Acute viral hepatitis is a self-limiting infection that predominantly affects the liver, resulting in a necroinflammatory response. Formerly, acute hepatitis was divided into two types based on clinical and epidemiologic characteristics: type A or infectious hepatitis and type B or serum hepatitis. Currently, five distinct hepatotropic viruses have been identified: hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis D virus (HDV), and hepatitis E virus (HEV). Several viruses (hepatitis G virus or GBV-C and SEN viruses) were initially thought to cause posttransfusion hepatitis but are now not believed to be human pathogens.
HAV and HEV generally cause self-limited infections; on occasion fulminant hepatitis occurs (1% to 2% of infections). While HDV, the delta agent, produces coinfection in HBV infected individuals, it does not cause serious infection by itself. HBV and HCV are the most important of these hepatotropic viruses as they frequently result in chronic persistent infection. While many of these chronically infected individuals are asymptomatic, persistent infection may lead to cirrhosis, liver failure, and hepatocellular carcinoma. As a result, chronic HCV is responsible for an increasing percentage of liver transplantations in industrialized countries. Moreover, HBV and HCV are the most important viral cause of carcinoma worldwide. In Table 8.1 these distinct types of viral hepatitis and their characteristics are summarized.
Despite the presence of multiple causative viruses, the clinical presentations of acute viral hepatitis are nearly identical. As a result, specific diagnosis of the etiologic agent requires serologic assays that are specific for each of the different viruses. The laboratory tests (serologic) used to differentiate the various types of acute hepatitis are listed in Table 8.2andBox 8.1.
This discussion will emphasize the epidemiology, mode of transmission, and clinical aspects of these five forms of hepatitis. The effects of these viruses during pregnancy on mother, fetus, and neonate will be reviewed. It is important to recognize that clinically apparent icteric hepatitis is only a part of the disease spectrum and that “silent” infections (carrier state) may result in chronic and progressive disease in the mother and her offspring. Exciting new developments in the therapy of HBV and HCV infection with both antiviral agents and immunomodulators will be discussed. Prevention efforts directed at HBV and HCV (vaccines and passive immunization) will be touched on but are presented in detail in Chapter 25.
A variety of other viral agents also infect the liver, producing an acute viral hepatitis-like syndrome. However, these cases of hepatitis present as part of a more systemic clinical presentation. These agents include cytomegalovirus, Epstein-Barr virus, herpes simplex virus, varicella-zoster virus, rubella virus, rubeola, mumps virus, coxsackie B virus, adenovirus, and yellow fever virus.
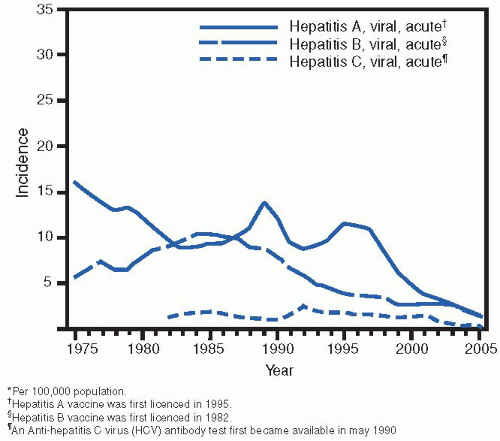
Although acute viral hepatitis is a common infection and is a reportable disease in the United States, the true incidence of this disease is not known. Of the more than 500,000 cases of acute viral hepatitis previously diagnosed each year in the United States, HAV accounts for 32%; HBV, 43%; HCV, 21%; and 4%, unknown. The estimated disease burden of viral hepatitis in the United States for the decade 1984 to 1994 is depicted in Table 8.3. In 2006, the number of acute cases reported to the Centers for Disease Control and Prevention (CDC) were HAV, 3,579; HBV, 4,713; and HCV, 802. Although these numbers are probably underestimates of the true number of acute cases, the incidence of HAV, HBV, and HCV infection has declined dramatically over the past several years to decade in the United States (Fig. 8.1). In large part these declines are attributed to the widespread availability of vaccines (HAV and HBV) and blood bank screening (HCV).
