Pelvic inflammatory disease (PID) is a spectrum of upper genital tract inflammatory disorders that includes any combination of endometritis, salpingitis, tubo-ovarian abscess, and pelvic peritonitis. In general, acute PID refers to infection of the upper genital tract attributed to ascending spread of microorganisms from the vagina and/or endocervix to the endometrium, fallopian tubes, and/or contiguous structures. In the past, the terms acute PID and acute salpingitis were often used interchangeably. In this chapter, the term acute PID will be used recognizing that acute salpingitis is the most important component of the PID spectrum.
PID is one of the most frequent and important infections seen in nonpregnant reproductive age women; it is associated with major clinical and public health problems, including diagnosis, treatment, prevention, sequelae, healthcare costs, and morbidity and mortality. Among women, acute PID is the most common important complication of sexually transmitted infections affecting millions of women worldwide. In the United States, more than one million women develop acute PID each year (Box 13.1). Women with acute PID are at risk to develop long-term sequelae including tubal factor infertility, ectopic pregnancy, and chronic pelvic pain. The annual cost of PID in the U.S. is estimated to be as high as $4 billion.
Recently subclinical PID has emerged as an important entity. A growing body of literature has demonstrated that subclinical PID is common among women with lower genital tract infections, especially Chlamydia trachomatis, Neisseria gonorrhoeae, and bacterial vaginosis (BV). Moreover, it is believed that subclinical PID is responsible for a greater proportion of PID related sequelae than acute PID.
EPIDEMIOLOGY
To prevent the significant medical complications and healthcare costs associated with PID, methods for accurate diagnosis, effective treatment, and prevention strategies must be developed. To accomplish this, clinicians must understand the epidemiology of PID, including the incidence/prevalence and risk factors for PID.
Unfortunately, precise figures on the incidence and prevalence of acute PID in the United States are not available. PID is not a reportable disease in many areas, and thus a variety of sources have been utilized to estimate these data, including patient surveys, hospital discharge rates, private physician office visits, emergency room visits, retrospective self-reporting, and extrapolations from incidence figures of gonorrhea and chlamydia. This situation is further complicated by the wide spectrum of clinical presentation and lack of accurate clinical diagnostic criteria associated with acute PID. In addition, it has been estimated that up to two thirds of cases of PID go unrecognized.
During the 1970s and 1980s, as a result of the STD epidemic and the widespread use of the intrauterine contraceptive device, the incidence of acute PID dramatically increased. In that era, approximately one million women were diagnosed annually with PID and the estimated yearly cost was $5.5 billion. A large part of this cost was attributed to long-term sequelae of PID, such as tubal factor infertility and ectopic pregnancy. In the 1980s, 250,000 to 300,000 women were hospitalized each year with a diagnosis of PID and over 1.2 million visits for PID to private physician offices occurred. In addition an estimated 150,000 surgical procedures were performed annually for complications of acute PID. During this time, an estimated 30% of acute PID cases were hospitalized.
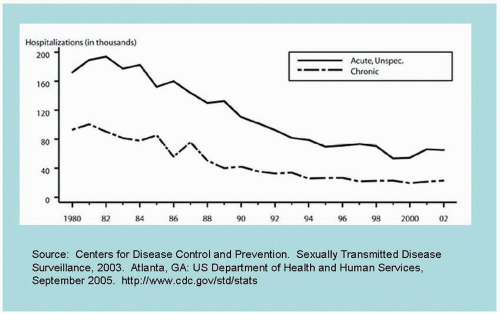
Since the peak in the early 1980s, hospitalization rates for acute PID have declined (Fig. 13.1). Whereas in 1981 there were an estimated 289,000 hospitalized cases of acute PID, in 1986 there were 114,000 and by 2001 only 28,000 women were treated as inpatients for acute PID. Since then the number of hospitalizations for acute PID plateaued.
During this period of time, the rates of PID declined from 14% of U.S. women 15-44 years of age in 1982 to 8% in 1995.
We recently reported that the hospitalization rate for PID in California had declined between 1991 and 2001 by 61.5% (2.6 to 1.0 per 10,000 women). Hospitalization rates for tuboovarian abscess declined by 33.3% during the same period (0.6 to 0.4 per 10,000 women).
While hospitalization rates for acute PID declined over this time, office-visit rates for PID remained relatively unchanged, with the number of new visits for PID diagnosed in physicians’ offices reported at 283,375 cases in 1981 and 285,000 cases in 1996. An additional 379,000 cases of PID on average were diagnosed annually in emergency rooms and outpatient clinics from 1992 to 1996. Thus approximately 780,000 cases of acute PID were being diagnosed annually in the U.S. during the 1990s.
