There has been a virtual revolution in our knowledge related to the etiology, pathogenesis, diagnosis, and treatment of sexually transmitted diseases (STDs) and sexually transmitted infections (STIs), over the past two decades. However, despite these advances, the United States remains in the midst of an epidemic of STDs (Box 5.1). Currently, more than 30 microorganisms, including bacteria, viral agents, protozoan parasites, and ectoparasites, are sexually transmitted (Table 5.1).
The Institute of Medicine in their 1997 report, “The Hidden Epidemic: Confronting Sexually Transmitted Diseases,” sought to raise public awareness regarding the adverse medical and economic impact of STDs in the United States. However, more than a decade later, STDs and STIs remain a major (and growing) public health problem in the United States. According to the Centers for Disease Control (CDC), approximately 19 million new cases of STI occur each year in the United States, with almost half of these infections occurring among adolescents and young people ages 20 to 24 years (Table 5.2). As a result, the United States has the highest rate of curable STDs among the developed countries. In fact, of the 10 most frequently reported diseases in the United States in 2005, four were STDs (Table 5.3), accounting for nearly 90% of the top 10 notifiable diseases. In addition to the significant medical consequences of these infections, STDs result in a substantial economic impact, with estimated annual direct medical costs of $14.7 billion in the United States.
STDs are also significant social, health, and economic burdens worldwide, and STDs (excluding human immunodeficiency virus [HIV]) are estimated to be the second leading cause of lost healthy life among women ages 15 to 44 years in the developing countries of the world. The World Health Organization (WHO) estimates that there are 333 million new cases worldwide of the four curable STDs (gonorrhea, 62.6 million; syphilis, 12.2 million; chlamydia, 89.1 million; and trichomoniasis, 167.2 million) among persons 15 to 49 years of age each year.
Sexually active adolescents have the highest rates of STDs of any age groups. The CDC estimates that approximately 3 million adolescents in the United States acquire an STD each year. Factors that explain why adolescents and young adults are the age groups at greater risk for acquiring a STD include (i) they are more likely to have multiple partners; (ii) they may be more likely to engage in unprotected intercourse; (iii) their partners may be at higher risk of being infected; and (iv) they are more susceptible to cervical infections with gonorrhea, chlamydia, and human papilloma virus (HPV).
It is also notable that, with the exception of acquired immunodeficiency disease (AIDS), STDs are associated with more serious long-term consequences in women than in men. These complications include (i) an increased risk for genital cancer with HPV; (ii) loss of reproductive capability and ectopic pregnancy secondary to damage to the fallopian tubes with Neisseria gonorrhoeae and Chlymydia trachomatis; (iii) complications of pregnancy, including spontaneous abortion, stillbirth, chorioamnionitis, preterm birth, and low birth weight; and (iv) transmission of serious or fatal infections to the fetus or newborn, such as syphilis, HSV, C. trachomatis, cytomegalovirus (CMV), or Hepatitis B virus.
A dramatic change in emphasis in the field of STDs has occurred over the past 100 years. There has been an evolution from concern for the traditional venereal diseases, such as gonorrhea and syphilis, to emphasis on the syndromes associated with C. trachomatis, herpes simplex virus (HSV), and human papilloma virus (HPV), and recently to concern with the potentially fatal disease AIDS, caused by HIV. Although the bacterial STDs (gonorrhea, chlamydia, and syphilis) are easily cured with antimicrobial therapy, the more recently recognized viral STDs are associated with incurable and fatal conditions (HIV with AIDS, HPV with genital cancers, and chronic recurrent HSV).
An epidemiologic synergy exists among STDs. They are historically, biologically, behaviorally, economically, and programmatically related. The ulcerative STDs (syphilis, chancroid, HSV) are associated with increased risk of acquiring and transmitting HIV. STDs that cause cervical discharge (gonorrhea, chlamydia, and trichomoniasis) also enhance the acquisition and transmission of HIV.
GONORRHEA
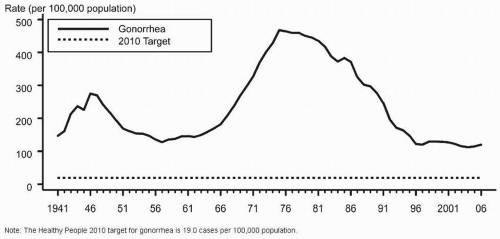
Gonorrhea, which is caused by the Gram-negative diplococcus N. gonorrhoeae, is the second most commonly reported communicable disease in the United States, with 358,366 cases reported in 2006 (second only to chlamydia). Following the peak of 1 million cases reported in 1975 (Fig. 5.1), there was a dramatic decline in the rate of reported gonorrhea rates from 1997 to 2005. Subsequently, reported cases of gonorrhea have increased. In 2006, the gonorrhea rate was 120.9 cases per 100,000 population, an increase of 5.5% since 2005. Because of underreporting, it is estimated that nearly 800,000 cases of N. gonorrhoeae occurred in 2006 in the United States (Box 5.2).
Man is the only natural host for N. gonorrhoeae. Because the organism has a predilection for columnar or pseudostratified epithelium, mucous membranes that are lined by columnar, cuboidal, or noncornified squamous epithelial cells are most susceptible to infection with N. gonorrhoeae in adults. As a result, gonococcal infection is most commonly found in the urogenital tract. N. gonorrhoeae is a fastidious organism with specific nutrient and environmental needs. Its growth is optimal at pH 7.4, temperature 35.5°C, and a 2% to 10% CO2 atmosphere.