Despite its common occurrence and often benign course, acute viral hepatitis is a serious disease. The estimated mortality rate of viral hepatitis associated with clinical jaundice is 1%, and approximately 285 deaths from fulminant hepatitis occur each year in the United States. In general, the frequency of fulminant hepatitis and mortality rates are dependent on the age of infected persons and the causative agent of the hepatitis. The mortality rate is higher in elderly patients. Fulminant hepatitis occurs more commonly with hepatitis B and D than with other types of hepatitis, with mortality rates ranging from 2% to 20% reported in outbreaks of delta hepatitis. In addition, a unique finding with hepatitis E is the increased incidence of fulminant hepatitis and high mortality rate (approximately 10%) that occur in pregnant women, especially in the third trimester of pregnancy. While an exact incidence of mortality with acute HCV infection has not been reported, fatal cases do occur. Of greater concern than the morbidity and mortality associated with acute hepatitis is development of a chronic state with hepatitis B, C, and D, which can lead to significant sequelae such as chronic liver disease, cirrhosis, hepatocellular carcinoma, and nonhepatic diseases including polyarteritis nodosa, cryoglobulinemia, glomerulonephritis, and aplastic anemia.
Clinical Manifestations of Acute Viral Hepatitis
Acute viral hepatitis presents with a wide spectrum of findings ranging from asymptomatic disease to fulminant hepatitis. No clinical features are specific enough to clearly differentiate among the various types of hepatitis. While certain epidemiologic patterns of transmission may point to a particular hepatitis agent, confirmation of etiology requires serologic studies.
TABLE 8.1 ▪ CHARACTERISTICS OF THE MAJOR TYPES OF VIRAL HEPATITIS
The initial symptoms associated with the preicteric phase of acute hepatitis are nonspecific; malaise and weakness are the earliest and most common (95%) symptoms, followed rapidly by anorexia, nausea, vomiting, and mild, dull, right upper quadrant pain. This preicteric phase typically lasts 3 to 10 days. The icteric phase commences with onset of jaundice or dark urine or both. However, clinically evident icterus is present in only 20% to 50% of acute viral hepatitis infections. Approximately, 5% to 15% of patients with acute hepatitis present with a “serum sickness-like syndrome” during the preicteric phase. This syndrome is characterized by a triad of symptoms: fever, rash (urticarial), and arthritis (polyarticular and migratory). With the onset of jaundice, the “serum sickness-like syndrome” rapidly resolves. Other immune complex-mediated diseases are associated with acute viral hepatitis. These include polyarteritis nodosa (HBV), glomerulonephritis (HBV and HCV), and mixed cryoglobulinemia (HBV and HCV).
BOX 8.1 ▪ LABORATORY CRITERIA FOR DIAGNOSIS OF HEPATITIS
Acute hepatitis A
IgM antibody to HAV (anti-HAV) positive
Acute hepatitis B
IgM antibody to HBcAg (anti-HBc) positive and
IgM anti-HAV negative
Acute hepatitis C
Serum ALT levels >7 times normal and
IgM anti-HAV negative and
IgM anti-HBc negative (if not performed HBsAg negative) and
ONE OF FOLLOWING
Anti-HCV screening test positive, verified by additional more specific assay (e.g., RIBA for anti-HCV or nucleic acid testing for HCV RNA) or
Anti-HCV positive with a signal to cut-off ratio predictive of a true positive (e.g., >38 for EIA)
TABLE 8.3 ▪ ESTIMATED BURDEN OF VIRAL HEPATITIS IN THE UNITED STATES, 1984 TO 1994a
HAV
HBV
HCV
HDV
Acute infection
125,000-200,000
140,000-320,000
35,000-180,000
6,000-13,000
Fulminant deaths/year
100
150
?
35
Chronic infections
0
1-1.25 million
3.5 million
1,000
Chronic liver disease deaths/year
0
5,000
8-10,000
1,000
aReprinted with permission. Curry MP, Chopra S. Acute viral hepatitis. In: Mandell GL, Bennett JE, Dolin R (eds). Principles and Practice of Infectious Diseases. Philadelphia, PA: Elsevier Churchill Livingstone; 2005:1426-1440.
The most serious manifestation of viral hepatitis is fulminant viral hepatitis, which is defined as severe acute liver failure with hepatic encephalopathy that occurs at ≤8 weeks following onset of jaundice. HBV is responsible for 30% to 60% of these cases, and 30% to 40% of such patients are coinfected with delta virus. On the other hand, HAV infection is an uncommon cause, with <0.1% of acute hepatitis A cases progressing to liver failure and HCV alone has not been associated with acute fulminant hepatitis.
