Vulvovaginal burning, discharge, odor, itching, and dyspareunia, account for a considerable proportion of outpatient gynecologic visits. In many cases, the diagnosis is straightforward: candidiasis, bacterial vaginosis (BV) or trichomoniasis. Yet, many patients experience persistence or recurrence, and still others have less common diagnoses. Recent developments have included improved knowledge of the complications associated with vaginitis (upper genital tract infection and adverse pregnancy complications), new diagnostic techniques, new therapies, and preventions.
PREVALENCE AND DISTRIBUTION OF VAGINITIS
Vaginal symptoms occur commonly. Trichomoniasis, candidiasis, and BV account for the vast majority of cases, but especially in a referral practice, many cases cannot be accounted for by these three diagnoses. Further, many women with vaginal yeasts, Trichomonas vaginalis or Gardnerella vaginalis are asymptomatic.
GENERAL DIAGNOSTIC APPROACH TO INFECTIOUS VULVOVAGINITIS
Most cases of infectious vulvovaginitis can be diagnosed with a few inexpensive tests. In all cases, the physical examination should note the following: vulvar erythema; edema; excoriation or lesions; and color, amount, and consistency of the vaginal discharge. Normal vaginal secretions are heterogenous. Careful attention should be paid to the white epithelium (characteristic of a vulvar dystrophy) or to vulvar tenderness (characteristic of vulvodynia). The cervix should be examined for eversion, friability, and color and amount of mucus. For patients with vaginal discharge or irritation, the following tests are indicated:
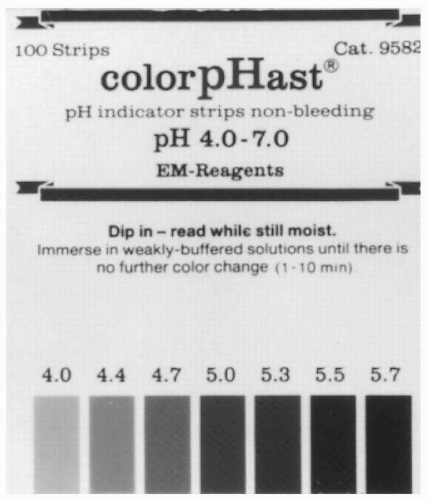
pH (using a paper that will distinguish pH values in the range from 4.0 to 5.0 (Fig. 11.1)
Amine (“fishy”) odor by adding a drop of discharge to a drop of 10% potassium hydroxide (KOH) solution
Saline preparation for true clue cells, trichomonads, parabasal cells and background bacteria (lactobacilli vs. mixed),
KOH preparation for hyphae and pseudomycelia of yeasts,
Culture for yeasts, if the other tests are nondiagnostic,
Saline preparation of an endocervical smear (to detect microscopic evidence of cervicitis)
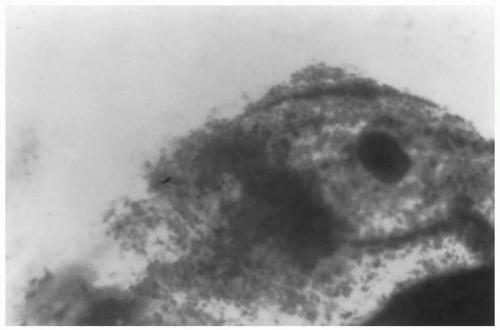
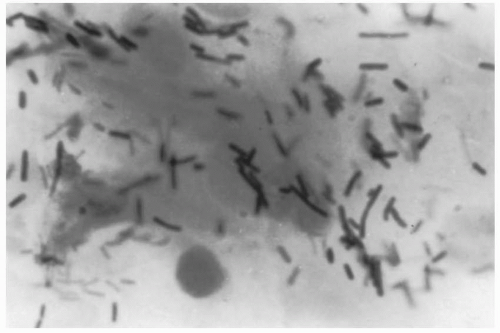
True “clue cells” (Fig. 11.2) are epithelial cells so heavily stippled with adherent bacteria as to obscure the cell margin. Normal epithelial cells commonly have some adherent bacteria (Fig. 11.3).
Culturing for G. vaginalis is wasteful. Although 95% of women with BV are positive (when selective media are used), so are 40% of women with normal secretions.