BOX 5.1 ▪ STD EPIDEMIC IN UNITED STATES
19 million new STDs annually
50% occur in adolescents and 20-24 year olds
Cost $15 billion annually
Among nonpregnant women, N. gonorrhoeae is an important cause of urethritis, cervicitis, and pelvic inflammatory disease. Pharyngeal gonorrhea and disseminated gonorrhea occur less commonly. Infection with N. gonorrhoeae in pregnancy is also a major concern. Gonorrheal ophthalmia neonatorum has long been recognized as a major consequence of untreated maternal infection. More recently, an association between maternal gonococcal infection and disseminated gonococcal infection, amniotic infection syndrome, and perinatal complications such as premature ruptured membranes, chorioamnionitis, prematurity, intrauterine growth retardation, neonatal sepsis, and postpartum endometritis has been recognized.
Epidemiology
The current epidemic of gonorrhea commenced in 1957 and reached its peak in 1975, with more then 1 million reported cases and a rate of 473 cases in 100,000, a nearly 300% increase in gonorrhea cases between 1966 and 1975. Since then, gonorrhea rates declined dramatically until 1997 (Fig. 5.1), when the rates leveled off. However, in 2005 and 2006, the rates increased for the first time since 1985.
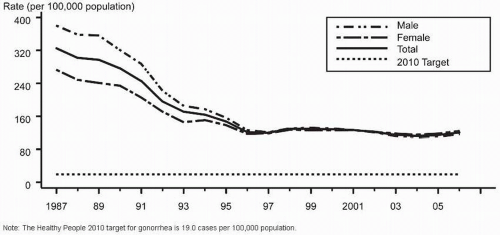
Several important changes in the epidemiology of gonorrhea in the United States have taken place during the past two decades. Whereas in 1987 twice as many cases were reported from public STD clinics than from private providers, by 1996 only slightly more than one half of reported gonorrhea cases were from STD clinics. For women, this pattern is even more dramatic, with nearly two thirds of gonorrhea cases reported from non-STD clinical sites. In 1966, the male-to-female ratio of gonorrhea cases was 3:1. This ratio has declined rapidly, and by 1996 the male-to-female ratio was 1:1 (Fig. 5.2). In fact, since 2002, reported cases and rates of gonorrhea have been slightly higher in women.
TABLE 5.1 ▪ SEXUALLY TRANSMITTED PATHOGENS
Bacterial agents
N. gonorrhoeae
C. trachomatis
T. pallidum
G. vaginalis
H. ducreyi Shigella
Shigella
Campylobacter
Group B Streptococcus
Mobiluncus curtissi, M. mulieris
Genital mycoplasmas
M. hominis
U. urealyticum
M. genitalium
Fungal agents
C. albicans
Viral agents
Human papilloma virus (>25 genital types)
Herpes simplex virus
Hepatitis A virus
Hepatitis B virus
Hepatitis C virus
Cytomegalovirus
Molluscum contagiosum virus
Human Immunodeficiency virus (HIV)
type 1, type 2, subtype 0 HTLV-types I and II
Human herpes virus type 8
Protozoan agents
T. vaginalis
E. histolytica
G. lamblia
Ectoparasites
P. pubis
P. scabiei
TABLE 5.2 ▪ ESTIMATED INCIDENCE AND PREVALENCE OF SEXUALLY TRANSMITTED DISEASES IN THE UNITED STATES, 2004 STD Incidence a Prevalence b
aFrom Weinstock H, Berman S, Cates W Jr. Sexually transmitted diseases among American youth: incidence and prevalence estimates, 2000. Perspect Sexual Reprod Health 2004;36:1-10.
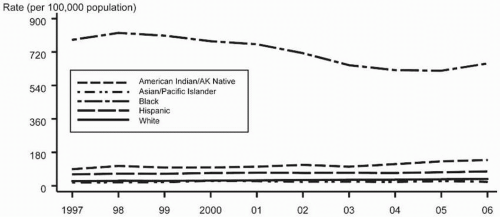
In the United States there is a dramatic variance in the incidence and trends in incidence of reported gonorrhea cases among different racial groups (Fig. 5.3). As of 2006, the rate of gonorrhea in black non-Hispanics was 658.4 in 100,000 compared with 138.3 for American Indian/Alaskan Natives, 77.4 for Hispanics, 36.5 for white non-Hispanics, and 21.1 for Asian/Pacific Islanders. Another important determinant of the incidence of gonorrhea is age. Approximately 75% of reported cases of gonorrhea in the United States in 2006 were among persons ages 15 to 29 years, with the highest rates occurring in the 15- to -19-year-old age group. If only sexually active females are considered, the incidence of gonorrhea is twice as high in adolescents than in women ages 20 to 24 years. In the United States, the highest age and race ethnicity-adjusted rates for gonorrhea among women are in 15- to 19-year-old African-American non-Hispanics, with a 2006 reported gonorrhea incidence of 2,898.1 in 100,000. Additional risk factors for gonorrhea include low socioeconomic status, early onset of sexual activity, unmarried marital status, a history of gonorrhea, illicit drug use, and prostitution.
TABLE 5.3 ▪ MOST COMMONLY REPORTED NOTIFIABLE DISEASES IN THE UNITED STATESa
FIGURE 5.1 Gonorrhea rates: United States, 1941-2006 and the healthy people 2010 target.
Transmission of gonorrhea is almost entirely by sexual contact. The risk of infection in the female is twofold to fourfold higher than for the male. Although it is estimated that a male having a single sexual encounter with a gonorrhea-infected female will become infected 20% to 25% of the time, the risk of transmission from male to female is estimated at 50% to 90%. A short incubation time of 3 to 5 days occurs.
