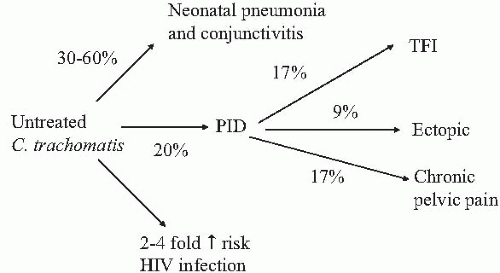
Chlamydia trachomatis infections are the most commonly reported notifiable disease in the United States. In addition, C. trachomatis is the most common bacterial sexually transmitted infection in the United States, with an estimated 3 million new infections occurring annually at an estimated cost of more than $2 billion (Box 3.1). Three fourths of these healthcare costs associated with chlamydial infection in the United States involve women. Globally, C. trachomatis is also the most common sexually transmitted bacterial infection, with an estimated 92 million new cases annually. Most concerning is the recognition that the long-term consequences of chlamydial infection occur most frequently in women (Fig. 3.1). In large part, this is because of the risk of women infected with C. trachomatis for developing pelvic inflammatory disease (PID) and its sequelae of tubal factor infertility, ectopic pregnancy, and chronic pelvic pain. Additionally, pregnant women infected with C. trachomatis but untreated are at increased risk for adverse pregnancy outcome including preterm delivery, premature rupture of the membranes, low-birth-weight infants, and neonatal death. Infants born to mothers with untreated chlamydial infection of the cervix are at increased risk to develop neonatal conjunctivitis and/or pneumonia. Chlamydia trachomatis also can facilitate transmission of human immunodeficiency virus (HIV) infection.
During the past 20 years, the spectrum of diseases caused by C. trachomatis has expanded dramatically (Table 3.1).Chlamydia trachomatis has long been known as the causative agent of trachoma, a disease that is hyperendemic in many developing countries and considered to be the leading preventable cause of blindness in the world. Chlamydia trachomatis is the pathogen long known to cause lymphogranuloma venereum (LGV) and inclusion conjunctivitis of the newborn. Since the early 1980s, chlamydial infections of the genital tract and the consequences of perinatal exposure, both maternal and neonatal, have received considerable attention. More recently, attention has focused on the adverse effects on reproductive health associated with the sequelae of upper genital tract infections with C. trachomatis in women and the role of chlamydial infection in asymptomatic (unrecognized) PID.
Thus, C. trachomatis is a high-prevalence sexual pathogen that is associated with a wide variety of complications. Unfortunately, the majority (up to 85% to 90%) of chlamydial infections of the lower genital tract in women are asymptomatic and if not detected and treated can spread to the upper genital tract, resulting in PID and its associated complications of tubal factor infertility, ectopic pregnancies, and chronic pain. Similarly, unrecognized maternal chlamydial infection causes neonatal conjunctivitis, chlamydial pneumonia of the newborn and fetal wastage, premature ruptured membranes, preterm labor and/or delivery, and neonatal death.
BOX 3.1 ▪ CHLAMYDIA INFECTION IN THE U.S.
Most common reported communicable disease
Most common bacterial STD
Easy to diagnose and treat
If not treated results serious complications
Paradoxically, although chlamydial infections are readily detected with diagnostic tests utilizing new technology (e.g., nucleic acid amplification tests, DNA probes) and are easily treated, the failure to routinely screen sexually active women, especially those younger than 25 years, for chlamydial infection exposes those women infected with chlamydia to significant adverse effects on their reproductive health and the health of their newborn infants.
THE ORGANISM
There are four recognized species within the genus Chlamydia: C. trachomatis, C. psittaci, C. pneumoniae, and C. pecorum(Table 3.2).Chlamydia psittaci is the causative agent of psittacosis, a common pathogen in avian species and lower mammals. Human C. psittaci infectious are rarely found in the United States. Chlamydia pneumoniae (Taiwan acute respiratory) is a major cause of acute respiratory tract infections. The clinical syndromes associated with C. pneumoniae infection include bronchitis, pneumonia, otitis, pharyngitis, and sinusitis. It has also been suggested that C. pneumoniae may play a role in coronary artery disease as a consequence of the inflammatory response to C. pneumoniae. Although high levels of antibody to C. pneumoniae have been detected in patients with coronary artery disease and chlamydial antigen and genes have been detected in atherosclerotic lesions, the causative role of C. pneumoniae in coronary artery disease remains controversial. Chlamydia pecorum is a recently recognized species that formerly was a subset of C. psittaci, which causes disease in the reproductive tract of sheep, cattle, and swine. Except for a few strains of rodent origin, C. trachomatis is a specific human pathogen. Although all chlamydiae share a common genus-specific antigen (chlamydial lipopolysaccharide), C. trachomatis may be further differentiated on a serologic basis. There are currently 15 recognized serotypes (Table 3.2). The C. trachomatis serotypes are responsible for three major groups of infections. Three of these serotypes (L1, L2, L3) represent the agents causing lymphogranuloma venereum and are more invasive than the remaining chlamydial serotypes. Serotypes A, B, Ba, and C are the agents responsible for endemic blinding trachoma. The remaining serotypes of C. trachomatis (D, E, F, G, H, I, J, K) are the oculogenital and sexually transmitted strains that cause inclusion conjunctivitis, newborn pneumonia, urethritis, cervicitis, epididymitis, PID, acute urethral syndrome, and perinatal infections.