Recently the CDC performed an analysis of the trends in incidence of PID among reproductive-aged women in hospital and ambulatory settings utilizing three nationally representative surveys conducted by the National Hospital Discharge Survey, National Hospital Ambulatory Medical Care Survey, and National Ambulatory Medical Care Survey. From 1985 through 2001 rates of hospitalized PID declined 68% overall from 4.4 to 1.4 per 1,000 women ages 15 to 44 years. Similarly, overall there was a 47% decrease in the estimated rates of PID cases diagnosed in physicians’ offices between 1985 and 2001. From 1995 to 2001, an annual average of nearly 90,000 hospitalizations for PID occurred. During the same period, overall an estimated 735,000 women aged 15 to 44 were diagnosed with PID in ambulatory settings in the United States annually, including 429,000 initial visits for PID in private physician offices and 258,000 emergency department visits for PID. From 1995 to 2001 only 11% of the total estimated cases of PID were hospitalized and 89% of cases were diagnosed in an ambulatory setting.
BOX 13.1 ▪ PELVIC INFLAMMATORY DISEASE
Among women, the most common important complication of STIs
Nearly 1 million cases per year in the United States
Dramatic decrease in hospitalizations for PID in past decade
Subclinical PID emerging as a common complication
Several suggestions have been put forth in an attempt to explain the apparent decrease in the number of cases of PID being seen in the United States. During the same time period there has been a parallel decrease in the incidence of gonorrhea and in some local areas there has been a decrease in chlamydial infection. This decline has been implicated in the decrease of estimated cases of PID. Similar trends have been seen in Sweden and Norway where hospital admissions for PID decreased in parallel to dramatic decreases in infections with C. trachomatis and N. gonorrhoeae. Of concern are the recent increases reported for N. gonorrhoeae and C. trachomatis infections reported in the U.S. by the CDC. It would not be surprising if this resurgence is accompanied by a future increase in the PID rate. Another factor may be the significant decline in the use of IUDs as a method of contraception in the United States in the 1980s and 1990s and an effort to increase use of barrier methods and oral contraceptives in high-risk, sexually active young age groups (age, 14-24years).
Two economic factors may also have played a role in producing an apparent but not true decline in the incidence of PID. The increasing penetration of managed care, especially closed staff Health Maintenance Organizations (HMOs), may have shifted patients from private physician offices that are surveyed to clinics that are not and have probably emphasized ambulatory treatment over hospitalization for PID. The second factor relates to the economics of the past decade with increasing poverty and lack of health insurance coverage resulting in lack of access to healthcare and increasing use of public sector clinics not included in national survey data.
Increasing attention has recently focused on what initially was called “silent” or “atypical” PID. This term was used for the condition where women with documented infertility secondary to tubal scarring and adhesions denied any past history of PID despite the fact that the scarring suggested that pelvic infection had previously occurred. Rather than a totally asymptomatic, silent infection, this “unrecognized” form of PID may present in an atypical clinical manner (e.g., intermenstrual bleeding, mucopurulent discharge) that is not recognized or diagnosed as PID. Thus we prefer the term subclinical PID. Subclinical PID is probably as common as, if not more common than, clinically apparent acute PID. However, no data are available elucidating the incidence or prevalence of this important entity.
FIGURE 13.1 Rates of hospitalization for PID among women aged 15 to 44 years: United States, 1980 to 2002.
Available studies suggest that 25% of women with chlamydial or gonococcal lower genital tract infection and 15% of those with BV have subclinical PID (as determined by endometrial biopsy) in the absence of the traditional symptoms and signs of acute PID. Thus, it has been suggested that as many, if not more, cases of subclinical PID occur annually as clinically apparent acute PID.
RISK FACTORS
Risk assessment is important in the diagnosing, management, and prevention of PID. Risk assessment is dependent on an understanding of known and suspected risk factors and/or risk markers. A risk factor is a variable that has a direct causal effect. On the other hand a risk marker has an indirect effect and may be a surrogate for a risk factor.
PID can result from several different microbiologic agents (see Section on Etiology). Although risk factors may vary according to the etiologic agent(s), the majority of PID is associated with sexually transmitted diseases (STDs). Table 13.1 provides a summary of risk factors associated with STD acquisition, development of PID and development of PID sequelae.
