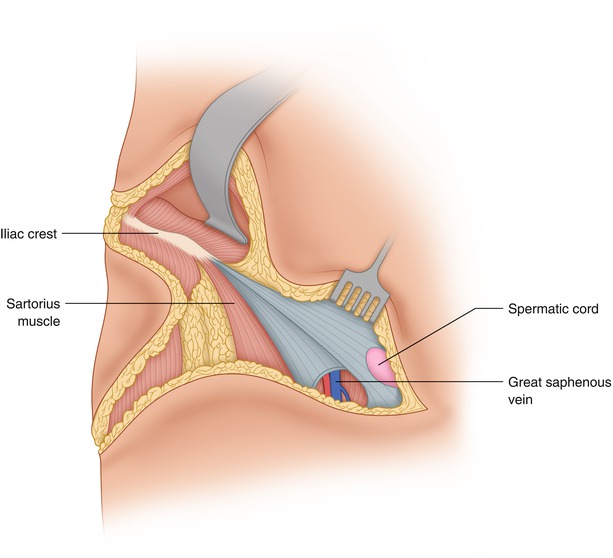
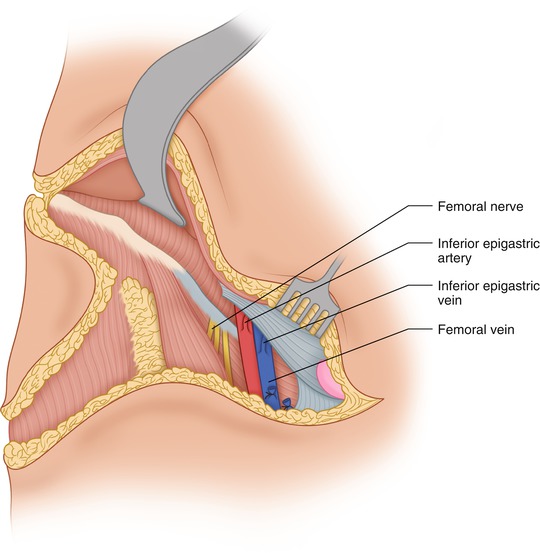
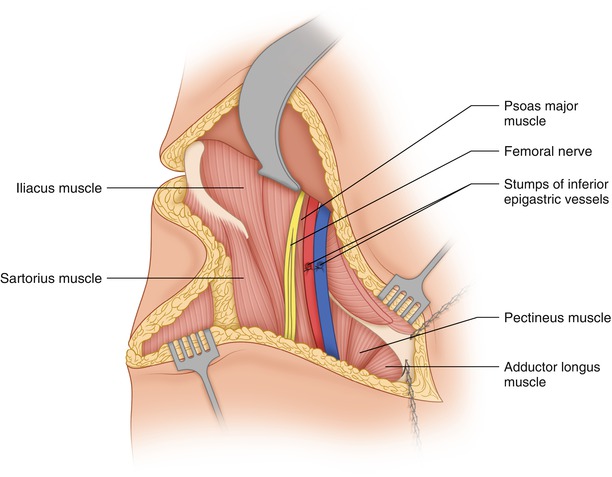
Fig. 43.1
A reverse Y incision is used
Fig. 43.2
The incision is carried to the level of the fascia
Fig. 43.3
The retroperitoneal space is entered above the iliac crest
Fig. 43.4
The inferior epigastric vessels are exposed and dissected so they can be ligated and divided. The femoral nerve has been exposed lateral to the common femoral artery
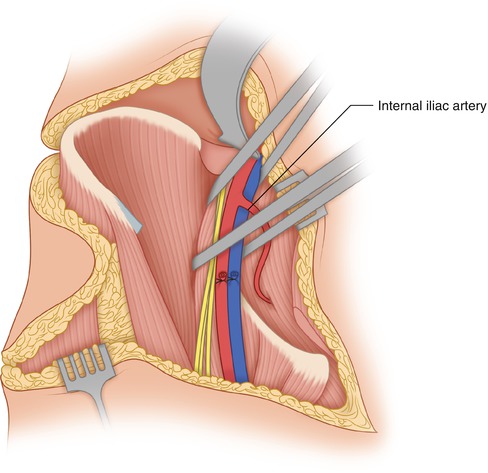
Fig. 43.5
The pubic symphysis is divided with a Gigli saw. The retroperitoneal space has been exposed after ligation and division of the inferior epigastric vessels and after division of the rectus abdominis muscle off the pubic crest
The femoral nerve, surrounded by tapes so that it can be retracted as necessary, provides a good landmark for the plane of separation between the fibers of the psoas muscle and those of the iliacus. The muscle fibers of the psoas may be surrounded by a tape passed from the lateral side of this muscle on the surface of the iliac bone to the greater sciatic notch. The tape is made to encircle the psoas, the femoral nerve, and the iliofemoral vessels (Fig. 43.6). The iliacus muscle, originating from the iliac bone and clinging to its medial aspect, is removed en bloc with the bone. The inguinal and iliac nodes should be removed only if indicated by tumor biology, nor should the iliofemoral vessels be skeletonized by entering their sheaths, as this will interrupt some lymphatics and likely increase the chance of postoperative lymphedema of the extremity. If any nodes appear to be enlarged and suspicious, they may be removed and subjected to frozen section. Hyperplastic nodes, even when large, retain their soft consistency and are rather flat, whereas lymph nodes involved by malignant tumor are more spherical and firm. The iliofemoral vessels are sufficiently mobilized so they can be retracted, and the muscles originating from the inferior aspect of the pubic and ischial bones are divided at their origin. The adductor muscles (the pectineus, adductor longus, and gracilis), the second layer of adductors (the adductor brevis), and finally, the adductor magnus are divided off the anterior and posterior pubic rami (Fig. 43.7). The obturator nerve (anterior and posterior divisions) and vessels are encountered in front of and behind the adductor brevis, and they are ligated and divided. An indication that one has divided the adductors at their origin is that the obturator externus muscle is then exposed, covering the obturator foramen on its inferior aspect. (The superior aspect is covered by the obturator internus.)