Resection of the Primary Tumor to Negative Margins
Lymph Node Dissection
Gastrointestinal Reconstruction
Construction of Gastric Conduit
Performance of a Gastric-Emptying Procedure
Alternate Conduits
Cervical Versus Intrathoracic Anastomosis
Hand-Sewn Versus Stapled Anastomosis
End-to-End Versus End-to-Side Anastomosis
a negative margin with the ability to complete the operation safely and to reestablish GI continuity. In this regard, intraoperative pathologic evaluation of the proximal margin should be considered unless resection of additional proximal esophagus would be ill-advised.
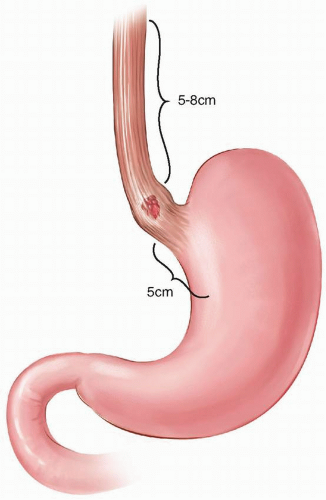 FIGURE 7-1 A proximal distance of 5 to 8 cm and distal length of 5 cm from the respective tumor edge maximizes likelihood of a microscopically negative margin. |
to consistently demonstrate 5-year survival rates between 25% and 30%.25,26,27 These series mostly involve two-field (thoracic and abdominal) lymph node dissections or sampling through either a transhiatal or transthoracic approach. Altorki et al28 demonstrated that a three-field approach with associated three-field lymph node dissection (cervical, thoracic, and abdominal) can be safely performed with low mortality and 5-year survival rates approaching 50%. These outstanding results have not been replicated in other centers, limiting the applicability of these data.
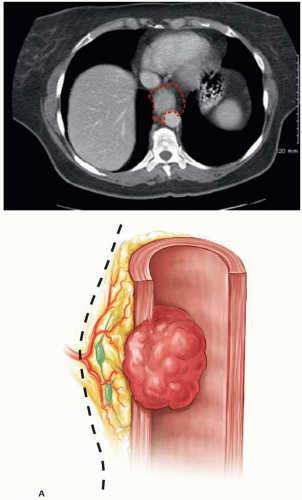 FIGURE 7-2 Circumferential dissection plane of the esophagus during esophagectomy for malignancy. A: Axial view of computed tomography scan (top) and illustration (bottom) show tumor in the esophagus and the suggested resection plane (black dotted line) to facilitate negative radial margin. |
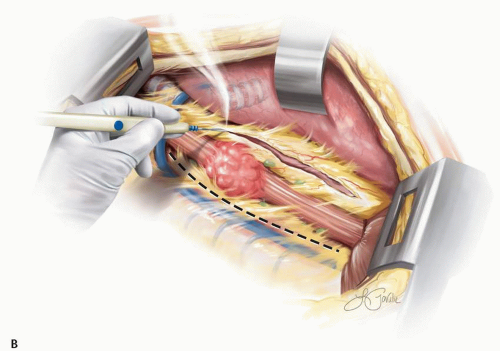 FIGURE 7-2 (continued) B: Illustration shows suggested resection plane to include mediastinal and periesophageal tissue but to avoid trauma to the adjacent structure, such as the airway, to obtain negative radial margins. |
consensus regarding the optimal approach to and extent of lymphadenectomy has not yet been achieved.
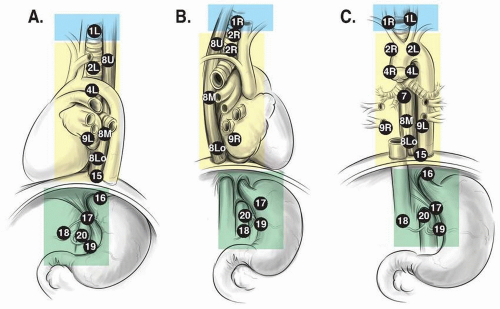 FIGURE 7-3 Regional lymph node stations for staging esophageal cancer. Cervical (blue), mediastinal/thoracic(yellow) and abdominal (green) lymph nodes. Two field lymphadenectomy includes the mediastinal/thoracic and abdominal lymph nodes while three field lymphadenectomy includes the cervical, mediastinal/thoracic and abdominal lymph nodes. The eighth edition of the AJCC uses the number of metastatic lymph nodes from any of the fields as the basis for N staging. A = left sided, B = right sided, C = anterior |
of the stomach into the chest or neck for anastomosis with the proximal esophagus. Therefore, with two of the four major vessels supplying the stomach divided, the most proximal end of the mobilized stomach is always relatively ischemic. Previous anatomic studies investigating the vasculature of cadaveric adult stomachs with angiography have demonstrated that the arterial supply to the gastric conduit is derived entirely from the caudal end of the conduit.30,31,32,33,34,35 The right gastroepiploic arcade provides the vast majority, if not all, of the arterial inflow to the conduit. Both the celiac axis through the gastroduodenal artery and the superior mesenteric artery through the pancreaticoduodenal arteries supply the gastroepiploic artery. The right gastric artery also provides inflow to the conduit from the celiac axis through the hepatic artery. The left gastroepiploic arcade and short gastric vessels arise from the splenic artery. Retrograde flow from intramural and highly variable anastomoses between the right and left gastroepiploic arcades may play a role in perfusion of the cranial aspect of the gastric conduit.32,35
Technical errors and poor perfusion of the gastric conduit at the anastomotic site likely account for the majority of these leaks. Based on the previously mentioned anatomic studies, inadequate perfusion of the gastric conduit and resulting anastomotic leaks may be related to the manner in which the conduit is fashioned.30,31,32,33,34,35 However, only a limited number of studies have assessed the potential association of gastric conduit width and anastomotic leak.