Initial studies assessing risk factors associated with PID focused on demographic and social indicators. More recently the important role of sexual behavior, contraceptive practice, healthcare behavior, and other individual behaviors and practices have been stressed (Table 13.1) (Box 13.2). In addition, women who have had previous PID are more likely to have recurrent infections. The exact mechanism for this increased susceptibility has not been delineated. Perhaps, as the result of previous acute salpingitis, the fallopian tube loses some of its natural protective mechanisms against microorganisms. Additional explanations include: women with gonococcal and/or chlamydial PID are more likely to be reexposed to these putative agents and that certain organisms such as C. trachomatis may remain as latent infection in the fallopian tube after clinical response.
Demographic Factors
Demographic and social indicators of risk that have been suggested as risk factors for PID include age, socioeconomic status, marital status, and rural or urban residence (Table 13.1). Age, an important risk marker for PID, is inversely related to PID rates. Thus adolescent females are at significant risk to develop acute salpingitis. In Westrom’s classic laparoscopy study, nearly 70%of females with acute salpingitis were younger than 25 years of age, 33% experienced their first infection before the age of 19, and 75% were nulliparous. The risk for developing acute pelvic inflammatory disease in the sexually active 15 year olds was 1:8, decreasing to 1:80 in females 24 years or older. Similar results have been reported in the U.S. with sexually active adolescent females three times more likely to be diagnosed with PID than 25- to 29-year-old women. It has been suggested that the adolescent population is at greater risk because this population has a high prevalence of sexually transmitted diseases, has multiple sexual partners, and tends not to use contraceptives—many of which (i.e., BCP, diaphragms, condoms) protect against the development of acute pelvic inflammatory disease. In addition, the postpubertal adolescent is relatively estrogen-dominant with a resultant cervical ectopy that provides a greater target for attachment of C. trachomatis and N. gonorrhoeae.
TABLE 13.1 ▪ RISK FACTORS ASSOCIATED WITH STD ACQUISITION, DEVELOPMENT OF PID, AND DEVELOPMENT OF PID SEQUELAE
Reproduced with permission from Padian NS, Washington AE. Risk factors for pelvic inflammatory disease and associated sequelae. In: Landers DV, Sweet RL, eds. Pelvic Inflammatory Disease. New York: Springer-Verlag; 1997:21-29.
Socioeconomic measures have been associated with increased risk for PID. These include (i) low levels of education; (ii) unemployment; and (iii) low income. While these appear to be markers for PID risk, this association may well be an artifact of the relationship between socioeconomic status and the prevalence of STDs and sexual and health behaviors. Marital status also has been associated with development of PID, with higher rates of PID in the never married category and the divorced or separated category.
BOX 13.2 ▪ RISK FACTORS FOR PID
Young age, especially sexually active adolescents
Low socioeconomic status
African-American race
Multiple sexual partners
Failure to use barrier methods of contraception
Douching
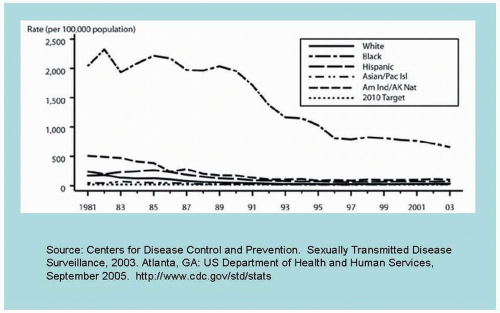
An association between race/ethnicity and STDs/PID has been well documented by the CDC, with African-American women in the highest risk group. This increased risk is to a large extent caused by the differential gonococcal and chlamydial rates among racial/ethnic groups (Fig. 13.2). Rates of gonorrhea and chlamydial infection are 30 times and 7 times higher respectively in African-American women than white women.
Behavioral Factors
Sexual Behavior/Sexual Practices
While STD organisms are clearly involved in the etiology of STD-related PID, the role of sexual behavior in the development of non-chlamydial, non-gonococcal PID remains poorly defined. In particular, studies have failed to differentiate between the role of sexual behavior as a risk factor for acquisition of STD-associated lower genital tract infection and the subsequent development of PID. However, several aspects of sexual behavior have been proposed to be associated with an increased risk of PID (Table 13.1). These include (i) multiple sex partners; (ii) high frequency of sexual intercourse; (iii) rate of acquisition of new sex partners within previous 30 days; and (iv) age at first sexual intercourse. Both multiple lifetime partners and multiple current partners have been reported to be risk factors for PID. In a case-control study of PID risk factors we identified >1 sex partner in the previous 30 days as a significant risk factor (odds ratio, 11.08; 95% CI, 4.31-28.50) whereas lifetime number of partners was not associated with an increased risk for PID. Similarly, women with subclinical PID have higher numbers of lifetime partners. Multiple sexual partners have also been associated with the long-term sequelae of PID. It is important to recognize that it is not the presence of multiple partners per se that produces an increased risk for PID, but the fact that multiple partners increases the risk of being exposed to STDs.