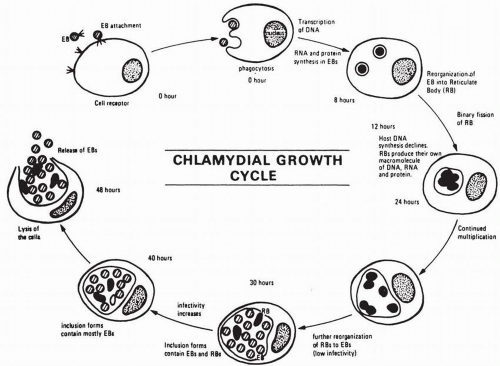
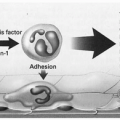
Chlamydiae have a unique growth cycle (Fig. 3.2) that distinguishes them from all other microorganisms. The chlamydial organism exists in two forms: (i) the elementary body, which is the infectious particle and capable of entering uninfected cells; and (ii) the reticulate body, which is the metabolically active and reproductive form that multiplies by binary fission to produce the inclusions that are identified in properly stained cells.
The life cycle of chlamydiae can be divided into several steps: (i) initial attachment of the elementary body (infectious particle) to a host cell; (ii) entry into the host cell; (iii) morphologic change into the reticulate body with subsequent intracellular growth and replication; (iv) transformation of the reticulate bodies into the elementary bodies; and (v) release of the infectious elementary bodies, whereby adjacent cells can be infected, elementary bodies ascend to upper genital tract, and vertical or horizontal (sexual) transmission occurs.
The host cells are generally nonciliated columnar or cuboidal epithelia such as those found in the conjunctiva, urethra, and endocervix and the mucosa of the endometrium and fallopian tubes. After the elementary body attaches to the host cell, it is rapidly ingested by a phagocytic process similar to ordinary bacterial phagocytosis. This process is an enhanced phagocytosis, which is induced by the elementary bodies, which then are selectively taken up by the susceptible host cell. Intracellularly, the elementary bodies exist within a cytoplasmic vacuole. Chlamydiae remain within this phagosome throughout their entire growth cycle. In this state, chlamydiae may be protected from host defense mechanisms such as cellular lysosomes. In the next step of the chlamydia growth cycle, the elementary body, approximately 8 hours after entry, undergoes reorganization into the reticulate body, which represents the metabolically active and dividing form of the organism. These forms are not infectious and will not survive outside the cell. They divide for approximately 8 to 24 hours and then condense and reorganize to form new elementary bodies. Recognition of the characteristic cytoplasmic inclusion is the means by which chlamydiae were classically detected. Infectivity increases as the number of elementary bodies increases, and by 48 to 72 hours the host cell bursts and liberates these infected particles. The complete infectious cycle takes approximately 48 to 72 hours.
Chlamydia trachomatis is an obligatory intracellular bacterium that depends on the host cell for nutrients and energy. Although chlamydiae are capable of limited metabolic activities, they do not possess an enzyme system capable of generating ATP and have been considered energy parasites. Although chlamydiae do not stain with the Gram stain, in many respects they are bacteria-like. They contain DNA and RNA, are susceptible to certain antibiotics, have a rigid cell wall similar in structure and content to that of a Gram-negative bacteria, and multiply by binary fission. Chlamydiae are similar to viruses in that they are obligate intracellular parasites and may be regarded as bacteria that have adapted to an intracellular environment. Thus, they need viable cells for their multiplication and survival.
TABLE 3.2 ▪ CHLAMYDIAE: TAXONOMY AND ASSOCIATION WITH HUMAN DISEASE
Species
Serotype
Disease
Chlamydia psittaci
Many
Psittacosis
Chlamydia pneumoniae
TWAR
Acute upper and lower respiratory tract infections
Chlamydia trachomatis (serotypes A, B, Ba, C) has long been recognized as the causative agent of trachoma, a chronic conjunctivitis affecting an estimated four hundred million people in developing countries and resulting in millions of cases of blindness. In trachomas-endemic areas, child-to-child transmission is the most common method of chlamydial transmission where spread of chlamydial organisms is facilitated by poor hygiene and unsanitary conditions. For the oculogenital serotypes, which are the major focus of this chapter, the primary method of transmission is sexual. Chlamydia trachomatis appears to be more difficult to transmit than Neisseria gonorrhoeae. Among couples with discordant infection status, male-to-female transmission of chlamydia is estimated to occur 40% of the time and female-to male-transmission, 30%.