The prevalence of gonorrhea in a community is dynamic, fluctuates over time, and is influenced by a number of interactive factors. Mathematical models have been developed that suggest that the prevalence of gonorrhea is sustained by both continued transmission and by asymptomatically infected individuals and “core-group” transmitters who are more likely to acquire and transmit gonorrhea than the general population. The core group is mainly characterized by residence within inner cities and low socioeconomic status. However, it also includes individuals with repeated episodes of gonorrhea, persons who do not abstain from sex in the face of symptoms and/or exposure to GC, and those who practice high-risk behavior such as prostitution, patronizing prostitutes, or illicit drug use.
Pathogenesis
Over the past 40 years there has been a phenomenal expansion in our understanding of the pathogenic mechanisms of the gonococcus. Initially it was demonstrated that there are differences in the virulence of N. gonorrhoeae associated with specific colony types. Of the Kellogg colony types, only types 1 and 2 (now called P+), which contain pili, are capable of producing infection, whereas types 3 and 4, which do not contain pili (now called P-colonies), fail to cause infection. The pili appear to facilitate attachment of gonococci to epithelial surfaces. Other gonococcal surface structures in addition to pili are also associated with pathogenesis.
BOX 5.2 ▪ GONORRHEA
Approximately 800,000 cases annually in U.S.
Rates of gonorrhea began increasing in 2005
Fluoroquinolone resistant N. gonorrhoeaenow widespread in U.S.
Fluoroquinolones no longer recommended for treatment of gonorrhea
Pathogenic neisseria have an extraordinary capability to vary their surface structures. Not only is this property used to protect the organism from the host immune response, but such variation also affects the function of factors that interact with host cells. As a result, the gonococcus can interact with epithelial cells or phagocytic cells, adhere to cells, invade cells, or remain protected from serum factors inside a capsule or sialylated lipopolysaccharide. These surface structures and functions are determined by proteins present in the outer membrane of the gonococcus, including porin protein (Por), an important cofactor in gonococcal invasion of epithelial mucosa cells, and opacity-associated proteins designated Opa (a family of proteins that promote cell adhesion), thus setting the stage for cell invasion, and reduction modifiable protein (RmP), which induces antibodies that block access of other antibodies, including IgM, to the gonococcal surface.
Additional gonococcal virulence factors include (i) lipopolysaccharide, which has endotoxin activity, causing cytotoxic effects on the epithelium of the fallopian tube and the systemic findings of fever and toxicity; (ii) IgA protease, which is present in all gonococci and destroys the secretory immunoglobulin IgA; and (iii) iron-repressible proteins that are involved in uptake of iron, an essential requirement for growth of gonococci.
As with other infections, the initial step in gonococcal infection is adherence of N. gonorrhoeae to mucosal cells lining the genitourinary tract. This process of adherence is mediated by pili and other surface proteins. This step is followed by a process of pinocytosis, by which the organism is transported into epithelial cells and then into submucosal tissues. Attachment of N. gonorrhoeae also results in the release of the endotoxin gonococcal lipopolysaccharide, which damages the ciliated and nonciliated cells of the fallopian tube epithelium.
Clinical Manifestations
The clinical presentation of infection with N. gonorrhoeae depends on the site of infection, duration of infection, and whether the infection remained localized or spread systemically. In women, infection is often asymptomatic (up to 80%), and the primary site of involvement is the endocervical canal and the transition zone of the cervix. However, it has become apparent that women with endocervical gonorrhea may be symptomatic and most commonly present with symptoms such as vaginal discharge, dysuria, and abnormal uterine bleeding. Urethral colonization occurs in the majority of women with endocervical gonorrhea, and infection of the periurethral (Skein’s) glands, Bartholin’s glands, and anorectum also occur.
FIGURE 5.2 Gonorrhea rates: Total by sex, United States, 1987-2006 and the healthy people 2010 target.
UNCOMPLICATED ANOGENITAL GONORRHEA IN FEMALES
Uncomplicated anogenital gonorrhea in women may involve the endocervix, urethra, Skein’s glands, Bartholin’s glands, and/or anus. The most commonly infected site is the endocervix. Gonococcal infection of the vagina is rare except in prepubertal and postmenopausal patients. Urethral colonization is present in 70% to 90% of women infected with N. gonorrhoeae. The rectum is infected in 35% to 50% of women with endocervical gonococcal infection and is the only site of infection in approximately 5% of women. If present, symptoms of anorectal gonorrhea range from mild pruritus and mucoid discharge to severe proctitis symptoms.
FIGURE 5.3 Gonorrhea rates by race/ethnicity: United States, 1997-2006.
At one time, uncomplicated anogenital gonorrhea in females was considered an asymptomatic disease. It is now recognized that although the majority of women harboring N. gonorrhoeae are asymptomatic, a large number of women (20% to 40%) with anogenital gonorrhea are symptomatic. Common symptoms include vaginal discharge, dysuria, intermenstrual bleeding, menorrhagia, and pelvic discomfort. In 15% to 20% of women with uncomplicated anogenital gonorrhea, upper genital tract infection (PID) occurs. Gonococcal-associated PID tends to occur at the end of or just after menstruation. A detailed description of PID and the role of N. gonorrhoeae in its etiology and pathogenesis are reviewed in Chapter 13.