The Gram stain is helpful in diagnosing vaginitis, as the variety and numbers of bacteria can be readily identified, but this technique is cumbersome and is used primarily in research settings. Diagnostic criteria for common causes of vaginitis are given in Table 11.1. Approximately 8% to 10% of patients with abnormal vulvovaginal symptoms will not be diagnosed by the tests described. In these patients, cervicitis caused by gonorrhea or chlamydia should be excluded by specific testing. In addition, a saline preparation of an endocervical smear should be examined microscopically to detect microscopic evidence of cervicitis, which often is nongonococcal and nonchlamydial in origin. Because of the limited sensitivity of the wet mount for trichomonads (estimated at 50% to 80%), additional diagnostic tests have been developed. Media for culturing trichomoniasis are available commercially, as Diamond or Trichosel media or as the InPouch TV system (see section on trichomoniasis). Some women presenting with symptoms of vulvar burning and irritation, usually with dyspareunia, may be characterized as having vulvodynia (VVD) or, alternatively, vulvar vestibulitis. This condition, commonly called the “burning vulva syndrome” in the lay press, most likely is neuropathic rather than infectious in origin. It has a fairly characteristic presentation, marked by vulvar (rather than vaginal) symptoms, of greater than 3 to 6 months duration and point tenderness along the vaginal vestibule (elicited by pressure from a cotton tipped applicator). The physical appearance of the vulva is usually normal but there may be erythema in the vestibular glands at the 5 and 7 o’clock positions (i.e., posteriorly at the introitus, just to the right and left of the midline). Because the symptoms of VVD are often initially diagnosed as being caused by vulvovaginitis, vulvodynia is discussed briefly at the end of this chapter.
TRICHOMONIASIS
Trichomoniasis is caused by T. vaginalis, a protozoan first described in 1836. The organism has previously been reported to cause one fourth of all cases of clinically evident vaginal infections, but its prevalence appears to be decreasing lately. The prevalence of T. vaginalis ranges from 1% to 2% in middle-class women to 50% in women attending sexually transmitted disease (STD) clinics. Approximately 50% of women with T. vaginalis are asymptomatic, but about 30% of these asymptomatic women develop symptoms when they are observed for 6 months.
FIGURE 11.1 pH paper used in the differential diagnosis of vulvovaginitis. The pH range is from 4.0 to 7.0.
Among symptomatic women with trichomoniasis, the vaginal secretions usually are copious, homogeneous, and malodorous, with a pH above 4.5. A frothy, yellow-green discharge often is cited as the typical finding, but, in objective series, frothiness was detected in only one third or less. The color of the discharge is gray in about half of cases, and yellow-green in about a third. Punctate mucosal hemorrhages of the cervix, the so-called strawberry or “flea-bitten” cervix, are seen infrequently with the naked eye but are seen frequently with colposcopy. Because of the variations in signs and symptoms, one cannot rely on these findings solely to make a diagnosis.
Under most circumstances, the clinical diagnosis can be confirmed by microscopic examination of a wet mount, made by mixing a drop of secretions with saline on a slide. Because trichomoniasis may produce a heavy polymorphonuclear infiltrate, it is easy to miss the trichomonads. Examine the preparation in an area with relatively few white cells. Usually, the trichomonads are evident because of the motile activity of these flagellates in freshly made preparations. Overall, the sensitivity of clinical microscopy varies from as low as 42% to as high as 92%. When experienced technicians perform the test, the sensitivity runs at about 80%, compared with culture; when busy clinicians perform it, the sensitivity drops to about 50%. Most reports have found the sensitivity of culture to be greater than that of wet mounts.
FIGURE 11.2 Vaginal Gram stain showing a true clue cell and abnormal bacteria characteristic of bacterial vaginosis.
FIGURE 11.3 Gram stain showing normal vaginal flora with a predominance of Lactobacillus morphotypes.
Culturing currently is considered the best method for making the diagnosis. Culture for T. vaginalis is not difficult, but special media, such as Diamond or Kupferberg medium, is needed. A drop or swab of the vaginal secretions is placed in the broth, which is incubated. A drop of the media is examined daily under the microscope for 5 to 7 days for appearance of the motile trichomonads. Because there is limited demand for T. vaginalis cultures, few clinical laboratories have this available, even though the media are commercially available. In a comparison of a commercially available kit system (InPouch TV) to Diamond modified medium for culture of T. vaginalis from vaginal secretions, both culture techniques performed with similar high sensitivity.
The diagnosis of trichomoniasis by Papanicolaou (Pap) smear is unreliable. Its sensitivity is modest (52% to 67%). False-positive Pap smears are not uncommon as inflamed epithelial cells may be mistaken for trichomonads.