FIGURE 8.1 Viral hepatitis. Incidence, by year—United States, 1975
Physical examination in acute viral hepatitis reveals few findings. When the bilirubin level exceeds 2.5 to 3.0 mg/dL, icterus can be detected. Other findings on the skin include vascular spiders and, when severe pruritus exists, excoriations. On abdominal examination, the liver is slightly enlarged and tender. In patients with serum sickness-like syndrome, an urticarial rash and erythematous, warm, tender joints are present. With fulminant hepatitis, patients demonstrate signs of hepatic encephalopathy, including lethargy, somnolence, confusion, stupor, and ultimately full coma and asterixis (asynchronous flapping of dorsiflexed hands).
Laboratory findings associated with acute viral hepatitis are fairly specific. The most characteristic laboratory findings are dramatic elevations in aspartate aminotransferase (AST) and alanine aminotransferase (ALT). In contradistinction, alkaline phosphatase and lactic dehydrogenase (LDH) are only mildly elevated. Bilirubin, both direct and indirect in an equal ratio, is elevated in icteral hepatitis. In nonfulminant cases of acute viral hepatitis, the prothrombin time is normal. A prolonged prothrombin time is a serious sign and raises concern that more severe liver necrosis progressing to fulminant hepatic failure may occur.
HEPATITIS A
Hepatitis A is caused by infection with hepatitis A virus (HAV), a 27-nm RNA virus that is a member of the Picornaviridae family and may be classified as an enterovirus. Hepatitis A is usually a mild self-limited disease without any chronic sequelae. Infection may be asymptomatic or result in acute hepatitis. Fulminant hepatitis is rare.
Epidemiology
In the prevaccine era it was estimated that HAV was responsible for 30% to 35% of cases of hepatitis in the United States. In 2006 there were 3,579 cases of hepatitis A reported in the United States; the incidence was 1.2 in 100,000 population. This is the lowest rate of HAV infection ever recorded and represents a decline of 90% since 1995. To a large extent the decline is attributable to the introduction of the hepatitis A vaccine in 1996. Declines were greatest among children and in states where routine vaccination of children was recommended in 1999. According to the CDC, after taking into account asymptomatic infection and under reporting, an estimated 32,000 new infections with HAV occurred in 2005.
The mortality rate of hepatitis A is low (about 2 per 1000 icteric cases), and an estimated 100 persons die each year in the United States as the result of acute liver failure caused by fulminant hepatitis A. However, adults >50 years of age and persons with chronic liver disease are at increased risk for fulminant hepatitis A. Mild and clinically unrecognized infections with HA virus commonly occur in childhood (90% >5 years of age) and account for the high incidence of IgG anti-HA in adult populations, a finding reflected in the adequate antibodies present in normal immune serum globulin (ISG). The prevalence of previous HAV infection in the United States has been estimated to be approximately 40%.
The most frequently identified risk factor for HAV in the United States is international travel (15% of HAV cases), especially to Mexico and Central/South America. Other risk factors include (i) sexual and household contact with an individual infected with HAV (12% of cases); (ii) injection of street drugs (5% of cases); and (iii) MSM (3% of cases).
Transmission
Hepatitis A virus is transmitted predominantly via the fecaloral route (Box 8.2). HAV is highly contagious and can spread rapidly from person to person. HAV has been demonstrated to be spread by (i) contaminated water, milk, or food; (ii) breakdown in sanitary conditions following floods or other natural disasters; (iii) ingestion of raw or undercooked shellfish (oysters, clams, mussels) from contaminated water; (iv) travel to areas with poor hygienic conditions where hepatitis A is endemic; (v) exposure to children in daycare centers; and (vi) exposure to institutionalized individuals. In addition to the predominant route of fecal-oral transmission, HAV is transmitted by alternate routes such as intravenous drug use and sexual contact, especially among men having sex with men in whom HAV infection correlates with number of sex partners and frequency of oral-anal contact. Perinatal transmission of HAV is very rare. Persons in the United States who are at high risk for hepatitis A are those who have recently traveled to or immigrated from developing countries where hepatitis A is an endemic disease.