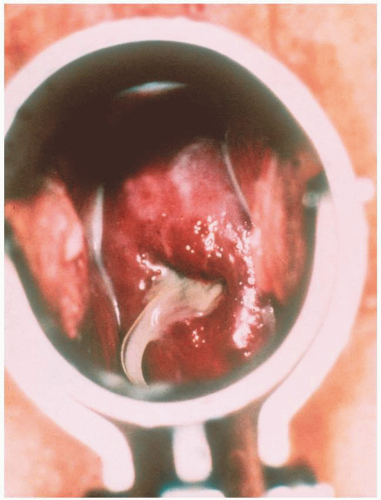
The cervix infected with N. gonorrhoeae can appear healthy or reveal an inflamed cervical canal with ectopy and a mucopurulent exudate (Fig. 5.4). The area of ectopy is edematous, erythematous, and friable. In general, these signs of gonococcal cervicitis are indistinguishable from other causes of cervicitis, and thus an absolute diagnosis of gonococcal cervicitis requires confirmatory laboratory tests. Gonococcal infection of the urethra, Skein’s glands, or Bartholin’s glands may be associated with mucopurulent exudate, which can be expressed from these structures.
Gonococcal infections in pregnant patients are most commonly asymptomatic. The two most common symptoms are vaginal discharge and dysuria. On examination, an endocervicitis may be present with erythema and a mucopurulent discharge. If routine screening for N. gonorrhoeae is not performed during pelvic examinations, the presence of lower genital tract complaints or signs such as abnormal bleeding, discharge, dysuria, mucopurulent endocervicitis, and/or pelvic discomfort should suggest that cultures be obtained to determine if the gonococcus is present.
NONGENITAL GONOCOCCAL SYNDROMES
Non-genital tract gonococcal disease may result from direct or contiguous spread and by bloodstream dissemination. Direct or contiguous spread occurs for pelvic inflammatory disease, anorectal infection, perihepatitis (Fitz-Hugh-Curtis syndrome), conjunctivitis, and pharyngeal gonococcal infection.
Although up to 10% to 20% of heterosexual women with urogenital gonorrhea have coexistent pharyngeal gonorrhea, the pharynx is the sole site in less than 5% of females. The majority of patients with pharyngeal gonorrhea are asymptomatic. In those with symptomatic infection, a mild sore throat and erythema are present. However, oral ulcerative lesions and exudates of the pharynx and tonsils may occur.
Rarely, N. gonorrhoeae causes conjunctivitis in adults. This usually is the result of direct sexual contact or indirect via contaminated hands, amniotic fluid at delivery, or accidental inoculation in the laboratory with clinical isolates. The typical presentation for gonococcal conjunctivitis is an acute onset of purulent conjunctivitis with extensive inflammation and copious purulent secretions.
Acute PID is a local complication of gonorrhea which is the most common complication of gonorrhea in women occurring in an estimated 10% to 20% of untreated cases. Bartholin’s gland abscess is the next most frequent complication of gonococcal infection in women.
DISSEMINATED GONOCOCCAL INFECTIONS
Disseminated gonococcal infection (DGI), the most common systemic complication of gonorrhea, occurs when gonococcal bacteremia produces extragenital manifestations of gonococcal infection. The prevalence of DGI among total gonorrhea cases ranges from 0.1% to 0.3%, with females predominating over men by about 4:1. The majority of women with DGI develop symptoms either during pregnancy, especially the third trimester, or within 7 days from the onset of menstruation. Only certain strains of N. gonorrhoeae have a predisposition to disseminate. In general, they are strains that are highly antibiotic-sensitive, resistant to bactericidal activity of human serum, and have a unique nutritional requirement for arginine, hypoxanthine, and uracil (i.e., ArgHyxUra auxotype). In addition, complement deficiencies have been demonstrated to be associated with an increased risk for DGI.
Patients are considered to have proven DGI if they have positive cultures from blood, joint fluid, skin lesions, or otherwise sterile sources. This group makes up less than 50% of DGI cases. Probable DGI is defined when N. gonorrhoeae can be cultured from the primary site in the lower genital tract or pharynx or in a sexual partner.
Disseminated gonococcal infection manifests two stages: an early bacteremia stage and a late stage (Table 5.4). The bacteremia stage is characterized by chills, fever, typical skin lesions, and asymmetric joint involvement. Blood cultures are positive for N. gonorrhoeae in half of the patients cultured during the bacteremia stage. The bacteremia stage is associated with a dermatitis that is characterized by a variety of skin lesions due to gonococcal emboli and occurs in 50% to 75% of cases (Fig. 5.5). These lesions appear initially as small vesicles that become pustules and develop a hemorrhagic base. The center becomes necrotic. These lesions occur on any body region but are most frequently present on the volar aspects of the upper extremities, the hands, and the digits. These skin lesions resolve spontaneously without residual scarring.
TABLE 5.4 ▪ CLINICAL MANIFESTATIONS OF DISSEMINATED GONOCOCCAL INFECTION
Early stage
Migratory arthritis
Tenosynovitis
Dermatitis
Late stage
Arthritis
Perihepatitis
Osteomyelitis
Pericarditis
Endocarditis
Meningitis
FIGURE 5.5 Disseminated gonococcal infection: Pustule with hemorrhagic base and necrotic center.
Joint symptoms are frequently present during the early stage, with arthritis developing in 30% to 40% of cases. Asymmetric joint involvement is the usual pattern, most often affecting the knee, elbow, wrist, ankle, and metacarpophalangeal joints. The arthritis is migratory (i.e., one joint heals as another becomes affected). In two thirds of patients, tenosynovitis is present. The most frequent sites are the dorsal tendons of the hands, wrists and ankles.