FIGURE 3.2 Chlamydial growth cycle. EB, elementary body. RB, reticulate body (from Thompson SE, Washington AE. Epidemiology of sexually transmitted Chlamydia trachomatis infections. Epidemiol Rev 1983;5:96-123).
A number of clinical conditions in the female have been attributed to C. trachomatis. These include mucopurulent endocervicitis, endometritis, salpingitis, acute urethral syndrome, urethritis, and perinatal infections. The anatomic site within the female genital tract most commonly infected with C. trachomatis is the cervix. Unfortunately, there are no specific signs or symptoms associated with the cervical infections, and thus many of the chlamydial infections of the cervix are clinically inapparent. This is unfortunate because mucopurulent cervicitis (the female equivalent of nongonococcal urethritis) caused by C. trachomatis predisposes to acute pelvic inflammatory disease in nonpregnant women and to maternal and infant infections during pregnancy. In addition, asymptomatic chlamydial cervicitis is a major reservoir for sexual transmission of C. trachomatis.
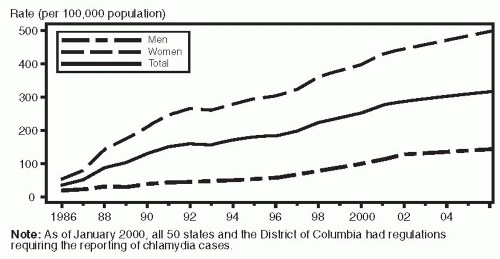
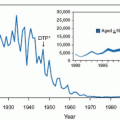
FIGURE 3.3 Chlamydia rates: Total and by sex: United States, 1986 to 2005.
Until recently, genital chlamydial infection was not a reportable disease in the United States. Thus, physician surveys and sentinel surveillance projects were used to estimate national trends. Based on a model using the ratio of chlamydial to gonococcal infections, it was estimated at that time that the annual incidence of genital chlamydial infection was nearly 4.5 million chlamydial infections, with 2.6 million occurring in women and 250,000 among infants. In 1986, the Centers for Disease Control (CDC) made genital chlamydial infection a reportable disease, and, by 2000, all 50 states and the District of Columbia had regulations requiring the reporting of chlamydia cases. In 2006, 1,031,000 chlamydia infections were reported to the CDC, corresponding to a rate of 348 cases per 100,000 population. This is an increase of 5.6% compared with the 2005 rate (Fig. 3.3). With greater than 1 million cases reported, chlamydia cases set a new U.S. record for reported cases of a sexually transmitted diseases (STD) (old record of 1,013,436 gonorrhea cases reported in 1978).
From 1986 through 2006, the rates of reported chlamydia infection increased dramatically from 35.2 to 348 cases per 100,000 population (Fig. 3.3). According to the CDC, the continued increase in reported cases primarily reflects the expansion of screening programs for chlamydia, the development and use of more sensitive screening tests (i.e., nucleic acid amplification tests), and more complete national reporting. The seemingly higher rates among women is misleading and is largely due to the failure of young men to seek preventive services and to be screened for chlamydia.
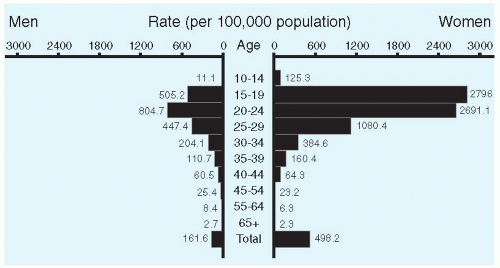
FIGURE 3.4 Chlamydia: Age- and sex-specific rates: United States, 2005.
The highest rates of chlamydial infection in the United States occur among adolescent females and young women (Fig. 3.4). Among routinely screened females ages 16 to 20 years, the rates of chlamydial infection range from approximately 5% to 14%; among women ages 20 to 24 years, 3% to 12% are infected with chlamydia. In a recent large, cross-sectional analysis of a nationally representative sample of young adults ages 18 to 26 years (National Longitudinal Study of Adolescent Health), the overall prevalence of chlamydial infection was 4.19% (95% confidence interval [CI], 3.48% to 4.90%). Nearly 5% of young women were infected (men, <4%), with chlamydial infection rates sixfold greater in African-American young women than in white young women.
Although the rate of reported chlamydia infections among blacks was greater than 8 times higher than that of whites (1,247.0 and 152.1 cases per 100,000, respectively), chlamydia rates continued to increase for all race/ethnic groups in the United States. The rates among American Indian/Alaska Natives (748.7) and Hispanics (459.0) were also higher than that of whites.