 FIGURE 7-4 A conduit width that is <4 cm in diameter increases the preservation of submucosal blood supply and viability. |
whole stomach was used as a conduit (1% vs. 7.9%; P = 0.021). Subgroup analysis by route of the conduit revealed consistent results favoring a whole-stomach conduit. Finley41 retrospectively reviewed single-institution outcomes of 295 patients treated with esophagectomy for management of malignant disease using a transhiatal approach with a 4-cm gastric tube, using a McKeown approach with a whole-stomach conduit and a thoracoabdominal approach with anastomosis to the “distal stomach.” Cervical anastomoses were performed with the transhiatal and McKeown approaches, whereas an intrathoracic anastomosis was used with the thoracoabdominal approach. The majority of patients had a gastric-emptying procedure with either a pyloroplasty or pyloromyotomy. Anastomotic leak rates were similar irrespective of operative approach or conduit width (tubular/transhiatal, 16%; whole stomach/McKeown, 22%; distal stomach/thoracoabdominal, 14%; P = not significant [NS]).
gastric-emptying procedures have been proposed to decrease the resistance at the level of the pylorus, thereby facilitating emptying of the denervated conduit. Despite the literature on these topics, definitive answers have not emerged.
foods within 1 week after normal findings on an esophagram routinely performed on postoperative day 7. DGE was significantly higher when the whole stomach was used (n = 15; 37.5%) than with wide (n = 9; 13.8%; P = 0.05) and narrow (n = 1; 2.8%; P = 0.007) gastric conduits. No difference in DGE was noted comparing wide with narrow conduits (P = 0.02), nor was there a difference with or without a pyloroplasty in the whole-stomach and wide-conduit cohorts.
the drainage-no drainage divide included studies from Mehran et al55 (34% vs. 32%), Cerfolio et al50 (17% vs. 22%), and Palmes et al53 (16% vs. 13%). These studies reported perioperative mortality rates of 1% to 3%, which included patients who died of pulmonary complications.
function between the use of the whole stomach or a 4- to 5-cm conduit, but we recommend a gastric-emptying procedure to reduce the inherent 15% to 20% risk of DGE.
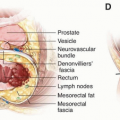
routes of reconstruction (e.g., posterior mediastinum or retrosternal; see Fig. 7-6). The posterior mediastinal route in the esophageal bed is ideal because it is the shortest and has an excellent functional result for patients undergoing immediate reconstruction. Unfortunately, significant scarring from prior esophagectomy makes this route impossible in those patients who have undergone esophagectomy. In these cases, a retrosternal approach is recommended.44 If the retrosternal route is not an option (e.g., previous cardiac surgery), the subcutaneous route is also an option although less optimal because of the longer length of conduit needed. Finally, mesenteric angiography interrogates the superior mesenteric artery to rule out calcification or disease, provides anatomic information in patients who have had previous abdominal surgery, and importantly reveals the configuration of the jejunal arcades. Colonoscopy or barium enema allows the entire colonic mucosa to be examined, and biopsies of suspicious areas may be performed if found.