The late stage of disseminated gonococcal infection is characterized by frank arthritis with permanent joint damage, endocarditis, meningitis, pericarditis, osteomyelitis, and perihepatitis. With arthritis, the knees, ankles, and wrist joints are the sites most commonly involved. Since the introduction of penicillin, gonococcal endocarditis and meningitis have been rarely seen complications of DGI. It is estimated that gonococcal endocarditis occurs in 1% to 3% of patients with DGI. However, recognition of gonococcal endocarditis is crucial because there is rapidly progressive valvular damage, especially to the aortic valve. Typically, patients present with a febrile illness of several weeks’ duration in association with malaise, fatigue, and weight loss. Regurgitant murmurs are almost always present, with echocardiography demonstrating valvular vegetations and/or flail leaflets.
NEONATAL GONOCOCCAL OPHTHALMIA
Gonococcal ophthalmia neonatorum has been recognized since 1881. Prior to the introduction by Crede of silver nitrate prophylaxis, ophthalmia neonatorum occurred in approximately 10% of infants born in the United States. Introduction of eye prophylaxis resulted in a rapid reduction in this rate.
TABLE 5.5 ▪ IMPACT OF UNTREATED GONORRHEA ON PERINATAL OUTCOME Spontaneous Perinatal Abortion Mortality Prematurity PROM
Spontaneous Abortion
Perinatal Mortality
Prematurity
PROM
Sarrel & Pruett, n = 37
13 (35%)
3 (8%)
6 (17%)
8 (21%)
Amstey & Stedman, n = 222
24 (11%)
15 (8%)
49 (22%)
52 (26%)
Edwards, n = 19
−
2 (11%)
8 (42%)
8 (67%)
Handsfield, n = 12
−
−
8 (67%)
9 (75%)
Gonococcal conjunctivitis is the most common clinical manifestation of N. gonorrhoeae in the newborn. Most newborns who are infected with gonorrhea acquire it during passage through an infected cervical canal. Gonococcal ophthalmia usually is manifested within 4 days of birth, but incubation periods up to 21 days have been reported. A frank purulent conjunctivitis occurs which usually affects both eyes. Untreated gonococcal ophthalmia can rapidly progress to corneal ulceration, resulting in corneal scarring and blindness.
GONOCOCCAL INFECTION IN PREGNANCY AND THE NEONATE
Postabortal gonococcal endometritis and salpingitis are now well-recognized complications post pregnancy termination. Patients undergoing therapeutic abortion who have untreated endocervical gonorrhea are at increased risk for developing postabortion endometritis.
The effects of gonorrheal infection on both mother and fetus were not fully appreciated until 40 years ago. The amniotic infection syndrome is a manifestation of gonococcal infection in pregnancy. This entity presents with placental, fetal membrane, and umbilical cord inflammation, which occurs after PROM and is associated with a positive oral gastric aspirate for N. gonorrhoeae, leukocytosis, neonatal infection, and maternal fever. This syndrome is characterized by premature rupture of membranes, premature delivery, and a high infant morbidity and/or mortality.
Table 5.5 summarizes studies demonstrating an association between untreated maternal endocervical gonorrhea and perinatal complications, including an increased incidence of premature rupture of membranes, preterm delivery, chorioamnionitis, neonatal sepsis, and maternal postpartum sepsis. In addition, a higher incidence of intrauterine growth restriction has been observed in gravid women with gonococcal infection.
Although these investigations demonstrated the need to screen pregnant women (especially among populations at high risk for STD) for N. gonorrhoeae, the low incidence of gonorrhea in the general population resulted in a difference of opinion as to the need for routine screening of all prenatal patients for gonorrhea. Because almost all patients with gonococcal infection during pregnancy are asymptomatic, we recommended routine cultures for N. gonorrhoeae at the initial prenatal visit and repeat the culture early in the third trimester. Alternatively, in settings with a low prevalence of gonorrhea, screening may be limited to those patients deemed at high risk for gonococcal infection (e.g., multiple sex partners, other STDs, adolescents, previous gonorrhea or symptoms suggestive of gonorrhea). The introduction of DNA probes and nucleic acid amplification tests (NAATs) that screen for both N. gonorrhoeae and C. trachomatis concomitantly and the current recommendations for chlamydial screening have resulted in most prenatal patients also being screened for N. gonorrhoeae.
Diagnosis
The diagnosis of infection with N. gonorrhoeae requires sampling and identification of the organism at infected sites. The major site of primary infection in women is the endocervix. The anal canal, urethra, and pharyngeal cavity are important sites to consider, as well. Methods available include Gram stain, culture, nucleic acid hybridization tests, and NAATs.
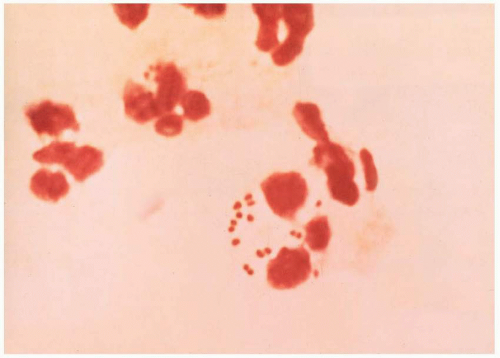
In men with urethral discharge and dysuria, the Gram stain of the urethral exudates is considered diagnostic for N. gonorrhoeae when Gram-negative diplococci are seen within or closely associated with polymorphonuclear leukocytes (Fig. 5.6). Unfortunately, microscopic examination of a Gram-stained specimen from the endocervix in women is not sufficient to detect gonococcal infection and is not recommended by the CDC. The same is true for pharyngeal or rectal specimens.