Current estimates of the annual incidence of new chlamydia infections in the United States range from 3 to 4 million cases. Because reporting for chlamydia remains fragmentary, screening is sporadic among various populations, and testing for chlamydia is inadequate (e.g., antigen detection versus nucleic acid amplification tests), it is likely that these data underestimate the true incidence of chlamydial infection in the United States. Of the reported U.S. cases, the majority are in women and approximately three fourths occurred in the 15-to 24-year age group. These reported rates for women are an overestimate of the female-to-male ratio of chlamydial infection because women are much more likely to be screened (Fig. 3.3). In areas where intensive chlamydia control programs have been instituted (e.g., Sweden, Pacific Northwest, and Wisconsin), dramatic decreases (>50%) in the prevalence of chlamydia have occurred.
Many sexually active women have been exposed to chlamydiae. The prevalence of serum antibody to C. trachomatis increases with age until about 30 years, when it plateaus at approximately 50%. Most of the women with antibody titers against chlamydia do not have a current infection. In general, between 3% and 5% of unselected asymptomatic nonpregnant women younger than 26 years have C. trachomatis isolated from their cervices. However, the prevalence of chlamydial infection depends on the population of women screened, and, in selected populations, C. trachomatis is more prevalent (Table 3.3).
Several patient characteristics have been found to be predictors of chlamydial genital infections among sexually active females. These risk factors for chlamydial infection include age 25 years or younger, more than one sexual partner, early onset of sexual intercourse, a recent new sexual partner, African-American race, being unmarried, history of other sexually transmitted infections, no method of contraception or nonbarrier methods of contraception (especially oral contraceptive use), cervical ectopy, and douching. Among these risk factors, young age is most strongly associated with chlamydial infection (Fig. 3.4). The inverse relationship to age is caused by increased sexual activity among younger women and the large squamocolumnar junction present in young adolescents, which provides a larger target area for infection with chlamydia.
The majority of women with chlamydial disease remain untreated because their infection is either asymptomatic or relatively inapparent. In general, one half to two thirds of chlamydial infections of the cervix are asymptomatic. If not treated, the infection can persist for several years and subject those infected to the risks of spread of C. trachomatis to the upper genital tract, with subsequent infertility and ectopic pregnancy. The unfortunate paradox of chlamydial infections is that although they can be easily diagnosed and treated, the failure to do so places young women at substantial risk for sequelae such as PID, infertility, ectopic pregnancy, chronic pelvic pain, preterm labor, and neonatal infection. In addition, women infected with chlamydia are at increased risk for HIV infection (Box 3.2).
TABLE 3.3 ▪ PREVALENCE OF CHLAMYDIAL INFECTION IN SELECTED POPULATIONS
Population
Prevalence of Chlamydial Infection
STD clinics
15% to 33%
Female partners of men with nongonococcal urethritis
29% to 68%
Female partners men with chlamydial urethritis
67% to 74%
Women with mucopurulent cervicitis
28% to 63%
Family planning clinics
2.8% to 9.4%
Female college students
2% to 7%
Gynecology clinics and women attending primary care clinics
3% to 5%
Community-based screening (urine NAAT)
8.6%
Female military recruits
8.5% to 9.9%
Adolescent females
10% to 40%
Pregnant women
2% to 37%
NAAT, nucleic acid amplification test.
BOX 3.2 ▪ COMPLICATIONS OF CHLAMYDIAL INFECTION
Pelvic inflammatory disease
Tubal factor infertility
Ectopic pregnancy
Chronic pelvic pain
↑ risk for HIV infection
Adverse pregnancy outcomes
Neonatal infection
Both medically and economically, PID is the most important consequence of chlamydial infection. More than 1 million women develop PID each year in the United States. Studies in the United States suggest that up to 20% to 50% of these cases are associated with C. trachomatis. Recently, it has been recognized that approximately 25% of women with untreated cervical chlamydial infection develop subclinical (asymptomatic, unrecognized) PID. In addition, these women with both clinical and subclinical PID are exposed to a significantly increased risk for infertility and ectopic pregnancies. The implications of these data are discussed in greater detail in Chapter 13.
The infant born to a woman with a chlamydial infection of the cervix is at 60% to 70% risk of acquiring the infection via vertical transmission during passage through the birth canal. Approximately 25% to 50% of exposed infants will develop chlamydial conjunctivitis in the first 2 weeks of life, and 10% to 20% of the infants will develop chlamydial pneumonia within 3 to 4 months of birth. In addition, women with undetected cervical infection are a reservoir for horizontal transmission to their sexual partner(s). These significant complications associated with vertical transmission to newborns, horizontal transmission to partners, and ascending genital tract infection with C. trachomatis strongly demonstrate the need for large-scale screening programs to detect cervical chlamydial infections. As noted above, when such chlamydia control programs have been undertaken, a dramatic impact on lowering the rate of genital chlamydial infection and their complications (e.g., PID) occurs.