FIGURE 13.2 Rates of gonorrhea by race and ethnicity: United States 1981 to 2003.
Coitus during menses has also been suggested as a risk factor for PID. Among hospitalized patients with acute PID, analyzed in a case-control study, we reported that sexual intercourse with the last menses was a significant risk factor for PID (odds ratio, 5.22; 95% CI, 1.88-14.48). This increased risk is present for both STD-associated and non-STD-associated PID.
Contraceptive Use
Use of different contraceptive methods has a major impact on the risk of acquiring STDs, PID, and sequelae of PID such as tubal factor infertility or ectopic pregnancy. Multiple studies have demonstrated that women who use no contraceptive method are at increased risk for PID, probably because they are risk takers and do not utilize the healthcare system. In addition some forms of contraception protect against developing PID.
Barrier methods, when used properly and consistently decrease the risk of STD, PID, and sequelae of PID. Male condoms when used appropriately are highly effective in decreasing the risk of acquisition and transmission of STD organisms associated with PID (e.g., N. gonorrhoeae, C. trachomatis) as well as HIV. In addition, condom use has been reported to decrease the risk of developing PID. Similarly, condom use has been associated with decreased risk of tubal factor infertility and ectopic pregnancy. Recently in the PID Evaluation and Clinical Health (PEACH) study, persistent use of condoms has been shown to reduce the risk of recurrent PID, pelvic pain and infertility.
Diaphragm use has also been reported to decrease the risk for PID and tubal factor infertility. Previously it was believed that vaginal spermicides decreased the risk of acquiring STDs, especially N. gonorrhoeae, and C. trachomatis, and consequently decreased the risk of PID. However, more recent studies, including a Cochrane systematic review, demonstrated nonoxynol-9 does not protect against STD acquisition. Currently, research efforts have focused on the use of microbicides to prevent transmission of STDs and HIV. If demonstrated to be safe, acceptable, and effective, microbicides could play an important role in the prevention of STDs and thus PID and its sequelae.
The intrauterine device (IUD) is an additional predisposing factor. Controlled studies from the 1960s through the 1980s demonstrated a two- to fourfold increased risk of PID or sequelae of PID among users of IUDs compared with women using either no contraceptives or other methods. In particular, Dalkon Shield and Cooper-7 users were at excessive risk for PID and its sequelae. Several more recent investigations have suggested that the risk of PID among IUD users is low and primarily limited to the immediate (<20) days after the insertion period. Several factors may contribute to the increased risk of PID associated with IUDs. The IUD string, especially multifilament strings such as used in the Dalkon Shield, facilitates ascent of bacteria from the vagina and cervix to the upper genital tract. The presence of a foreign body in the uterus (as elsewhere in the body) may interfere with normal local host defense mechanisms. In addition, the associated role of multiple sexual partners and STD acquisition complicates assessment of the IUD role. Progesterone/progestin containing IUDs may reduce the rate of PID compared with copper and inert IUDs.
Most studies have shown that oral contraceptives (OCPs) reduce the risk for symptomatic, clinically apparent acute PID by 40% to 60%. In addition, OCP users have less severe damage to the fallopian tubes at laparoscopically diagnosed acute PID compared with women using IUDs or no contraception and a better prognosis for fertility. The mechanism for such protection remains speculative. Perhaps the effect of OCPs on cervical mucus precludes the ascension of vaginal and cervical microorganisms up into the upper genital tract. An additional explanation is that OCPs cause modifications of the immune response. Women using OCPs have a shorter duration of menses and less flow; this could result in a shorter “window” for microorganisms to gain access to the uterus and/or fallopian tubes. In addition, OCPs result in atrophy of the endometrium and decrease the uterine contractility thus decreasing the movement of bacteria from the vagina and cervix into the upper genital tract.
Healthcare Behavior
Healthcare-seeking behavior influences the risk of PID. Early detection and effective treatment of STD and PID in women and their sex partners will decrease the risk of PID and its sequelae. For example, routine screening for chlamydial infection had been shown to reduce PID by 60%. Delayed treatment of PID has a significant adverse effect on fertility. When treatment is delayed for three or more days the rate of impaired fertility increases 2.5-fold. Thus prompt evaluation, compliance with management instructions, and treatment of sex partners probably decrease the risk of PID and its sequelae.