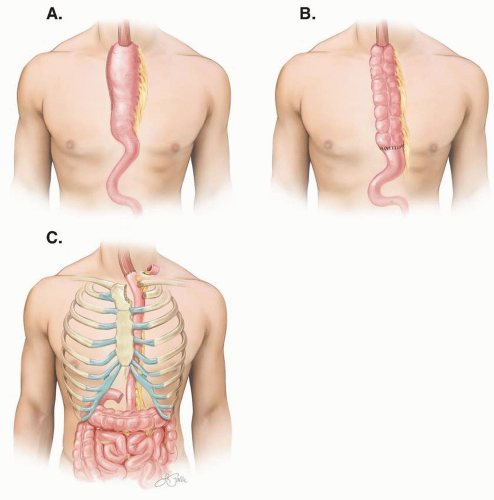 FIGURE 7-5 Stomach (A), colon (B), and jejunum (C) are the most commonly used conduits for esophageal replacement. |
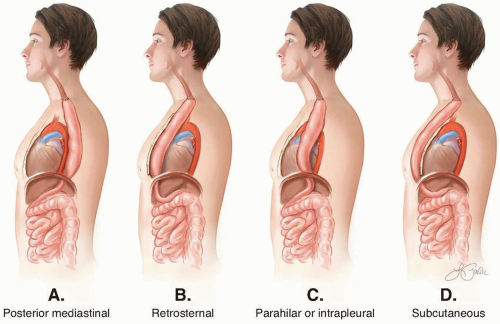 FIGURE 7-6 The posterior mediastinal route (A) requires the shortest length of conduit for reconstruction. When the posterior mediastinal space is obliterated or unavailable, the retrosternal (B) and rarely parahilar (intrapleural) (C) or subcutaneous (D) routes are used. |
midline space behind the manubrium. The retrosternal tunnel is then completed by blunt distal dissection from the superior and inferior entry sites. The neck incision is created, and the left clavicular head, first rib, and the left half of the manubrium are resected to create space for the jejunum or colon to enter the neck without constriction. This also prevents venous congestion of the conduit from compression by the thoracic inlet. This holds true for any retrosternal conduit—gastric, jejunal, or colonic (Fig. 7-7).31,44,63,64
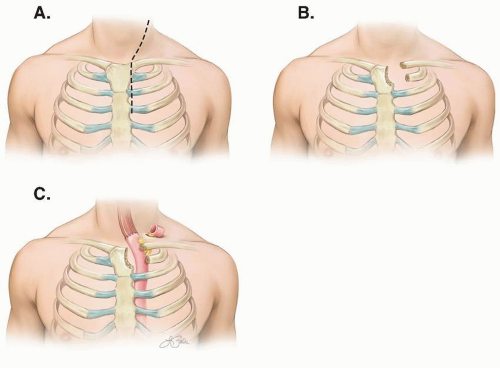 FIGURE 7-7 The cervical incision (A) and resection of a portion of the manubrium, first rib, and clavicular head (B) to accommodate the conduit without kinking or impingement. A small portion of a jejunal graft is externalized as a “monitoring flap” (C) of graft perfusion. |
vascular arcades or creating an intimal flap within the delicate vessels. Microvascular anastomoses are performed between the most proximal jejunal arcade (most commonly the second jejunal artery and vein) and either the internal mammary vessels (artery and vein) or the external jugular vein and branch of the external carotid artery. Anastomosis is performed under the microscope. In some cases, there is inadequate length, and the saphenous vein must be harvested to bridge the gap.31,65
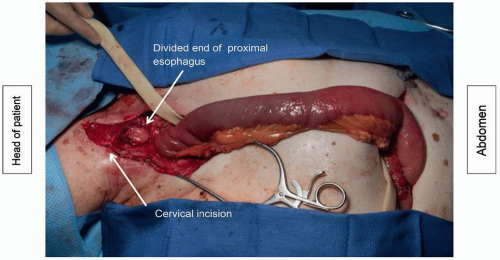 FIGURE 7-8 Jejunal conduit is draped over the sternal region to evaluate for adequate length of a viable portion of the bowel. |
95% CI, 1.1-10.8; P = 0.03).71,72 It is hypothesized that this difference may be explained by the finding of less tissue ischemia with an intrathoracic anastomosis because of the shorter length the blood supply must travel and therefore less tension on the intrathoracic anastomosis.71,72,73
TABLE 7-1 Characteristics and Results of Relevant Prospective Randomized Trials Regarding Anastomotic Location and Technique | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
of combining the heterogeneous data of these RCTs. Therefore, robust, adequately powered studies with a standardized surgical technique are warranted to determine potential differences between intrathoracic and cervical anastomoses.
techniques. However, in one subgroup analysis of 302 patients, it was suggested that stapling might have a benefit over single-layer, hand-sewn esophagogastric construction in reducing the risk of anastomotic leakage (relative risk [RR] = 0.37; 95% CI, 018-0.76; P = <0.01).85 Except for the single-layer hand-sewn technique, the current evidence suggests that it is appropriate to consider both anastomotic techniques (handsewn vs. stapled) as equivalent options for esophagogastric anastomotic construction.
