Infection that occurs during pregnancy involves maternal, intrauterine (amniotic fluid, membranes, placenta, decidua), and fetal tissue. These infections are a major cause of both maternal and fetal/neonatal morbidity and mortality.
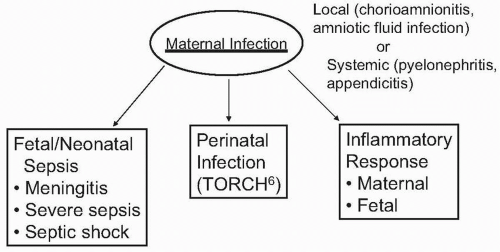
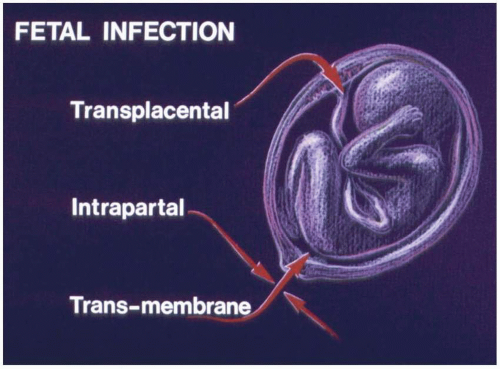
Conceptually, as shown in Figure 19.1, maternal infection may lead to a wide spectrum of infection and inflammation in the fetus and/or newborn infant. Perinatal and congenital infections are transmitted from mother to fetus or newborn transplacentally, transmembranous (ascending infection) or vertically during the process of labor and delivery (Fig. 19.2). The spectrum of perinatal infections has expanded dramatically from the original focus on the TORCH complex (Toxoplasmosis, Other, Rubella, Cytomegalovirus and Herpes simplex virus) (Table 19.1). Recently, Ledger suggested that this diverse group of microorganisms be called TORCH6 with HIV, human parvovirus B19, hepatitis B, hepatitis C, and human papillomavirus added to herpes simplex virus for “H6.”
These congenital and perinatal infections may be symptomatic with clinical signs of infection present in-utero or in the newborn. Many are asymptomatic at birth but manifest sequelae later in life including development delay, cerebral palsy (CP), sensorineural hearing loss, and learning disabilities. These infections are discussed in detail in Chapter 15.
Chorioamnionitis, clinical (intra-amniotic infection) and/or histologic, an important intrauterine maternal infection, is the major source of fetal/neonatal sepsis. Chapter 17 provides a detailed description of intra-amniotic infection. In turn, sepsis may progress to severe sepsis or septic shock (with hypotension and hypoperfusion) or meningitis, which may directly produce brain damage. Whereas complications of intra-amniotic infection were limited previously to maternal sepsis, neonatal pneumonia, neonatal sepsis, neonatal meningitis, and neonatal death, recently our understanding of these complications has expanded to include periventricular leukomalacia (PVL), CP, respiratory distress syndrome, bronchopulmonary dysplasia and necrotizing enterocolitis.
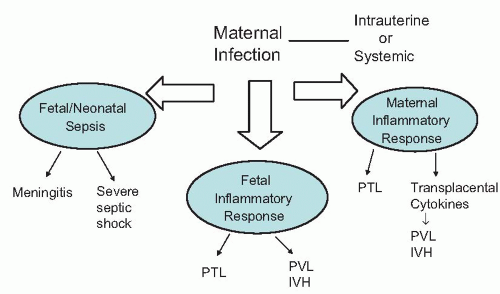
Infection has been demonstrated to be an important cause of preterm delivery and recently has been shown to rank high among antenatal risk factors for development of adverse neurologic outcomes in preterm and term infants (Fig. 19.3).
Of special concern has been CP, which comprises a group of nonprogressive motor impairment syndromes characterized by aberrant control of movement or posture that appears early in life and is caused by lesions of the brain arising early in development. CP can result in costly lifelong disability. In addition, seizures, cognitive impairment, and extra pyramidal abnormalities may occur. CP occurs in 1 to 2.4 per 1,000 live births. CP is the most common neuromotor developmental disability of childhood affecting 8,000 to 12,000 children born in the United States each year. Preterm infants are particularly at risk for CP. However, over half of all CP cases occur in children born at term. Several population-based studies have demonstrated that despite substantial advancements in both obstetric and neonatal care, the prevalence of CP has remained relatively constant over the past 40 years.
In 1862, William John Little initially suggested a link between cerebral palsy and perinatal events. Until recently intrapartum hypoxia/hypoxemia was considered the major risk factor for CP. This concept has been questioned and conflicting views have been advocated. Epidemiologic studies, including analysis of data from the Collaborative Perinatal Project in the United States in the 1950s and from Western Australia suggest that only 10% to 30% of CP is caused by intrapartum hypoxia/hypoxemia and that the majority are the result of antepartum events. Major risk factors identified in these studies included multiple gestation, prematurity, low birth weight, intrauterine infection, maternal pyrexia, and thrombophilia. On the other hand, recent studies employing modern imaging (MRI) of the neonatal brain shortly after delivery suggest that up to 90% of CP is due to acute intrapartum events.