Douching
Vaginal douching has recently been the focus of considerable interest and controversy as a potential risk factor for PID and PID associated sequelae. Both retrospective and cross-sectional studies have consistently demonstrated that women with PID report frequently douching more commonly than control women, even when gonococcal and chlamydial infections are controlled for. In the PEACH study, a large prospective study of over 800 women with mild-to-moderate PID, frequent and recent douching was associated with histologic endometritis or upper genital tract infection with N. gonorrhoeae or C. trachomatis. Additional investigations have demonstrated an association between douching and infertility and/or ectopic pregnancy. However, a recent large prospective observational study (GIFT) of nearly 1,200 women at high risk for chlamydial infection and followed for up to 4 years, failed to demonstrate an association between douching and development of PID among predominantly young African-American women.
While most but not all studies have suggested an association between douching and PID and sequelae of PID they do not prove causality. In favor of such a relationship is the consistency of the findings, the dose-response relationship seen with frequency of douching, the use of multivariate analysis controlling for confounding variables and the biologic plausibility. Regarding the latter, douching could result in pushing or flushing microorganisms from the vagina and cervix into the upper genital, thus increasing the risk for upper genital tract infection. Alternatively, douching may alter the vaginal microbial ecosystem resulting in colonization with organisms such as N. gonorrhoeae and C. trachomatis or predispose for development of bacterial vaginosis with subsequent increased risk for PID.
Additional Risk Factors
Additional risk factors that have been implicated as risk factors for PID include cigarette smoking, substance abuse, and menses. Women who are current cigarette smokers have a twofold increased risk of PID. Women who smoke have also been shown to be at increased risk for PID sequelae, including infertility and ectopic pregnancy. This relationship may be explained by the ability of cigarette smoking to alter cervical mucus and thus facilitate ascending infection. Alternatively, smoking may be a marker for high-risk behaviors.
A relationship between the symptomatic onset of acute PID and the menstrual period has long been noted. In particular, women with chlamydial and/or gonococcal PID are significantly more likely to develop symptoms within 7 days of the onset of menses. Additional studies have noted that alcohol and illicit drug use, particularly cocaine, are associated with PID. The latter may be a marker for other high-risk behaviors.
TABLE 13.2 ▪ RECOVERY OF MICROORGANISMS FROM THE UPPER GENITAL TRACT OF WOMEN WITH ACUTE PID
Similar to the link between chlamydial and gonococcal lower genital tract infections and PID, BV has also been implicated in an increased risk of PID—acute and subclinical. The role of BV in the pathogenesis of PID has been controversial and is discussed in detail in the section on etiology.
ETIOLOGY
Prevention of the significant medical and economic consequences linked with acute PID requires development of treatment and prevention plans that are based on an understanding of the microbiologic etiology and pathogenesis of acute PID. Unfortunately, our ability to determine the microbiologic etiology of acute PID has been complicated by several factors. These include (i) most studies rely on specimens obtained from the cervix (and less often vaginal) rather than the upper genital tract; (ii) majority of studies focused on sexually transmitted pathogens (e.g., C. trachomatis and/or N. gonorrhoeae); (iii) few studies assessed the role of viral agents (Herpes simplex virus or cytomegalovirus); and (iv) lack of validated and standardized criteria for the diagnosis of acute PID and subclinical PID.
Pelvic inflammatory disease is caused by ascension of microorganisms from the lower genital tract (cervix and vagina) into the upper genital tract. Whereas, until the 1970s PID was believed to be a monoetiologic infection caused by N. gonorrhoeae, it is now recognized that the etiology of PID is polymicrobic in nature and a wide variety of microorganisms have been recovered from the upper genital tract of women with acute PID (Table 13.2,Box 13.3). Among these organisms are N. gonorrhoeae, C. trachomatis, genital mycoplasmas, anaerobic and aerobic bacteria from the endogenous vaginal flora such as Prevotella species (P. bivia), black-pigmented Gram-negative anaerobic rods, Peptostreptococci sp, Gardnerella vaginalis, Escherichia coli, Haemophilus influenzae, and aerobic streptococci.
BOX 13.3 ▪ PID IS A POLYMICROBIAL DISEASE
N. gonorrhoeae
65%-75%
C. trachomatis
Mixed anaerobic and facultative bacteria – 25% to 35% (similar to BV-associated organisms)
In general, studies utilizing laparoscopy and/or endometrial aspirations to obtain specimens from the upper genital demonstrate that approximately two thirds of acute PID is associated with only N. gonorrhoeae and/or C. trachomatis and in about one third of PID only anaerobic and/or facultative bacteria are present. In addition, approximately half of the women with STD associated PID also have anaerobic and/or facultative bacterial recovered.