CHLAMYDIAL INFECTION IN MEN
Chlamydial infection in men manifests in multiple sites and presents as urethritis, epididymitis, prostatitis, or Reiter’s syndrome (reactive arthritis post urethritis). Reported cases of chlamydial infection in men (Fig. 3.3) provide a misleading picture of the relative frequency of chlamydial infection in women and men. The dramatic discrepancy is due to young men not seeking routine or preventive care.
CHLAMYDIAL INFECTION IN WOMEN
In many ways, the clinical spectrum and epidemiology of C. trachomatis infection in women are similar to those associated with gonococcal infection. However, there are also major differences. Chlamydial infection is generally more frequent, often asymptomatic, may be associated with nonspecific symptoms, or may exist in the absence of any visible signs of infection. The diagnosis can be proven only by culture, antigen detection methods, DNA probes, or nucleic acid amplification tests (NAATs).
Despite the absence of clinically apparent disease, women infected with C. trachomatis may harbor the organism for long periods of time. Based on longitudinal studies of women in Bogota, Colombia, 50% of chlamydial infections persisted at 1 year, 20% at 2 years, and 10% at 3 years. The incubation period for C. trachomatis is 6 to 14 days, which is considerably longer than that for N. gonorrhoeae. As a result of the longer incubation period, the high rate of asymptomatic infection, and the persistent carrier state, a large reservoir of C. trachomatis infection exists in the population. Moreover, this reservoir in the lower genital tract places women at risk for ascending infection to the upper genital tract with its resultant adverse effect on future reproductive health and for adverse perinatal outcomes.
Bartholinitis
Chlamydia trachomatis produces an exudative infection of Bartholin’s ducts similar to that seen with N. gonorrhoeae. Concurrent infections with gonococci are often present. However, the proportion of cases of bartholinitis associated with chlamydial infection is unknown.
Endocervicitis
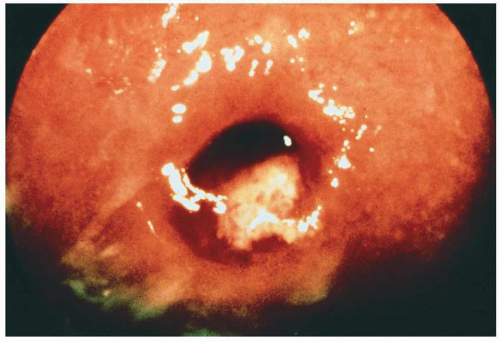
The anatomic site within the female genital tract most commonly infected with C. trachomatis is the cervix. Chlamydia trachomatis is a major cause of mucopurulent cervicitis (MPC) (Fig. 3.5). However, up to two thirds of women with chlamydia infection of the cervix do not have signs or symptoms of infection. Chlamydia trachomatis does not cause vaginitis because it does not attach to and will not grow in vaginal squamous epithelial cells. The organism appears to be a specific parasite of squamocolumnar and columnar cells and thus grows only within the transitional zone and the endocervix. The infected cervix may range from a clinically normal examination to a severely eroded cervix with a hypertrophic cervicitis and a mucopurulent endocervical discharge. Hypertrophic cervicitis is the term applied to the presence of cervical ectopy, which is edematous, congested, and friable. Use of colposcopy to evaluate the sexual partners of men with nongonococcal urethritis demonstrated that in women with positive endocervical cultures for C. trachomatis, more than 80% had hypertrophic cervicitis with mucopurulent endocervical discharge. This association between mucopurulent endocervicitis and isolation of C. trachomatis from the endocervix has been confirmed in multiple studies. It has been suggested that MPC is the female counterpart of nongonococcal urethritis in the male.
FIGURE 3.5 Chlamydial mucopurulent cervicitis.
MPC is diagnosed by demonstrating (i) yellow or green mucopus on a swab of endocervical secretions (“positive swab test”); (ii) more than 10 polymorphonuclear (PMN) leukocytes per oil immersion field of a Gram stain of the endocervix; or (iii) friability, erythema, or edema within a zone of cervical ectopy. A cutoff of ≥30 PMN leukocytes per ×1,000 field in Gram-stained smears of cervical mucus has been suggested to best correlate with chlamydial cervicitis.
Although the positive predictive value of mucopurulent cervicitis for identifying women with chlamydial cervicitis is high in populations at high risk for chlamydial infection [e.g., STD clinic patients, nonpregnant adolescents with high prevalence rates (>15%), or other high-prevalence groups of women], in the general population of low-risk patients, the positive predictive value is low.
Women with clinical signs of chlamydial cervicitis such as mucopurulent discharge or hypertrophic ectopy yield greater numbers of chlamydial inclusion-forming units than those in whom chlamydial infection is not associated with signs or symptoms of cervicitis. Similarly, chlamydia infection occurs more frequently in women with cervical ectopy than in those without. In sexually active adolescents, cervical ectopy is present in 60% to 80% of young women, which is a much higher prevalence than that seen in the third and fourth decades. Possibly, ectopy predisposes to chlamydial infection by providing exposure of more susceptible columnar epithelial cells to C. trachomatis. This relationship may in part explain the high prevalence of chlamydia cervical infection among adolescents. Similarly, oral contraceptives are associated with ectopy, and this relationship may explain the increased risk for C. trachomatis infection of the cervix among users of oral contraceptives.