New diagnostic methods using monoclonal antibodies, enzyme-linked immunosorbent assay, and latex agglutination have been introduced. Although initial reports show encouraging results, there has not been much use in the clinical setting to determine the practical reliability of these. Several publications also have assessed a T. vaginalis polymerase chain reaction (PCR) test. Although these diagnostic tests each have used different PCR primers, each test has reported higher sensitivity with the PCR than with wet-mount microscopy, culture on Diamond or modified Kupferberg medium, or Pap smear. The PCR test also appears to be highly specific without interaction with other species of trichomonas other than T. vaginalis and without cross-reactivity with other human parasites or other human STDs such as Chlamydia trachomatis or Neisseria gonorrhoeae. The improved sensitivity of PCR appears to apply both to women without and women with symptoms of vaginal discharge. One additional advantage of the PCR test is that satisfactory specimens can be obtained by self-collection from the distal vagina, which eliminates the requirement for a vaginal speculum examination.
Urine sediment can be examined for trichomonads, and this is the preferred site for detection in males. The sediment can be cultured as well as inspected microscopically.
TABLE 11.1 ▪ CHARACTERISTICS OF NORMAL SECRETIONS AND COMMON CASES OF VAGINITIS
Feature
Normal
Bacterial Vaginosis
Trichomonas
Yeast
Appearance
White, floccular; gray, white, milky/creamy
Gray, yellow, greenish, white, often curdy
High viscosity or white; homogeneous, often frothy
pH
<4.5
>4.5
>4.5
<4.5
Amine odor
Absent
Present
Absent
Absent
Clue cells
Absent
Present
Absent
Absent
Trichomonads
Absent
Absent
Present
Absent
Mycelia
Absent
Absent
Absent
Present
The historic treatment for trichomoniasis available in the United States is metronidazole (Flagyl). Over the past 20 years, evidence has been strong that metronidazole is neither carcinogenic nor teratogenic. In a study of 1,387 women who filled prescriptions for metronidazole in pregnancy, there was no excess of overall birth defects (in their offspring), compared with 1,387 control women (risk ratio [RR], 1.2; 95% confidence interval [CI], 0.9 to 1.6). Also there was no excess risk in any category of birth defects.
Current CDC recommendations for treating trichomoniasis are provided in Table 11.2. For the first time, tinidazole is now provided as one of the recommended regimens. Cure rates with these regimens have varied from about 85% to 95%, and side effects (mainly nausea) have not been significantly different between the two regimens. The CDC guidelines recommend single-dose treatment as the regimen of choice.
Possible causes of failure of metronidazole therapy include:
problems in either absorption or delivery to the infected site,
inactivation of metronidazole by vaginal bacteria,
interference by other drugs,
resistance to metronidazole,
noncompliance or gastrointestinal intolerance, and
reinfection.
Over the last 20 years, strains of T. vaginalis with relative resistance to metronidazole have been common (see later). The CDC clearly recommends concurrent treatment of male partners of women with trichomoniasis.
Use of metronidazole occasionally is accompanied by headache, metallic or bitter aftertaste, or nausea and vomiting. Seizures and central nervous system toxicity can accompany metronidazole therapy, but almost exclusively in patients on exceedingly high doses (>3 g/day). Blood dyscrasias are rare consequences. Alcohol should be avoided during treatment and for 24 hours after completion of metronidazole and 72 hours after tinidazole. Metronidazole gel (0.75%) is available for treating BV. It should not be used for trichomoniasis because of poor efficacy.
Follow-up examination is not recommended for patients who become asymptomatic after treatment.
TABLE 11.2 ▪ RECOMMENDED REGIMENS FOR TRICHOMONIASIS
Metronidazole 2 g orally in a single dose
OR
Tinidazole 2 g orally in a single dose
Alternative Regimen for Trichomoniasis
Metronidazole 500 mg orally twice a day for 7 days
For treatment of trichomoniasis in pregnancy, metronidazole (FDA Category B drug for use in pregnancy) is recommended by the CDC in a single 2-g oral dose.
