(1)
State University of New York at Buffalo Kaleida Health, Buffalo, NY, USA
Forequarter amputation, also called interscapulothoracic amputation, involves the removal of the whole upper extremity, the scapula, and a portion of the clavicle. It is performed for malignant tumors near the shoulder or axilla, or those involving extensively the brachial plexus, axillary vessels, or both. Involvement of the axillary vein itself is not an indication for amputation, because this vessel (or at least its lateral two thirds) can be sacrificed without replacement, as sufficient venous outflow is provided by the cephalic and other veins, so that venous edema is usually avoided. Forequarter amputation generally is performed for any tumor in this area that cannot be removed with a lesser operation.
The Anterior Approach to Vessel Control
An incision from a point near the sternal end of the clavicle is carried obliquely to the medial wall of the axilla. From the same starting point, another incision is carried above and along the clavicle to near the acromion, from where it is directed on the posterior aspect of the shoulder and along the axillary border of the scapula to its inferior angle. This incision then changes direction to meet the anterior incision in the medial wall of the axilla (Fig. 17.1). Of course the incision should be modified according to the location of the tumor, to allow wide margins all around it. The anterior part of the incision is carried through the subcutaneous fat and deepened through the fibers of the clavicular origin of the pectoralis major, which are divided below the clavicle to the anterior axillary fold. Dissection above the clavicle is carried out, dividing the platysma fibers and exposing the superior surface of this bone. The clavicular head of the sternocleidomastoid medially may be divided (Fig. 17.2). It then becomes possible to manipulate the end of a right angle clamp around the clavicle near its sternal end, which is simpler than disarticulating the sternoclavicular joint. With a Gigli saw, the clavicle is divided near its medial end (Fig. 17.3). The lateral end of the divided clavicle is held with a bone clamp, and with further dissection, the posterior surface of the clavicle is freed lateralward for 4–5 cm and is divided again at this point. The removal of a piece of the clavicle provides the necessary room for the exposure of the subclavian vessels as they arch over the first rib (Fig. 17.4). The subclavius muscle, which is superficial to the subclavian vessels and extends from the cartilage of the first rib to the inferior surface of the clavicle laterally, is divided. A skin flap underneath the platysma is raised superiorly to about the mid portion of the sternocleidomastoid muscle. The fascia on the surface of the sternocleidomastoid is incised, exposing its lateral edge. The omohyoid is divided where it crosses behind the sternocleidomastoid. The