TABLE 8.4 ▪ CLINICAL AND EPIDEMIOLOGIC FEATURES OF ACUTE VIRAL HEPATITIS
Hepatitis A
Hepatitis B
Hepatitis C
Epidemiologic features
Onset
Acute
Acute and insidious
Insidious
Age group
Children and adults
All ages
All ages
Season
Fall and winter
All year
All year
Parenteral transmission
Rare
Common
Common
Nonparenteral transmission
Common
Common
Uncommon
Clinical features
Prodrome
Common
Common
Common
Severity
Mild
Mild to severe
Mild
Prognosis
Benign
More severe in older age group
Benign acute
BOX 8.2 ▪ HEPATITIS A VIRUS
Fecal-oral route of transmission
Acute infection usually mild
Fulminant hepatitis uncommon
No chronic carrier state
No perinatal transmission
Diagnosis
Acute viral hepatitis is a clinical syndrome that can be divided into four stages: (i) incubation period; (ii) preicteric phase; (iii) icteric phase; and (iv) convalescence. The clinical manifestations of viral hepatitis are usually so characteristic that diagnosis is reasonably straightforward (see previous discussion, Clinical Manifestations Acute Hepatitis). The comparative epidemiologic and clinical features of Hepatitis A, B, and C are shown in Table 8.4 The incubation period for hepatitis A ranges from 2 to 6 weeks, with a mean of 28 to 30 days. HA virus excretion peaks late in the incubation period and early in the preicteric phase, with the highest concentration in fecal material.
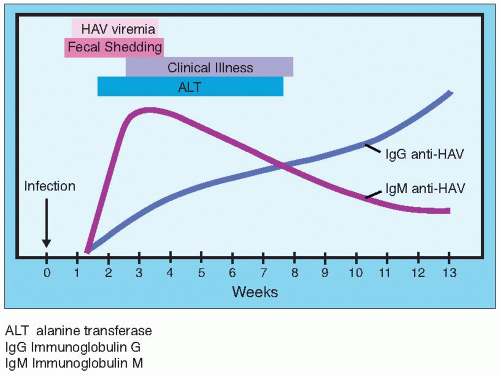
As noted above, no reliable methods are available to differentiate clinically among the types of acute viral hepatitis. Thus, once a diagnosis of acute viral hepatitis has been entertained, identification of the responsible viral agent requires use of serologic markers (Table 8.2). The clinical, virologic, and serologic course of acute HAV infection is shown in Figure 8.2. Antibody to HAV (anti-HAV) is present in the serum by the time of onset of clinical symptoms. The presence of IgM anti-HAV in a patient with clinical symptoms and/or enzyme evidence of acute viral hepatitis is diagnostic of acute HAV infection. After 3 to 12 months, IgM anti-HAV disappears and IgG anti-HAV persists to provide life-long immunity.
Pregnancy-Associated Hepatitis A Infection
In the United States it is estimated that hepatitis A occurs in approximately 1 per 1,000 pregnancies. There is no evidence that pregnant women are more susceptible to HAV and the course of hepatitis A is similar in pregnant and nonpregnant women. Usually, hepatitis A produces no adverse effect on the fetus; neither perinatal transmission (exception 1 case report) nor a chronic carrier state in the newborn occurs. No teratogenic effect of HAV has been noted. Transmission to the neonate from a mother acutely infected with HAV via the fecal-oral route is possible during delivery and postpartum. It appears reasonable to administer immunoglobulin to infants born to mothers who develop acute hepatitis A during the third trimester (or just prior to delivery). Whether such an approach is cost-effective has not been demonstrated.
Breast-feeding is not contraindicated in HAV-infected mothers. However, appropriate hygienic precautions to prevent fecal-oral transmission are necessary. HAV vaccine is not contraindicated in pregnancy. Similarly, immunoglobulin does not pose a risk in pregnancy and should be provided when indicated.
Treatment
There is no specific therapy for acute hepatitis A. Thus, the management of patients with hepatitis A consists primarily of supportive measures. Most of the patients with hepatitis A (including pregnant) can be managed on an outpatient basis. In general, patients require increased bed rest, a diet high in protein, and avoidance (if possible) of drugs that are hepatotoxic or metabolized by the liver. In the majority of patients, hepatitis A is mild and usually a self-limited infection. Indications for hospitalization of patients with hepatitis A include (i) severely debilitated patients who are unable to tolerate oral intake and require intravenous/hyperalimentation; (ii) severe anemia; (iii) diabetes; (iv) a prolonged prothrombin time; (v) low serum albumin level; and (vi) bilirubin ≥15 mg/100 mL. Patients with evidence of fulminant hepatitis, coagulopathy, or encephalopathy require treatment in an intensive care setting.