Therefore, in women, the diagnosis of N. gonorrhoeae infection requires specific testing for the organism. Because the majority of women with gonococcal infection are asymptomatic, screening of women at high risk for STDs is an essential component of gonorrhea control. Ideally, all sexually active women should be screened at every opportunity (i.e., annual routine pelvic examinations, presenting with gynecologic complaints). However, because of logistical and economic concerns, routine screening is not recommended in patient populations with low rates (<1%) of gonorrhea.
The U.S. Preventive Services Task Force (USPSTF) recommends that clinicians screen all sexually active women, including those who are pregnant, for gonorrhea infection if they are at increased risk. These include:
Women age <25 years
Previous gonorrhea infection
Other STDs
New or multiple sex partners
Partners of men with gonorrhea or urethritis
Inconsistent condom use
Commercial sex workers
Drug use
Women with symptoms or signs of lower genital tract infection
In addition, the CDC recommends that all patients treated for gonorrhea should be tested for other STDs, including chlamydia, syphilis, and HIV.
FIGURE 5.6 Gram-negative intracellular diplococci of Neisseria gonorrhoeae on Gram stain.
Screening for gonorrhea in pregnancy is cost-effective if the prevalence exceeds 1%. Thus, the CDC recommends that all pregnant women at risk for gonorrhea or living in an area where the prevalence of gonorrhea is high should be screened for N. gonorrhea at their first prenatal visit. At-risk pregnant women should be rescreened during the third trimester. In a recent study, approximately one third of women at risk for gonorrhea tested positive only on the repeat third trimester screen.
Culture for isolation is best performed using a selective media for N. gonorrhoeae, such as Thayer-Martin medium containing the antibiotics vancomycin, colistin, and nystatin, which inhibit the growth of contaminating organisms present in the same body sites as the gonococcus. The diagnosis of N. gonorrhoeae infection is made by identification of the organism with a typical growth on selective media, a positive oxidase reaction, and a Gram-negative diplococcal morphology on Gram stain of the isolated colonies. Fermentation reactions may be also performed. Although nonculture tests have to a large extent replaced culture as the primary approach for gonorrhea detection, culture remains important for monitoring antibiotic susceptibility patterns of N. gonorrhoeae.
Reliable nonculture assays for detection of gonorrhea have recently become available and have gained increasing acceptance as the result of their excellent sensitivity and specificity and extensive promotion by manufacturers and because specimens used by those assays for gonorrhea can also be used to test for C. trachomatis. These include nucleic acid hybridization tests such as nonamplified DNA probe tests (PACE 2 system by Gen-Probe) and NAATs. NAATs include polymerase chain reaction (PCR), ligase chain reaction (LCR), transcription-mediated amplification (TMA), and Strand-displacement assay (SDA). These newer technologies compare favorably to culture with selective media. Nucleic acid hybridization tests have sensitivities ranging from 89% to 97% and specificity of 99%. NAATs have both excellent sensitivity and specificity (>99%).
Nucleic acid hybridization tests require endocervical swab specimens. NAATs are FDA-cleared for use with endocervical swabs, vaginal swabs, and urine in women and thus provide the widest range of testing specimen types. Culture remains the best available option for diagnosis of infection with N. gonorrhoeae in nongenital sites.
The introduction of dual, single-swab NAATs and nucleic acid hybridization tests for detection of C. trachomatis and N. gonorrhoeae have simplified testing and facilitated expansion of STD screening. However, because the prevalence of gonorrhea is substantially lower than that of chlamydia, providers (especially in low-risk community settings) face potential false-positive results for N. gonorrhoeae because the positive predictive value of a test decreases as the prevalence of disease decreases. In addition, as these newer technologies replace culture, fewer isolates are available for antibiotic susceptibility testing. In cases of persistent gonococcal infection after treatment, the CDC recommends performance of culture and antimicrobial susceptibility testing.
Treatment
Uncomplicated Gonorrhea
The choice of antimicrobial agents for the treatment of gonococcal infection to a large extent reflects in vitro resistance patterns to N. gonorrhoeae. Additional factors that influence the choice of antimicrobial agents include maximizing compliance with single-dose (observed) therapy and the probability that patients infected with N. gonorrhoeae are coinfected with other STDs (especially C. trachomatis).
Initially, N. gonorrhoeae were sensitive to many antimicrobial agents including sulfonamides, penicillins, tetracyclines, macrolides, cephalosporins, erythromycin, aminoglycosides, aminocyclitols, and quinolones. Over time, increasingly resistant strains have appeared. By 1944, sulfamide resistance had become prevalent.
Once penicillin was available after World War II, it became the drug of choice for gonorrhea. Despite a progressive increase in resistance by N. gonorrhoeae, penicillins remained the therapy of choice by increasing the dose of penicillin and coadministering Probenecid. However, in 1976, strains of N. gonorrhoeae with high-level penicillin resistance due to plasmid-mediated production of β-lactamase were initially reported and by 1990 over 10% of N. gonorrhoeae strains were penicillinase-producing N. gonorrhoeae (PPNG).
In addition to the plasmid-mediated production of β-lactamase enzyme associated with PPNG, other resistant strains of N. gonorrhoeae have emerged in the United States. Gonococcal strains with high-level chromosomal resistance to penicillin (CMRNG) were first identified in 1983, and by 1987 the CMRNG form of resistance had become quite common. More recently, gonococcal isolates with plasmid-mediated, high-level resistance to tetracycline (TRNG) have been reported. The TRNG strains owe their resistance to acquisition of a tet M gene that codes for high-level tetracycline resistance. More recently, the emergence of fluoroquinolone resistance has been demonstrated. Quinolone-resistant N. gonorrhoeae (QRNG) have spread rapidly and have become increasingly common in the United States.