Interestingly, the initial references suggesting that inflammation may cause CP appear in Sigmund Freud’s book “Infantile Cerebral Paralysis.” Over 50 years ago, Eastman and DeLeon reported a sevenfold increase in CP among the infants of mothers with fever during labor. This finding was largely ignored until the mid 1980s, when reports that analyzed data from the Collaborative Perinatal Project suggested that intrauterine infection/inflammation plays a role in the development of CP and served to focus considerable subsequent research on the hypothesis that intrauterine exposure to maternal or placental infection was associated with an increased risk for periventricular leukomalacia (PVL) and CP. Similarly, a 1998 study from Western Australia, assessing risk factors for newborn encephalopathy, reported an adjusted odds ratio (OR) of 3.82 (95% confidence interval [CI], 0.44 to 10.12) for maternal pyrexia intrapartum.
During the past two decades, a substantial body of investigative work has evolved assessing the role played by maternal and intrauterine infection as a cause of white matter damage (WMD) in the brain, PVL, and CP. This body of evidence is summarized in Table 19.2 and discussed in the following sections.
FIGURE 19.1 Spectrum of maternal infections as a cause of neonatal brain damage.
FIGURE 19.2 Routes for transmission of maternal infection to fetus or neonate.
TABLE 19.1 ▪ MICROBIAL AGENTS THAT RESULT IN CONGENITAL AND PERINATAL INFECTIONS INVOLVING THE CENTRAL NERVOUS SYSTEM
Bacteria
Group B streptococcus
Viridans streptococcus
Clostridium sp.
Group A streptococcus
Staphylococcus aureus
Anaerobic streptococcus
Enterococcus
Listeria monocytogenes
Bacteroides fragilis
Escherichia coli
Citrobactea sp.
Treponema pallidum
Klebsiella sp.
Salmonella sp.
Borrelia burgdorfei
Proteus sp.
Pseudomonas
Mycobacterium tuberculosis
Viruses
Mycoplasmas
Herpes simplex virus
Varizella zoster virus
Ureaplasma urealyticum
Cytomegalovirus
Rubella
Mycoplasma hominis
Human immunodeficiency virus
Human parvovirus B19
Enteroviruses
West Nile virus
Rubeola
Mumps virus
Hepatitis B
Human papillomavirus
Hepatitis C
Protozoa
Fungi
Toxoplasmosis gondii
Candida sp.
Plasmodium sp.
Aspergillus
Crytococcus
Coccidiodes immitii
FIGURE 19.3 Infection and brain damage.
CHORIOAMNIONITIS AND CEREBRAL PALSY
In 1978, Nelson and Ellenberg demonstrated that the risk for CP increased from 12 per 1,000 to 39 per 1,000 live births among infants <2,500g born to mothers with chorioamnionitis. Subsequently, multiple other investigators reported a significant relationship between chorioamnionitis and CP among preterm infants. Similarly, several studies demonstrated a significant link between chorioamnionitis and cystic PVL, a powerful predictor of CP in preterm infants. Maternal infection has also been implicated as a risk factor for CP in term births, although the data are more limited.
A recent meta-analysis assessed chorioamnionitis as a risk factor for CP. Among premature infants, 19 studies were analyzed and demonstrated that clinical chorioamnionitis was significantly associated with both CP and cystic PVL (Table 19.3). Overall, chorioamnionitis (clinical or histologic) was significantly associated with CP (risk ratio [RR], 1.8 [95% CI, 1.5 to 2.3]). Detailed analysis of these studies may be found at the Web site.
Among full term infants, studies of clinical chorioamnionitis and cerebral palsy yielded a summary relative risk of 4.6 (95% CI, 1.3 to 16.2). Only a single study examined the association between histologic chorioamnionitis and cerebral palsy in full term infants and found a relative risk of 8.9 (95% CI, 1.9 to 4.0).