It seems apparent that cervical infection with C. trachomatis is a major reservoir for the male and neonatal infections associated with this agent. In addition, the cervix is the source for major complications involving the upper genital tract, such as acute PID. Thus, it is imperative that efforts be made to identify those women who are symptomatic and asymptomatic carriers of C. trachomatis in their cervix. As noted above, in geographic areas where intensive chlamydia control programs have been implemented, the prevalence of C. trachomatis infection and the incidence of acute PID have been significantly reduced.
Acute Urethral Syndrome
The acute urethral syndrome, which is defined as acute dysuria and frequent urination in women with pyuria but whose voided urine is sterile, is a common and perplexing problem for the clinician. Up to 25% of women whose male partners had chlamydial urethritis have chlamydial infection in their urethra. Based on studies in STD clinics with women cultured for C. trachomatis from the cervix and urethra, 25% of positive women harbor the organism only in their urethra; an additional 50% harbor the organism in both their cervix and urethra. This emphasizes the importance of screening both the cervix and urethral sites for chlamydial infection in women.
Chlamydia trachomatis is the etiologic agent in up to 25% of women presenting with the acute urethral syndrome. On the other hand, C. trachomatis was unlikely to be recovered from women with acute cystitis or those women with the urethral syndrome and bladder bacteriuria.
The clinician must be aware that C. trachomatis will not be recovered from the urine but that culture attempts must be performed via urethral swabs. NAATs can also be used on urine specimens to identify the presence of chlamydia. Several findings on history are suggestive of C. trachomatis being the causative agent in women presenting with symptoms of acute urethral syndrome. These include a recent change in sexual partner, the use of oral contraceptives, and a longer duration of presenting symptoms (approximately 7 to 10 days), as compared with women with acute cystitis or bacteriuria who present within 4 days. In addition, women with chlamydia are less likely to give a history of recurrent urinary tract infections, which is in contradistinction to those women with acute cystitis or bladder bacteriuria.
Antimicrobial therapy of the acute urethral syndrome using an agent effective against C. trachomatis is significantly more effective than placebo in eradicating urinary symptoms, pyuria, and the infecting microorganism among women with the urethral syndrome due to coliforms, staphylococci, or C. trachomatis. In contradistinction, those women with acute urethral syndrome and no pyuria do not benefit from antibiotic therapy.
Nonpuerperal Endometritis
Multiple investigations have demonstrated that endometritis in nonpregnant women is another manifestation of genital chlamydial infection. Histologic endometritis based on the presence of plasma cells and infiltration of the superficial epithelium by PMN leukocytes has been detected in nearly one half of patients with chlamydial mucopurulent cervicitis. The presence of histologic endometritis has been associated with both cultural and immunohistologic detection of C. trachomatis. In addition, histologic endometritis can be detected in nearly all patients with chlamydial salpingitis. Recently, histologic endometritis has been termed subclinical or unrecognized PID. Histologic endometritis has also been demonstrated with N. gonorrhoeae and the mixed anaerobic and aerobic bacteria associated with bacterial vaginosis. The impact of subclinical PID is discussed in detail in Chapter 13.
Chlamydia ascends from the cervix and affects the uterine mucosa and then spreads intracanalicularly from the endometrium to the fallopian tubes. In studies from Sweden, San Francisco, and Seattle, 25% to 50% of patients with laparoscopically confirmed PID had C. trachomatis recovered from the endometrium. Taken together, these studies demonstrate that endometritis is an important component of PID and an intermediate step in the spread of microorganisms from the cervix and/or vagina to the fallopian tubes.
The abnormal uterine bleeding (menorrhagia and metrorrhagia) often seen in patients with acute PID is probably caused by the presence of concomitant endometritis. In Chapter 13, the role of persistent C. trachomatis, production of heat shock proteins, and initiation of the cell-mediated immune response leading to damage of the fallopian tube are discussed in detail. Clearly, such a mechanism may explain a proportion of tubal factor infertility cases in which no history of an acute episode of PID exists.
Acute Pelvic Inflammatory Disease
The most serious complication of chlamydial infection in women is acute salpingitis (i.e., PID). The role of C. trachomatis as a pathogen in this disease has received considerable recent attention. Interestingly, the association of chlamydial infection of the female genital tract (as determined by giving birth to an infant with inclusion conjunctivitis) and PID in the postpartum patient was initially recognized by ophthalmologists in the 1930s.