Symptomatic nonpregnant women with documented trichomoniasis should be treated to prevent sexual transmission and future symptomatic infection. Symptomatic pregnant women with trichomoniasis should be treated with 2 g of metronidazole in a single dose. The CDC guidelines no longer restrict use of metronidazole to the second or third trimester. For pregnant women with asymptomatic trichomoniasis, the decision to treat is a dilemma. There is some evidence linking this infection to adverse pregnancy outcomes (see later), and trichomoniasis is sexually transmitted. However, a treatment trial conducted by the National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Unit Network concluded that metronidazole treatment increased the risk of preterm birth in asymptomatic women with trichomoniasis. In this multicenter, double-blind, placebo-controlled trial, women who were culture positive for trichomoniasis were randomized at 16 to 23 weeks of gestation to receive either metronidazole or placebo. The metronidazole regimen was 2 g given under observation and another dose 48 hours later. Sexual partners of women in both groups were given prescriptions for metronidazole. The regimen was repeated at 24 to 29 weeks of gestation. The two groups, with approximately 300 women in each group, did not differ significantly in terms of demographic characteristics. However, total preterm birth was significantly greater in the group receiving metronidazole (19% vs. 10.7%; RR, 1.8; 95% CI, 1.19 to 2.66). There were significant increases in preterm births caused by preterm labor (10% vs. 3.5%; RR, 2.87; 95 CI, 1.43 to 5.75). There were no significant differences in preterm births caused by preterm premature rupture of the membranes (PROM), births at less than 32 weeks, birth weights less than 2,500 g, or birth weights less than 1,500 g. The risk of preterm birth in the metronidazole group was elevated among women with a prior preterm birth (RR, 1.93; 95 CI, 0.93 to 3.98; p > 0.05). In view of the results of this trial, treatment of asymptomatic women in pregnancy with trichomoniasis has not been recommended, but many experts in obstetric infections favor treatment of a asymptomatic pregnant women with trichomoniasis as it is an STD.
Tinidazole is a category C drug for use in pregnancy, and the 2006 STD guidelines conclude that its safety in pregnancy has not been established. For lactating women taking metronidazole, the guidelines recommend withholding breastfeeding during treatment for 12 to 24 hours after the last dose to reduce the exposure of the neonate. For women taking tinidazole, the recommendation is to withhold breastfeeding during treatment and for 3 days after the last dose.
Treatment for patients with human immunodeficiency virus (HIV) infection and trichomoniasis currently is the same as the treatment for patients without HIV.
When a patient has apparent persistence of T. vaginalis despite appropriate initial therapy, determine whether there has been compliance by both the patient and her sexual partner(s). Exclude interference by other medications such as phenytoin or phenobarbital, which induce microsomal liver enzymes and accelerate elimination of metronidazole.
If these problems are excluded, presumptive treatment for a relatively resistant strain is appropriate.
Approximately 80% of the women with these relatively resistant strains are ultimately cured with a higher dose of metronidazole. Oral doses greater than 3 g/day are accompanied by a high risk of serious side effects, including irreversible neurologic problems. Intravenous administration appeared to have no advantage.
The CDC recommendations for treatment failures are retreatment with metronidazole 500 mg twice daily for 7 days or tinidazole 2-g single dose. If repeated failure occurs, a single 2-g dose once daily of metronidazole or tinidazole for 3 to 5 days is recommended. See Table 11.3. For patients who still have persistent infection, the CDC recommendation is to exclude reinfection, evaluate in vitro susceptibility of the isolate, and manage “in consultation with an expert.” Consultation is available through the CDC. Our approach is shown in Table 11.3. We check a complete blood count before repeat high-dose treatment.
Patients who have severe vaginal trichomoniasis and serious adverse reactions to metronidazole have also been managed by desensitization. In a report of two patients, women were given incremental intravenous doses of metronidazole, beginning at 5 mg and building up to 125 mg stepwise at 15-to 20-minute intervals. Oral doses then were given up to 2 g orally. It is important to note that this desensitization approach was carried out after obtaining a documented history and a positive wheal test after application of metronidazole gel to the vaginal mucosa. The desensitization was performed in a monitored bed with additional precautions that included placement of two large intravenous lines and availability of a cardiopulmonary resuscitation team. In both cases, the desensitization was carried out without complications, and both patients were cured.
One report described resolution of resistant vaginal trichomoniasis when the patient used intravaginal nonoxynol-9.
Prevention of trichomoniasis is achieved by using safe sexual practices, which include limiting numbers of sexual partners, using condoms, and treating sexual partners.
Trichomonas vaginalis has not been linked, by itself, to genital tract cancer, infertility, abortion, or endometritis. However, as an STD, it should prompt detection of other STDs. Trichomoniasis has been linked to BV, which has been associated with several obstetric and gynecologic complications (see later). Trichomoniasis has been associated with adverse pregnancy outcomes, such as PROM and premature birth.
TABLE 11.3 ▪ AN APPROACH TO TREATMENT OF PERSISTENT TRICHOMONIASIS AFTER A SINGLE 2-G DOSE OF METRONIDAZOLE
Metronidazole 500 mg twice daily for 7 days or tinidazole 2 g orally
If this fails, give metronidazole or tinidazole 2 g orally for 5 days.