Recently, attention has focused on subclinical PID (formerly “silent” or “atypical”), a term initially used to characterize the situation in which women with documented tubal factor infertility have no history of being diagnosed or treated for PID despite chronic inflammatory residua being confirmed. Whether the same microorganisms are associated with unrecognized PID that are the putative agents for clinically apparent PID remains to be confirmed. Preliminary studies suggest that both of the STD organisms, N. gonorrhoeae and C. trachomatis, and the BV-associated microorganisms are also associated with subclinical PID.
NEISSERIA GONORRHOEAE
In the United States, nontuberculous acute PID was traditionally separated into gonococcal and nongonococcal disease. This division was based solely on the recovery of N. gonorrhoeae from the endocervix of patients with acute PID. Studies utilizing endocervical cultures implicated the gonococcus as the causative agent in 33% to 81% of the cases of acute PID. More recent studies in which specimens were obtained from the abdominal cavity and/or fallopian tubes demonstrate that while recovery of N. gonorrhoeae from the endocervix is frequent (up to 40%) this organism was only found in the abdominal cavity/fallopian tubes in 18% of total patients and 43% of patients with N. gonorrhoeae isolated from the cervix. Generally, in populations with high endemic rates of gonorrhea, a high proportion of acute PID is associated with N. gonorrhoeae. Thus, in many areas of the United States, N. gonorrhoeae has been recovered in 40% to 50% of acute PID cases. In areas such as Scandinavia where the incidence of gonorrhea has dramatically decreased, the proportion of PID cases associated with N. gonorrhea have also decreased.
Recently, the PEACH study (largest prospective cohort of acute PID in the United States) reported that among 274 patients with acute PID confirmed by histologic endometritis, N. gonorrhoeae was isolated in only 11 (4%) with a range of 3% to 13% among four sites (Pittsburgh, Birmingham, Charleston, and Providence).
CHLAMYDIA TRACHOMATIS
Chlamydia trachomatis has received considerable attention and is now firmly established as a major etiologic agent in acute PID. Studies in the Scandinavian countries were the first to demonstrate the important role of C. trachomatis in the etiology of acute PID. These studies reported the recovery of C. trachomatis from the cervix in 22% to 47% of women with acute PID. Of more significance, C. trachomatis was recovered from the fallopian tube(s) in 9% to 30% of women with laparoscopically confirmed acute PID. Scandinavian studies utilizing serologic surveillance suggested that C. trachomatis was associated with 23% to 62% of acute PID cases.
Initial microbiologic investigations in the United States failed to confirm that chlamydia was a major putative agent in acute PID, including our initial laparoscopy study where we failed to recover C. trachomatis from the fallopian tube exudates in 37 patients. However, serologic data obtained from studies in the United States showed a fourfold rise in chlamydial antibodies in approximately 20% of acute cases. The conflicting findings from Scandinavia and the United States were thought to be caused by several factors. In Sweden, specimens for chlamydial cultures were obtained via biopsy or needle aspiration of the fallopian tube; in the United States, studies had utilized cultures from peritoneal fluid and/or tubal exudates. C. trachomatis is an intracellular organism, and, thus, fresh infected cells, such as obtained via biopsy, may be necessary to recover the organism. Secondly, the patient population studied may be different; the Swedish investigators studied women with a milder disease than was usually admitted to hospitals and studied in the United States. In fact, it has been suggested that patients with milder pelvic inflammatory disease are more likely to have C. trachomatis as the causative agent. Paradoxically though, at laparoscopy, those women with C. trachomatis infection based on serologic data had the most severe fallopian tube involvement and the highest estimated erythrocyte sedimentation rates (ESR).
Most recent studies have demonstrated a definite role for C. trachomatis as an etiologic agent for acute PID in the United States (Table 13.3). These studies utilizing specimens obtained from the upper genital tract (endometrial cavity and/or fallopian tubes) provided direct evidence for the etiologic role of C. trachomatis in hospitalized women with acute PID. A summary of results from laparoscopy studies in Table 13.3 demonstrates recovery of C. trachomatis from the fallopian tubes/abdominal cavity in 40 (10%) of 363 patients with confirmed acute PID. In these studies, C. trachomatis was isolated from the fallopian tubes/abdominal cavity in 28 (41%) of 69 PID patients with chlamydial cervical infection.