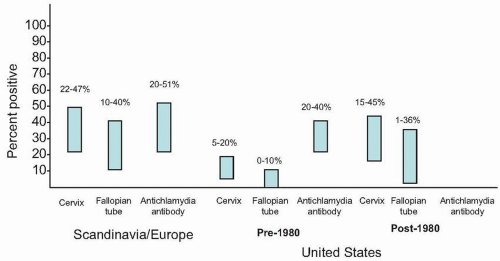
Microbiologic and serologic studies have firmly established C. trachomatis as an important sexually transmitted organism that leads to acute PID (Fig. 3.6). Initial evidence that C. trachomatis is an important etiologic agent in acute salpingitis came from Scandinavian investigators, who used laparoscopy to isolate C. trachomatis from the fallopian tubes of women with documented PID. However, the frequency of chlamydial PID appeared to differ in various geographic locales. The Scandinavian investigations suggested that approximately half of acute salpingitis occurring in that area were caused by C. trachomatis, whereas in North America, initial results were not as clear-cut.
In addition to the isolation studies, a number of investigations have indirectly associated acute salpingitis with chlamydial infection. In Scandinavia, serologic studies also indicated that C. trachomatis is a frequent causative agent in acute salpingitis. These studies demonstrated that 19% to 80% of acute salpingitis patients had antichlamydial antibody present or a fourfold rise in chlamydial antibody. The level of antibody titers was correlated with the severity of clinically graded tubal inflammation seen at the time of laparoscopy. Taken together, these studies from Scandinavia suggest that in the 1970s and 1980s, the major etiologic agent for acute salpingitis in that geographic area was C. trachomatis. Based on culture data and serologic data, somewhere between 30% and 67% of acute salpingitis was associated with chlamydia as the etiologic agent in Scandinavia. Further support for the role of chlamydia in acute PID came from a treatment study for gonorrhea in the United Kingdom, where women were randomly treated with penicillin or tetracycline. A significantly greater proportion of those who received penicillin (not effective against concurrent C. trachomatis) subsequently developed acute PID with documented persistence of C. trachomatis in the cervix.
Until the mid-1980s in the United States, evidence suggested that chlamydia-associated acute salpingitis was much less frequent than what has been reported from Scandinavia (Fig. 3.6). These initial studies noted the recovery of C. trachomatis from the fallopian tube or cul-de-sac aspirate in 0% to 10% of patients with acute salpingitis. In summary, studies emanating from Scandinavia demonstrated a twofold increased cervical isolation rate of C. trachomatis and a 20-fold increased fallopian tube isolation rate, as compared with the initial U.S. studies. Despite apparent differences in these recovery rates, the serologic evidence for an association between chlamydia and PID were quite similar. In the United States, serologic evidence for chlamydial infection was noted in 20% to 25% of patients diagnosed with acute PID.
Several factors were postulated to explain these differences between Swedish isolation rates and those in the United States. First, there were significant differences in the methods of collecting specimens. Swedish investigations used needle aspiration and/or needle biopsy of the fimbria at the time of laparoscopy. In the United States, culture attempts had been made on purulent tubal exudates. Because C. trachomatis is an intracellular organism, successful isolation may require the presence of fresh infected cells in the inoculum. A second reason is that the patient groups that have been studied in the United States and Sweden are not comparable. Investigations using intraperitoneal cultures in the United States were based on hospitalized patients who in general presented to emergency rooms with acute disease characterized by high fever and peritonitis. Swedish investigators, on the other hand, evaluated all patients with acute salpingitis, including many with clinically mild disease (often afebrile) who would not have been diagnosed in the United States, where more rigid diagnostic criteria (i.e., fever, leukocytosis) were being applied in the diagnosis of acute PID. Swedish investigators noted that patients presenting with acute salpingitis and C. trachomatis tend to have a milder clinical disease, were less often febrile, and had mild symptoms for longer periods of time than women admitted with gonococcal or nongonococcal-nonchlamydial salpingitis; paradoxically, though, those women documented to have chlamydial salpingitis had the highest erythrocyte sedimentation rates and the more severe inflammatory changes noted at the time of laparoscopy.
FIGURE 3.6 Detection of Chlamydia trachomatis in women with acute pelvic inflammatory disease.
In the mid-1980s, studies in the United States using appropriate methodology for obtaining chlamydial specimens (i.e., tubal biopsy, tubal aspirate, swab or endosalpinx, endometrial biopsy, and/or protected endometrial aspirate) confirmed that C. trachomatis is also a major etiologic agent for acute PID in the United States (Fig. 3.6). Currently it is estimated that C. trachomatis is responsible for 20% to 40% of clinically apparent acute PID in the United States.
Recently, it has been estimated that clinically apparent PID (symptomatic) accounts for less than half of the total cases of PID. The remaining cases are caused by subclinical or unrecognized (“silent” or “atypical”) PID. Thus chronic, subacute, or latent upper genital tract infection is present in a large number of women. Both the magnitude of and an accepted definition of these unrecognized infections has not been established. Unfortunately, subclinical PID appears to be as likely to result in progressive scarring of the fallopian tubes resulting in tubal factor infertility and ectopic pregnancy. Furthermore, C. trachomatis appears to be associated with these milder or unrecognized presentation of acute PID.