If these are not effective, then discuss with a consultant. The CDC is available at 770-488-4115 or http://www.cdc.gov/std.
4. Other regimens that may be effective include topical paromomycin 6.25% in a cream base, 4 g nightly for 14 nights.
Adapted from 2006 STD Guidelines.
YEAST INFECTION
Yeasts are commonly isolated in the female lower genital tract, with rates of about 20% among asymptomatic college women, 25% among patients in an STD clinic, and 40% among women with vulvovaginal symptoms. It is estimated that 75% of women will have at least one episode of yeast vulvovaginitis, with 4% to 45% having two or more episodes. In all studies, Candida albicans is the most common yeast isolate (in approximately 90% of cases), with Candida glabrata and other Candida species making up the remainder.
Commonly noted predisposing features to isolation of yeast in the vagina are glycosuria, diabetes mellitus, pregnancy, obesity, and recent use of antibiotics, steroids, or immunosuppression. Pregnancy is associated with an increased vaginal carriage rate, increased susceptibility to infection, and lower cure rates. Antibiotics that most commonly result in yeast colonization are ampicillin, tetracycline, and cephalosporins. Presumably, antibiotics suppress normal bacterial population and allow opportunistic colonization by yeasts. Prophylactic antifungal agents are an appropriate measure in patients susceptible to yeast infections when they require antibiotics for other infections.
Yeasts usually are not acquired through sexual intercourse. Evidence supporting sexual transmission in yeast vulvovaginitis includes
a fourfold increase in yeast colonization in male partners of infected women
isolation of the same strains in infected couples.
However, epidemiologic evidence against sexual transmission includes
no direct association between yeast infection and other STDs,
no difference in yeast isolation rates in STD versus non-STD populations,
and absence of any study showing that treatment of the male partner benefits the female.
Routine treatment of sexual partners is not recommended, but may be considered for women with recurrent infection. These recommendations suggest treatment of male partners who have balanitis, as evidenced by erythematous areas of the glans with local pruritus or irritation. Topical treatment to relieve symptoms is recommended in such cases. Despite much anecdotal information, purported risk factors, including wiping from back to front after using the toilet, use of feminine hygiene products, type of clothing, diet, and stress, showed no association with vulvovaginal candidiasis among college women.
The characteristic findings of vaginal candidiasis are reddened vulval or vaginal areas with vulval scaling, edema, or excoriation, and raised, white, or yellow adherent vaginal plaques. However such findings occur in a minority of women with positive cultures for C. albicans.
The diagnosis can be confirmed by observing mycelia and/or pseudohyphae on direct microscopy in a 10% KOH preparation, but this is a test with limited sensitivity (50% to 80%).
In view of the limited sensitivity of the KOH preparation and emergence of non-albicans species, we obtain a culture for yeast from vulvovaginal secretions in the following circumstances:
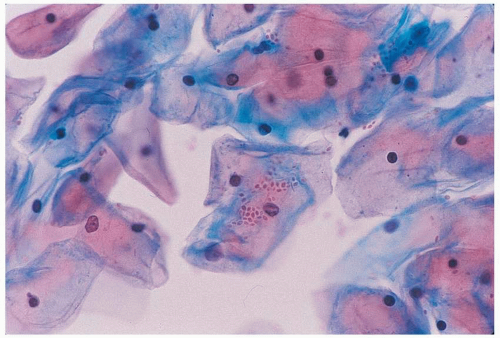
FIGURE 11.4Candida glabrata. As seen on a Papanicolaou smear. Buds are seen without pseudohyphae. This finding suggests non-Candida albicans species.
Yeast is suspected clinically but KOH preparation is negative
Poor response to therapy
A non-albicans species is suspected based on microscopy. (see Fig.11.4)
Specific communication should be sent to the laboratory that you are interested in detecting yeast so that selective media (such as Saborauds) will be used.
A vaginal yeast culture may reveal that the infecting species is a non-C. albicans variety. The most common of these species is Candida (formerly Torulopsis) glabrata. Some other species occasionally isolated include C. tropicalis and Saccharomyces cerevisiae. Infection with non-C. albicans species are often more difficult to treat and more likely to recur. The important point is that many of these species do not respond to usual oral or topical treatments.
The vaginal pH of women with yeast vulvovaginitis is normal (<4.5) (Table 11.1).
Rapid diagnostic techniques using technologies such as latex agglutination appear promising, but these tests have not been used widely in the clinical setting.
Only gold members can continue reading. Log In or Register to continue