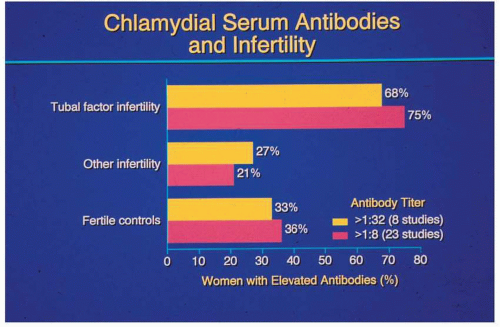
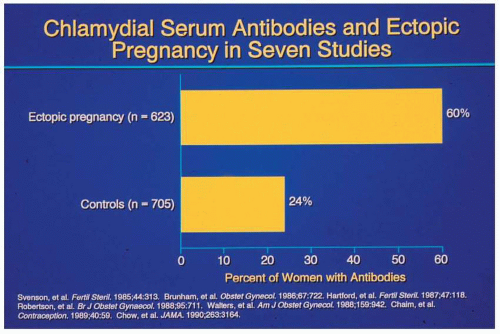
Additional epidemiologic data further suggest that chlamydia plays a role in infertility caused by tubal obstruction and salpingitis. These studies have demonstrated in a wide variety of populations and geographic areas that women with tubal factor infertility are significantly more likely to have had previous systemic chlamydial infection as documented serologically than pregnant controls or nontubal factor infertility patients (Fig. 13.3). A similar association with previous chlamydial infection and ectopic pregnancy has also been demonstrated (Fig. 13.4). Thus, the two major sequelae of acute PID, tubal infertility and ectopic pregnancy, have been associated with prior chlamydial infection. The finding that about one half of women with tubal factor infertility and serologic evidence of previous chlamydial infection had no history of being diagnosed or treated for acute PID has led to the concept of subclinical PID. Although very suggestive for a direct etiologic role in tubal infertility for C. trachomatis, these seroepidemiologic studies do not prove causation. However, recent investigations have provided a model for the pathogenesis of chlamydial salpingitis and its sequelae, which is discussed in depth below in the section on pathogenesis.
TABLE 13.3 ▪ UNITED STATES STUDIES DEMONSTRATING THE PUTATIVE ROLE OF CHLAMYDIA TRACHOMATISIN ACUTE PID
The genital tract mycoplasmas, M. hominis, U. urealyticum, and M. genitalium have been suggested as potential pathogens in the etiology of acute PID. However, their role remains controversial. Although M. hominis and U. urealyticum have been frequently recovered from the lower genital tract of women with PID, no difference exists between the rates of isolation from the cervices of these patients and sexually active control patients. Moreover, the genital tract mycoplasmas have been recovered infrequently from the peritoneal cavity and/or fallopian tubes of patients with salpingitis. In addition to the low recovery rate from the fallopian tube, in vitro studies with fallopian tube explant systems have suggested that mycoplasmas may be commensals rather than pathogens in acute PID as there was no apparent tubal damage produced.
FIGURE 13.3 Detection of anti-chlamydial IgG antibodies in patients with tubal factor infertility.
More recently, attention has focused on a third genital tract mycoplasma, Mycoplasma genitalium. While M. genitalium has been recovered from the cervix using polymerase chain reaction (PCR) amplification technology, no studies have been reported that demonstrate the presence of M. genitalium in tubal specimens from women with acute PID. Thus its role in acute PID remains undetermined.
FIGURE 13.4 Detection of anti-chlamydial IgG antibodies in patients with ectopic pregnancy.
OTHER SEXUALLY TRANSMITTED PATHOGENS
The etiologic role of viruses in acute PID has not been extensively studied. In particular, a potential role has been suggested for the viral agents—herpes simplex virus II and cytomegalovirus (CMV). Laparoscopy studies in the United States failed to demonstrate the presence of HSV in the cervices or fallopian tubes of patients with acute PID. Investigators in Finland reported the recovery of HSV from the cervix and/or the upper genital tract of a few women with laparoscopy confirmed acute PID. Recently, positive HSV-2 serology has been associated with histologic endometritis. CMV has been recovered from the cervices in women with acute PID. Recently, CMV has been found in the endometrium and fallopian tubes in a small number of women with acute PID. Trichomonas vaginalis has been rarely recovered from the pelvis in women with acute PID. A recent study from Pittsburgh notes T. vaginalis infection was associated with histologic evidence of acute endometritis. While interesting, these findings require confirmation and the role of viral agents and protozoa in acute PID awaits further investigation.