The ability of C. trachomatis to produce acute salpingitis has further been documented in several animal models including grivet monkeys, pig-tailed macaques, and mice.
Further support for the role of C. trachomatis in the etiology and pathogenesis of acute PID arises from a large number of studies demonstrating a statistically significant association for tubal factor infertility and ectopic pregnancy with previous systemic chlamydial infection identified by the presence of antibody against C. trachomatis. These findings are discussed in the section on sequelae of acute PID in Chapter 13.
PATHOGENESIS OF CHLAMYDIAL INFECTION
Several interesting pieces of evidence support a role for the host defense system in the development of long-term sequelae following chlamydial infection, including PID, tubal factor infertility, and trachoma. Multiple investigations have provided data suggesting that chlamydial PID is a cell-mediated immune disease probably resulting from immune responses to chlamydial heat shock protein 60 (CHSP-60). It has been hypothesized that this inflammatory immune response is similar to a delayed-type hypersensitivity reaction to C. trachomatis antigens leading to repeated and persistent infection, which results in damage to the fallopian tube. Such a response is similar to the mechanism by which C. trachomatis produces scarring and blindness in ocular trachoma.
Persistent and repeated chlamydial infections are particularly associated with pathologic disease and sequelae. Interferon gamma (IFN-γ) plays a major role in the immune response to chlamydia and the subsequent inflammatory process. IFN-γ is a critical factor for induction of delayed chlamydial development and thus restricting chlamydial infection. However, delayed development results in persistent expression of chlamydial heat shock proteins (HSPs), which not only share antigens with other bacterial HSPs but with human HSP. The damage and scarring associated with chlamydial infection appear to be dependent on four mechanisms of chlamydial disease: (i) persistent chlamydial infection; (ii) role of cytokines in chlamydial infection; (iii) role of chlamydial HSPs in the pathogenesis of disease; and (iv) host genotype.
Whereas the normal chlamydial development cycle is a productive cycle of infection resulting in release of infectious elementary bodies, persistent chlamydial infection is associated with incomplete chlamydial development with sporadic release of elementary bodies. This incomplete growth cycle can be induced by either inappropriate antibiotic treatment (e.g., penicillin, cephalosporins) or the cell-mediated immune response (e.g., IFN-γ as discussed above). Such persistent (“latent”) infection can subsequently revert into overt infection and disease.
The hallmark of chlamydial infection is an inflammatory process that is exacerbated by reinfection and subsequently results in tissue damage and scarring. Interaction of C. trachomatis with the cytokine network is a key element in disease production. Multiple investigations in murine models of chlamydial infection have demonstrated the key role played by the cell (T-cell)-mediated immune response in the host immune response against infection with chlamydia. Similarly, in vitro studies have shown that the growth of human strains of C. trachomatis are inhibited by IFN-γ, suggesting that Th1 cytokines including IFN-γ play an important role in protection against human chlamydial infection. Chlamydial infection produces a cytokine response by direct infection of epithelial cells and interaction with cells of the host immune system. Response to chlamydial infection by the cells of the immune system is a Th1-like response with a production of IL-2 and IFN-γ. This Th1 response is crucial to resolving established chlamydial infection. However, as discussed above, it also can result in persistent chlamydial infection and its associated adverse complications.
Taken together, the murine model studies of chlamydial infection produced a paradigm for chlamydia immunity that includes a role for (i) CD4+ Th1 effector cells that secrete IFN-γ, TNF-α, TNF-β, and IL-2 in eradication of infection; and (ii) CD4+ Th1 cells and antigen-specific B cells in resistance to reinfection. Human studies support the concept that the type of immune response (Th1 versus Th2) to chlamydial antigens determines susceptibility and resistance to infection with C. trachomatis.
Heat shock proteins are a family of closely related proteins widely distributed in virtually all organisms and expressed when organisms are exposed to stress. The major chlamydial HSPs (12, 60, and 75 kDa) are partially (40% to 50%) homologous with human mitochondrial proteins HSP 10, HSP 60, and HSP 70. Thus, the concept has evolved that immune responses to chlamydial HSPs, particularly HSP 60, initiates (by antigenic mimicry) an autoimmune response against related human HSPs. Central to this mechanism of pathogenesis is IFN-γ, which, although it inhibits chlamydial development, also permits expression of HSP 60. As an extension of this finding, it appears that in chronically or acutely infected persons, continued chlamydial HSP 60 expression initiates the chronic inflammatory responses associated with fibrosis and scarring characteristic of the sequelae of chlamydial infection (e.g., blinding trachoma, PID, infertility, and ectopic pregnancy). In humans, a number of studies have demonstrated an association between antibody to chlamydial HSPs and the chronic sequelae of chlamydial infection such as PID, infertility, ectopic pregnancy, and perihepatitis.
Only gold members can continue reading. Log In or Register to continue