As a result, in 2006 the CDC recommended that quinolones should not be used for the treatment of gonorrhea in men having sex with men (MSM) and should not be used in California or Hawaii because of the high prevalence of QRNG in these areas. In April 2007, when ongoing data from the CDC’s Gonococcal Isolate Surveillance Project (GISP) demonstrated that fluoroquinolone-resistant gonorrhea continued to spread and was now widespread in the United States, fluoroquinolones were no longer recommended for treatment of gonorrhea in the U.S.
Updated guidelines for treatment of uncomplicated and complicated gonococcal disease were promulgated by the CDC in 2006. These guidelines were further updated in April 2007. The current CDC recommendation for the treatment of uncomplicated gonorrhea of the cervix, urethra, and rectum are provided in Table 5.6. Ceftriaxone is highly effective (>99% cure rates) and safe for the treatment of uncomplicated gonorrhea. However, it must be administered by injection. Cefixime’s efficacy is similar to ceftriaxone and has the advantage of oral administration. Among the alternative agents, spectinomycin also is not currently available in the United States. There is some evidence supporting the use of cefpodoxime 400 mg and cefuroxime axetil 1 g as alternative oral agents for the treatment of uncomplicated anogenital gonorrhea.
Limited data exist regarding alternative regimens for treating gonorrhea among persons who have documented severe cephalosporin allergy. Thus, expert infectious diseases consultation is recommended. The best available treatment option is cephalosporin treatment following desensitization. If this is not an option, azithromycin 2 g orally is effective against uncomplicated gonococcal infection, but concerns over gastrointestinal disturbances and emerging antimicrobial resistance to macrolides should restrict its use to special circumstances.
Concomitant infection with C. trachomatis is common in individuals infected with N. gonorrhea. Among women with gonorrhea, 20% to 30% are coinfected with chlamydia. Thus the CDC recommends that all women treated for gonorrhea should also be presumptively treated for chlamydial infection unless chlamydia has been ruled out with a NAAT. Azithromycin 1 g orally in a single dose or Doxycycline (100 mg orally bid for 7 days) are the preferred regimens in nonpregnant individuals, whereas in pregnancy, azithromycin or amoxicillin should be used (see Chapter 3).
TABLE 5.6 ▪ CENTERS FOR DISEASE CONTROL AND PREVENTION RECOMMENDED TREATMENT OF UNCOMPLICATED GONOCOCCAL INFECTION OF THE CERVIX, URETHRA, AND RECTUM (APRIL 2007)a
Recommended Regimens
Ceftriaxone 125 mg IM in a single dose
or
Cefixime 400 mg orally in a single dose or 400 mg by suspension (200 mg/5 mL) plus
Treatment for chlamydia if chlamydial infection is not ruled out
aThese regimens are recommended for adult and adolescent patients.
aSpectinomycin is currently not available in the United States.
bCeftizoxime 500 mg IM or cefoxitin 2 g IM administered with probenecid 1 g orally, or cefotaxime 500 mg IM
Persons treated for gonorrhea should be screened for syphilis. Regimens for treating gonorrhea that include ceftriaxone or a 7-day course of doxycycline or erythromycin probably cure incubating syphilis.
In pregnant or lactating women, N. gonorrhoeae should be treated with a recommended or alternative cephalosporin. In cases in which cephalosporins cannot be tolerated, Spectinomycin 2 g IM should be administered.
Test of cure is no longer recommended for individuals with uncomplicated gonorrhea who received any of the CDC-recommended regimens for uncomplicated gonorrhea. Persons with persistent symptoms should be recultured, and any N. gonorrhoeae recovered should be tested for antimicrobial susceptibility. Because patients infected with gonorrhea are at high risk for reinfection, repeat screening 1 to 2 months after treatment is appropriate.
In addition, it is important that sexual partners of patients with gonorrhea be examined, cultured, and treated (prior to culture results). Treatment should be with one of the CDC regimens for uncomplicated gonorrhea, preferably with treatment for coexistent chlamydial infection.
Complicated Gonorrhea
Treatment of complicated (upper genital or extragenital) gonococcal infection depends on the anatomic location, the severity of the disease, and the clinical response. Basically, the same antibiotics are used as for uncomplicated gonorrhea, but the doses are different.
Disseminated Gonorrhea
Ceftriaxone is the drug of choice for DGI. Patients allergic to penicillins and cephalosporins can be treated with Spectinomycin 2 g IM every 12 hours. The current CDC recommendations and alternate drugs are listed in Table 5.7.
Hospitalization is recommended for initial therapy of patients with DGI, especially those who are unreliable, have uncertain diagnosis, or have purulent synovial effusions, endocarditis, or meningitis. Whether pregnant patients with DGI should be hospitalized for bed rest and close observation for the occurrence of preterm labor or intrauterine infection has not been established. Until further information is available, our policy has been to treat pregnant women on an inpatient basis.
Meningitis and endocarditis caused by N. gonorrhoeae require high-dose intravenous treatment with ceftriaxone 1 to 2 g IV every 12 hours. Gonococcal meningitis should be treated for 10 to 14 days and endocarditis for 4 weeks. Treatment of complicated DGI should be undertaken in consultation with an expert.
Pharyngeal Gonorrhea
The recommended regimens for pharyngeal gonorrhea include ceftriaxone 125 mg IM as a single dose. Although chlamydial coinfection of the pharynx is rare, coinfection at genital sites may occur. Thus, concomitant treatment for chlamydia with azithromycin 1 g orally in a single dose or doxycycline 100 mg orally twice a day for 7 days is recommended unless chlamydia is ruled out with a NAAT. Gonococcal infection of the pharynx is more difficult to eradicate than ano-genital sites. Such patients should have repeat cultures at 4 to 7 days after treatment to document cure.