sternocleidomastoid is retracted and the internal jugular vein is exposed. The fat pad and nodes are dissected en bloc from the surface of the scalenus anterior and are moved in a lateral direction in order to be removed with the specimen. This exposes the scalenus anterior muscle and the phrenic nerve running on its anterior surface. Lateral to the edge of the scalenus anterior, the trunks of the brachial plexus are exposed; the fat and lymph nodes are mobilized off the plexus in a lateral and posterior direction.
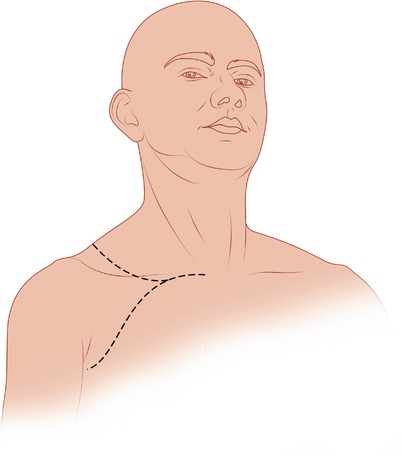
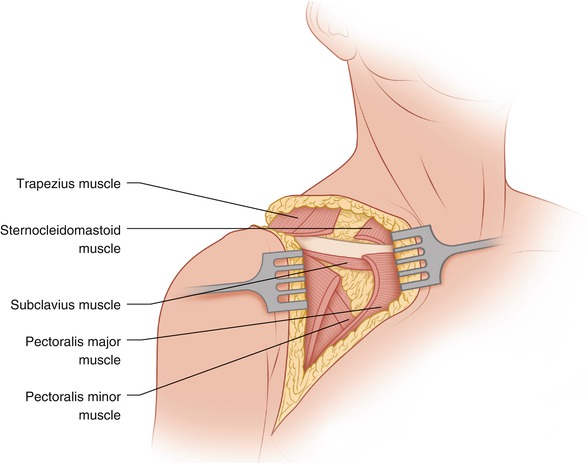
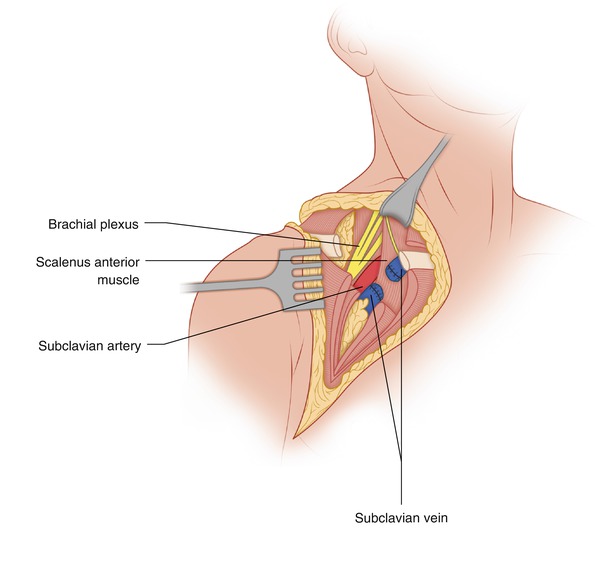
Fig. 17.1
The anterior portion of the incision is shown. Posteriorly, the incision is carried over the lower neck and along and slightly medial to the axillary border of the scapula to the inferior angle of the scapula, meeting the anterior incision in the medial wall of the axilla
Fig. 17.2
The platysma has been divided above the clavicle, and the pectoralis major has been divided below it
Fig. 17.3
The clavicle is divided near the sternal end, following division of the clavicular head of the sternocleidomastoid
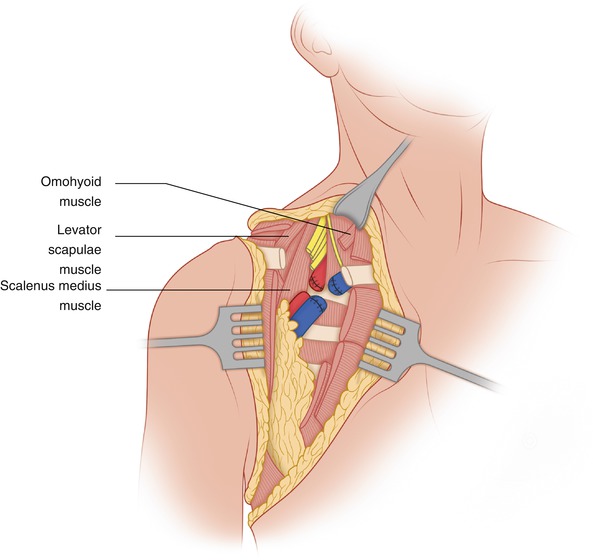
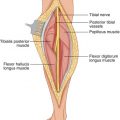
Fig. 17.4
A portion of the clavicle and subclavius muscle have been removed. The subclavian vein has been divided and the two stumps oversewn. The subclavian artery and brachial plexus are visible, as well as the scalenus anterior muscle and the phrenic nerve coursing on its surface
The scalenus anterior muscle, inserting at the first rib, is a good anatomic landmark separating the subclavian vein, which courses in front of this muscle, from the subclavian artery, which runs behind this muscle, as both vessels arch over the first rib. By following the lower part of the internal jugular vein in a lateral direction, the subclavian vein is exposed and a vessel loop is passed around it. The subclavian vein is divided between vascular clamps and the stumps are oversewn with a vascular suture while a stout ligature is placed proximal to the suture-closure of the opening (Fig. 17.4). Before clamping and dividing the vein, it is preferable that a ligature be placed on the artery to avoid the loss of some blood within the extremity. The same procedure is repeated with the subclavian artery, which is clearly exposed after division of the subclavian vein. The subclavian artery is exposed more proximally in order to allow secure ligation both proximally and distally, which is supplemented with suture ligature at least on the proximal side (Fig. 17.5). Care should be exercised in ligating the artery, because the intima of the vessel at times may disrupt owing to atherosclerosis, weakening the security of the knot and resulting in bleeding. Therefore, a small segment of the vessel should be kept available proximally so that there is enough space to apply a vascular clamp in such an eventuality.