Patients usually recover from acute hepatitis A within 4 to 6 weeks. Hepatitis A does not progress to chronic hepatitis, and there is no HAV carrier state. Mortality from hepatitis A is low, ranging from 0.1% to 0.2%.
Prevention
HAV infection is overwhelmingly a self-limited disease and is not associated with chronic infection. Therefore, no specific antiviral agent(s) are recommended for treatment of hepatitis A. However, effective measures for prevention of HAV transmission exist. Two types of products are available for prevention of hepatitis A: hepatitis A vaccine and immunoglobulin. Passive immunization with pooled immunoglobulin (gamma globulin) has been used to prevent transmission or to ameliorate symptoms of acute hepatitis A since the 1940s. Prior to the licensing of hepatitis A vaccines, pooled immunoglobulin (IG) was the mainstay of hepatitis A immunoprophylaxis. Before vaccine availability, IG still plays an important role in hepatitis A prophylaxis. It is useful for preexposure prevention of hepatitis A in travelers to endemic areas where the 2-weeks’ time required for vaccine effectiveness is not available. In addition, IG remains useful in postexposure prophylaxis for common source or family outbreaks. When administered within 2 weeks of last exposure, IG is 80% to 90% effective in preventing clinical Hepatitis A. IG is recommended for postexposure prophylaxis and for unvaccinated persons expecting to be in a highrisk situation in less than 2 weeks. IG is also recommended for pre exposure prophylaxis for persons allergic to one of the vaccine components and for children <2 years of age (vaccine not approved). The usual dose of IG is a single intramuscular injection of 0.02 mL/kg, which will provide protection for up to 3 months. If exposure for 3 to 6 months is expected, a single injection of 0.06 mL/kg should be provided. For longer exposure, 0.06 mL/kg of IG is repeated every 5 months.
Active immunization (vaccine) is also now possible against hepatitis A. In the United States, two HAV formalin-inactivated hepatitis-A vaccines (Havrix and Vaqta) are currently approved and available. In addition, a combined Hepatitis A and B vaccine (Twinrix®) is available. Inactivated hepatitis A vaccines, available in the United States since 1995, are administered as a two-dose series in which a booster dose is given 6 to 12 months following the initial dose. The vaccines are safe (inactivated virus), highly immunogenic, and efficacious. They induce seroconversion to protective level of antibody within 2 weeks after the initial dose. Protective antibodies are present in 94% to 100% of adults 1 month after the first dose of hepatitis A vaccine. After the second dose, all persons had protective levels of antibody, which provide long-term protection (possibly 20 years of longer). The CDC notes that inactivated hepatitis A vaccines are 94% to 100% effective in preventing HAV infection. Hepatitis A vaccine is recommended for any person 2 years of age or older who is at increased risk of exposure to hepatitis A. Persons at high risk include (i) travelers to countries where HAV is endemic; (ii) military personnel; (iii) certain ethnic or geographic populations with high rates of HAV (Native Americans, Alaskan people); (iv) homosexual or bisexual men; (v) intravenous drug users; (vi) regular recipients of blood or plasma-derived products (e.g., factor VIII); and (vii) persons engaged in high-risk employment (primate handlers, laboratory workers who handle HAV, employees of institutions for developmentally challenged, and staff of daycare centers). In addition, vaccine should be considered for persons with chronic liver disease (at greater risk for serious outcome of HAV infection) and food handlers. Recently, the CDC updated their recommendations for postexposure prophylaxis and international travelers to include single antigen Hepatitis A vaccine as the preferred approach for post exposure prophylaxis. Similarly, they noted that one dose of vaccine administered at any time prior to international travel provides adequate protection for most healthy persons.