ANAEROBIC AND FACULTATIVE BACTERIA
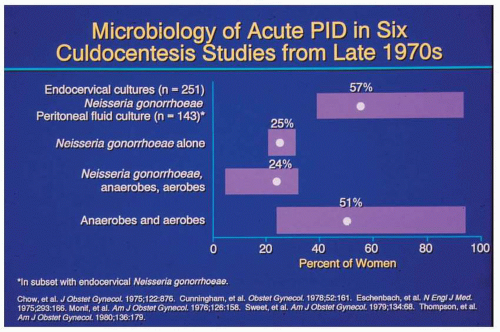
In the 1970s, it became apparent that the presence of pathogenic microorganisms in the endocervix was not absolute proof that such microorganisms are causally associated with upper genital tract infections such as PID. Investigations utilizing transvaginal culdocentesis to obtain culture specimens from the peritoneal fluid of women with acute PID demonstrated a poor correlation between the cervical and intraabdominal cultures (Fig. 13.5). A characteristic pattern evolved from these studies. While there was a high prevalence of N. gonorrhoeae in the cervix of these patients, only one fourth of the cases had N. gonorrhoeae as the only organism recovered from an intraabdominal site. An additional one fourth of the patients had a mixture of N. gonorrhoeae plus mixed anaerobic and aerobic bacteria (predominantly anaerobes). The final 50% of the patients did not have N. gonorrhoeae, but only a mixture of anaerobic and aerobic bacteria were recovered from the abdominal cavity. As a result of these studies it became recognized that the etiology of acute PID is polymicrobic in nature. While some investigators postulated that the gonococcus initiates acute PID and produces tissue damage and changes in the local environment, which in turn allow access to the upper genital tract for anaerobic and aerobic organisms from the vaginal and cervical flora, most have suggested that acute PID initially has a polymicrobial etiology. At the other extreme, it has been suggested that BV, an overgrowth of anaerobic and aerobic flora of the vagina, may predispose to or facilitate the ascent of N. gonorrhoeae into the upper genital tract.
FIGURE 13.5 Microbiologic isolates recovered via culdocentesis in patients with acute PID.
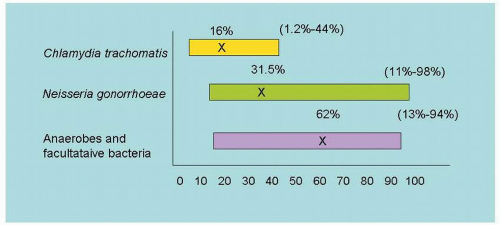
FIGURE 13.6 Recovery of microorganisms from the upper genital tract in acute PID.
However, subsequent studies utilizing laparoscopy to obtain specimens from the fallopian tube and cul-de-sac fluid demonstrated a discrepancy between culdocentesis and fallopian tube isolates from females with acute PID. Although close agreement between fallopian tube exudates and the cul-de-sac aspirate via laparoscopy was found, there was a poor correlation with the culdocentesis results, suggesting that contamination may occur during transvaginal culdocentesis.
The optimum microbiologic information for elucidating the etiology of acute PID would be obtained using specimens obtained directly from the site of infection—the fallopian tubes and/or endometrial cavity. In 1980, we reported our results from the first laparoscopy study of PID performed in the United States with cultures obtained directly from the fallopian tube. Subsequently, several other studies utilizing laparoscopy and/or endometrial aspirates to determine the microbiologic etiology of acute PID have been reported (Fig. 13.6). In summary, while C. trachomatis (16%) and N. gonorrhoeae (31.5%) were frequently recovered, mixed anaerobic and facultative bacteria (62%) were most commonly identified with anaerobic bacteria being the predominant isolates. The nongonococcal, non-chlamydial organisms identified in our studies are noted in Table 13.4. The most common included Prevotella (Bacteroides) species, Prevotella (Bacteroides) bivius, Prevotella (Bacteroides) disiens, Peptostreptococcus sp., Gardnerella vaginalis, group B streptococcus, and Escherichia coli. Most recently, our group demonstrated that in nearly one third of hospitalized cases of acute PID anaerobic and aerobic bacteria were the only organisms recovered from the upper genital tract (Fig. 13.7) and that among the two thirds of patients with N. gonorrhoeae and/or C. trachomatis isolated, 50% also had anaerobic and aerobes recovered. Thus anaerobes and aerobes were associated with two thirds of cases of acute PID. As noted in Figure 13.6, multiple studies from the United States and Scandinavia have yielded a similar pattern of etiologic agents with frequent recovery of anaerobes and facultative bacteria from the upper genital tract of women with acute PID. The more recent studies also identified black-pigmented anaerobic Gram-negative rods as a common pathogen in acute PID. Use of a broad-range 16S rDNA polymerase chain reaction to identify novel, possibly uncultivable bacteria has recently identified bacterial 16S sequences in fallopian tube specimens from 11 (24%) of 45 women with laparoscopically confirmed acute salpingitis. Many of these were anaerobic bacteria, including several associated with BV.
Only gold members can continue reading. Log In or Register to continue