TABLE 19.2 ▪ EVIDENCE SUPPORTING A ROLE FOR MATERNAL AND INTRAUTERINE INFECTION IN CEREBRAL PALSY
Epidemiologic studies noting association of infection and CP in preterm and term infants
Proinflammatory cytokines are increased in amniotic fluid, umbilical cord blood, and newborn blood of infants with PVL and CP
Histologic (and clinical) chorioamnionitis more common in newborns with PVL and CP
Immunohistochemical studies documented presence proinflammatory cytokines in brain tissue in newborns who died and had PVL
Inflammation activates microglial cells in the developing brain with resultant secretion of proinflammatory cytokines (IL-1β and TNF-α) and toxic molecules (NO, reactive oxygen species, and quinolinic acid) that damage adjacent neurons and glia and induce apoptotic or necrotic cell death through excitotoxicity and lipid peroxidation
FIRS plays a critical role in the pathogenesis of neonatal brain damage
Genetic susceptibility and gene polymorphisms which result in excessive production of cytokines are associated with increased risk for PVL and CP
Most recently, in a case-control study nested within a cohort of 231,582 term or near term singleton infants (≥36 weeks’ gestation) in the Kaiser Permanente Medical Care Program of northern California, a diagnosis of chorioamnionitis was noted in 14% of cases of CP compared with 4% of controls (OR, 3.8; 95% CI, 1.5 to 10). In a multiple logistic regression analysis, chorioamnionitis remained an independent risk factor for CP (OR, 4.1; 95% CI, 1.6 to 10.1). Strengths of this study included (i) inclusion of moderate-severe spastic or dyskinetic CP not due to post natal brain injury or developmental abnormalities; (ii) Hemiparesis and quadriparesis present in 40% and 38%, respectively; and (iii) MRI or computer tomography (CT) of the head was performed in 83% of children with CP.
Unexpectedly, the OR of chorioamnionitis for CP was higher among children with neuroimaging diagnosis of hypoxic-ischemic brain injury than among those with other neuroimaging findings (univariate OR, 17.2 [95% CI, 3.3 to 88] vs. 3.2 [95% CI, 1.2 to 8.1]; p = .04). In a multivariate analysis, the adjusted OR of chorioamnionitis for CP was particularly high among children with quadriplegic CP (OR, 9.7; 95% CI, 3.4 to 27.8) and among those with neuroimaging findings of hypoxic-ischemic brain injury (OR, 17.5; 95% CI, 3.3 to 93.4). The strong association found between chorioamnionitis and CP among children who sustained hypoxic-ischemic brain injury supports the hypothesis that chorioamnionitis plays a role in either initiating or exacerbating brain injury from hypoxia-ischemia (see section: Inflammation Increases Susceptibility to Hypoxia-Ischemic Injury).
TABLE 19.3 ▪ CHORIOAMNIONITIS AND CP IN PREMATURE INFANTSa
PVL is a developmental lesion of the cerebral white matter characterized by foci of necrosis in the white matter adjacent to the lateral ventricles. PVL is an antecedent to CP, especially of the spastic diplogia type with a peak incidence in premature infants. Potential etiologic mechanisms for PVL include ischemia-reperfusion and release of cytotoxic cytokines during infection, ischemia or other insults. These are not mutually exclusive pathogenic mechanisms. In addition, a complex interaction of vascular factors (e.g., vascular border and end zones, disturbances of cerebral autoregulation) and coagulation processes predispose periventricular white matter to injury.
PVL develops secondary to the loss of oligodendrocytes (OL) and particularly OL precursors in the periventricular white matter. Loss of the OLs results in the disrupted myelination which is the hallmark of PVL and its sequelae (i.e., CP). In vitro studies have demonstrated (in tissue culture) that OL precursors are particularly vulnerable to free radical-mediated injury, including glutamate-uptake-mediated toxicity, intracellular depletion of glutathione, and generation of intracellular oxygen radicals.
In addition, systems extrinsic to the OL contribute to the pathogenesis of PVL. The ability of endotoxin to experimentally induce white matter injury suggests a role for cell mediators. Two additional observations support this concept: (i) the presence of significant increases in reactive cell types—initially macrophages (microglia) and later reactive astrocytes at sites of WMD; and (ii) identification of cytokines with toxic or trophic effects on OL survival in tissue culture.
TABLE 19.4 ▪ INFECTION AND DEVELOPMENT OF PERIVENTRICULAR LEUKOMALACIA
Significant predictors of PVL. OR, 6.6 for prolonged PROM and 6.8 for chorioamnionitis
Alexander et al
Clinical chorioamnionitis
VLBW (500-1,500 g)
Independent risk factor for PVL (OR, 3.4; 95% CI, 1.6-7.3)
Wu and Colford
Clinical chorioamnionitis
Preterm neonates
↑ risk cystic PVL (RR, 3.0; 95% CI, 2.2-4.0)
Histologic chorioamnionitis
Preterm neonates
↑ risk cystic PVL (RR, 2.1; 95% CI, 1.5-2.9)
Until recently, ischemia was believed to be the predominant cause of PVL. More recent data suggest that infection plays an important role in the genesis of PVL. Over 30 years ago, initial support for the role played by infection came from the observation that neonates with documented sepsis were at increased risk for PVL. Shortly thereafter, injection of endotoxin into newborn kittens produced white matter brain lesions, similar to those seen in PVL. Similarly, in a rabbit model, intrauterine infection produced white matter damage.
Only gold members can continue reading. Log In or Register to continue