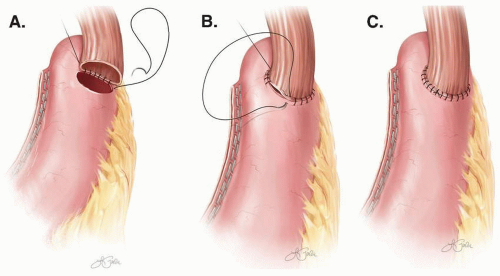 FIGURE 7-9 The hand sewn end to side anastomosis approximates the end of the esophagus to a gastrotomy made in the side of the gastric conduit (A). It can be performed in an interrupted or running (B) fashion. The gastrotomy should be positioned to avoid proximity to the gastric staple line along the lesser curvature and the gastroepiploic/short gastric vessels on the greater curvature when the anastomosis is completed (C). |
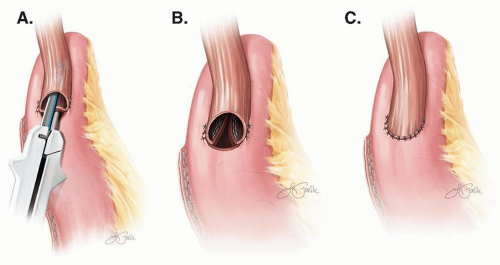 FIGURE 7-10 The esophagus is aligned along the gastric conduit (A) with enough overlap to accommodate the anvil and cartridge of a linear stapler (B) through the open end of the esophagus and a gastrotomy. Firing the stapler creates a common channel to form to back wall of the anastomosis. The remaining opening is closed with suturing (shown) or stapler (not depicted) (C). The gastrotomy should be positioned equidistant from the gastric staple line and greater curvature to decrease the incidence anastomotic ischemia. |
staples and further fibrosis. Of note is the lack of a consensus definition on diagnostic criteria for anastomotic strictures, which is an important limitation when comparison between trials is attempted.
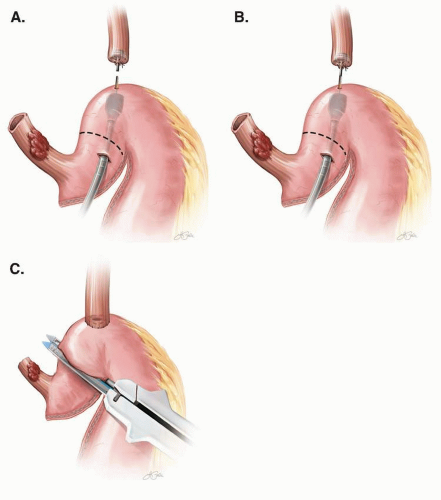 FIGURE 7-11 One method of performing an end to end stapled anastomosis requires inserting the anvil into the proximal stump of the esophagus and securing the open end around the anvil stem with a purse string suture (A). The cartridge is inserted through a gastrotomy in the proximal stomach and a puncture is made in the gastric wall where the anastomosis is planned to join the cartridge to the stem (B). After the stapler is fired, the portion of the stomach with the gastrotomy and GE junction is amputated with a linear stapler (C). |
then applied to include nonrandomized clinical trials including retrospective case series and comparative studies. Abstracts were reviewed and included if they met criteria of adenocarcinoma in all or most of the cohort, had >30 patients, provided a comparison between endoscopic eradication therapy and surgery, and described long-term outcomes after treatment with either endoscopic eradication therapy or surgery. Studies were excluded if they were case reports or reviews, contained cohorts of either all or mostly squamous cell carcinoma, did not contain patients with invasive adenocarcinoma, or did not report either long-term overall survival or disease-related survival. Full-text review of the selected articles applied the same inclusion and exclusion criteria. Articles selected were assessed according to the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system, and Table 7-2 was created. 111 Recommendations were made based on the strength of available evidence.
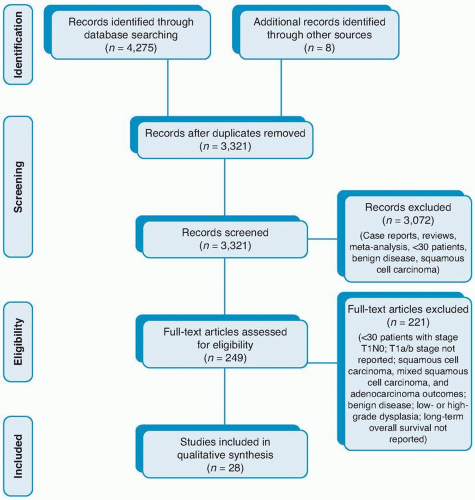 FIGURE 7-12 Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram: T1N0 esophageal adenocarcinoma. |
TABLE 7-2 Results and Characteristics of Observational studies of T1N0 Esophageal Adenocarcinoma | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