TABLE 5.7 ▪ CENTERS FOR DISEASE CONTROL TREATMENT RECOMMENDATIONS FOR DISSEMINATED GONOCOCCAL INFECTION (APRIL 2007)
Treatment should be continued for 24 to 48 hours after clinical improvement, at which time therapy may be switched to one of the following regimens to complete at least 1 week of therapy:
Cefixime 400 mg by suspension (200 mg/5 mL) twice daily
or
Cefpodoxime 400 mg orally twice daily
aTablet form of cefixime currently not available in the United States.
Gonococcal Pelvic Inflammatory Disease
Approximately 25% to 50% of patients with PID have gonococci isolated from their cervix. Treatment of PID is discussed in detail in Chapter 13.
Prevention
The increasing frequency of asymptomatic gonorrheal infection in women makes screening for N. gonorrhoeae during the antepartum period an important aspect of prevention of the perinatal morbidity associated with this organism. Additionally, aqueous solution or ophthalmic ointments containing erythromycin (0.5%) should be instilled into the conjunctiva of all newborns to protect against gonococcal conjunctivitis. The CDC recommends that infants born to mothers who have untreated gonorrhea are at high risk for infection and should receive prophylactic treatment with ceftriaxone 25 to 50 mg IV or IM, not to exceed 125 mg in a single dose. Most important to any prevention effort is the treatment of sexual contacts. Even those without symptoms must be treated if the cycle of infection is to be halted.
SYPHILIS
Syphilis is a chronic systemic infectious process due to the spirochete Treponema palladium. It is a strict anaerobic spirochete and obligate human parasite. The organism has never been grown in vitro in the laboratory. However, it can be grown in laboratory animals, especially rabbits. Because no in vitro system for culture of T. palladium is available, diagnostic efforts must rely on direct smears and/or serologic tests.
It has been recognized for several centuries that primary, secondary, or early latent syphilis in pregnant women caused infection of the fetus, with resultant stillbirths, premature births, congenital abnormalities, and active disease at birth. Because of this significant morbidity, great emphasis has been placed on routine screening of all pregnant women for the presence of syphilis.
Epidemiology
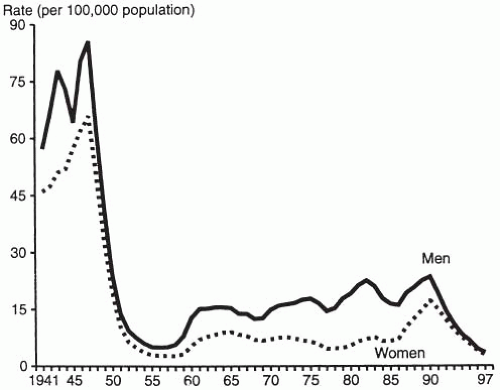
Following the startling prediction by the United States Surgeon General Thomas Parran in 1937 that 10% of Americans would be infected by syphilis during their lives, the incidence of primary and secondary syphilis (best indicator of incidence trends) rose during World War II, reaching a peak in 1947 of 76 cases in 100,000 population (Fig. 5.7). Following the introduction of penicillin, the incidence of primary and secondary syphilis fell dramatically, reaching a nadir of 4 cases in 100,000 by the late 1950s. Beginning in 1959, this trend reversed, with a rapid rise in incidence among men and women that reached a level of 12 in 100,000 by 1965 (3-fold increase). From 1965 through 1982 there was a steady but slow increase in the incidence of reported cases of primary and secondary syphilis that peaked in 1982 at 14.6 cases per 100,000 persons. Much of this increase was due to increased rates among MSM. From 1982 until 1985 there was a 22% decrease in reported cases of primary and secondary syphilis. In large part this decrease occurred among MSM, probably because of changes in sexual behavior as a result of the AIDS epidemic.
FIGURE 5.7 Trends in incidence of reported primary and secondary syphilis by gender, United States, 1941-1997. (From Aral SO, Holmes KK. Social and behavioral determinants of the epidemiology of STDs: industrialized and developing countries. In: Holmes KK, Sparling PF, Mardh P-A, et al, eds. Sexually transmitted diseases. New York: McGraw-Hill; 1999:39-76, with permission.)
Commencing in 1985, the United States experienced the most recent epidemic of syphilis. From 1985 to 1990, the incidence of primary and secondary syphilis rose sharply, reaching a peak in 1990 of 23.5 cases and 17.3 cases per 100,000 in men and women, respectively. Much of the increase occurred among African-American men and women. This increased spread of syphilis was linked to increased use of illicit drugs, especially “crack cocaine,” and high-risk sexual behavior associated with drug use. The rates of primary and secondary syphilis decreased throughout the 1990s and in 2000 reached an all time low (Fig. 5.8). As a result of the dramatic decline in syphilis rates, the CDC in 1999 launched the National Syphilis Elimination Plan. Unfortunately, this plan to eliminate syphilis from the United States was overly optimistic.
Since 2001, the syphilis rate in the United States has been increasing (Fig. 5.8) (Box 5.3). Between 2005 and 2006, the primary and secondary syphilis rate increased nearly 14%, from 2.9 to 3.3 cases per 100,000 population, and the number of cases increased from 8,724 to 9,756. The overall increase in syphilis rates has been driven primarily by increases among males. However, the rate among females increased in 2006 for the second year in a row, following a decade of declines. This increase among women was largely due to increased rates among African-American women. The reasons for these overall increases among females are not clear.
Only gold members can continue reading. Log In or Register to continue