HEPATITIS B
HBV infection remains a major public health problem in the United States as well as worldwide, with an estimated 350 million HBV carriers worldwide and 500,000 deaths per year. Acute HBV infection may be asymptomatic or be associated with mild to severe clinically apparent acute hepatitis. While the majority of acute hepatitis B cases are self-limited and resolve, HBV infection may be persistent, often for the lifetime of the infected individuals. To a large extent, it is this characteristic of persistent chronic disease associated with serious long-term consequences, which makes HBV such an important pathogen worldwide. In Southeast Asia and sub-Saharan Africa, the prevalence of chronic HBV infection may exceed 10%, and HBV-associated liver disease is an important health problem, being the most common cause of chronic liver disease and hepatocellular carcinoma.
HBV, a member of the Hepadnaviridae (hepatotropic DNA virus) family, contains one of the smallest genomes among animal viruses, consisting of 3,200 base-pairs. Hepatitis B infection is related to the presence of three morphologically distinct viral-like particles, as seen by electron microscopic studies. The 42-nm HB virus is a DNA virus; the intact virus is termed the Dane particle and has an outer lipoprotein envelope containing surface antigens. Within the envelope is a 27-nm core containing the double-stranded DNA. The core is completely enveloped by surface antigen (HBsAg). Excessive amounts of DNA-free HBsAg are synthesized by the liver cells of infected individuals and circulate freely in the serum as 20-nm spheres and tubules. A large amount of viral antigen forms in the liver and is detected in the blood during acute and chronic infection; this is a unique characteristic of HBV infection.
An additional antigen antibody system, the e system, has been described in HBV infection. The e antigen is distinct from all known antigenic determinants of HBsAg and HBcAg but appears to be associated with the intact virus (Dane particle) and high serum levels of hepatitis B viral-specific DNApolymerase activity. The e antigen appears early in almost all patients during the acute phase of hepatitis B infection and may persist in patients in whom the infection progresses to chronic active hepatitis. Most importantly, several important prognostic and epidemiologic observations have been made with the e antigen. Persistent carriers of HBsAg who are e antigen-positive have a greater chance of developing chronic active hepatitis. Second, it has been demonstrated that HBsAg-positive blood that lacked e antigen but contained anti-e antibody did not cause post-transfusion hepatitis, whereas e antigen-positive blood carried a significant risk for development of post-transfusion hepatitis B. The third finding relates to pregnancy and vertical transmission of hepatitis B from mother to offspring. Mothers with e antigen-positive blood are much more likely (up to 90%) to transmit HB virus to their children than those with HBsAg-positive, e antigen-negative blood. Thus, it seems likely that the presence of e antigen identifies the group that is highly infectious and at greater risk of transmitting hepatitis B virus. The nomenclature of hepatitis B antigen and antibodies is summarized in Table 8.5.
Epidemiology
Prior to widespread use of HBV vaccines, the CDC estimated that approximately 300,000 primary HBV infections occurred annually in the United States accounting for approximately 40% to 45% of all cases of acute hepatitis in the United States. More than 10,000 HBV infected persons were hospitalized annually and 300 die from fulminant hepatitis. An estimated 6% to 10% (18,000 to 30,000 cases) of persons acutely infected with HBV became chronic carriers. Most acute HBV infection occurs in young adults, with one-fourth associated with acute icteric disease.
Following widespread use of HBV vaccine, a dramatic decrease in new HBV infections occurred. Since 1990, reported acute hepatitis B incidence in the United States has declined by 81% to the lowest rate ever reported in 2006 (1.6/100,000 population). Declines occurred among all age groups but were greatest among children aged <15 years. For 2006, there were 4,713 acute, symptomatic hepatitis B infections reported. After asymptomatic infection and under reporting were adjusted for, the CDC estimates there were 46,000 new HBV infections in 2006.
HBV infection occurs almost exclusively through contact with body fluids containing the virus (e.g., blood, semen, vaginal-cervical secretions). Individuals having contact with these fluids are at risk to acquire HBV. This includes intravenous drug users, healthcare workers, sexual partners of infected persons, hemodialysis patients, and infants born to mothers with HBV (Box 8.3). The virus gains entry into susceptible persons via breaks in squamous epithelium or through mucous membranes. While in developing countries the most frequent route for HBV transmission is perinatal vertical transmission, in the United States, sexual contact and percutaneous drug injection are the predominant modes. Detection of serum HBsAg has become the important diagnostic tool for identifying hepatitis B. HBsAg is present in approximately 1 per 1,000 adults in the United States and Europe. However, it is present in 2% to 25% of adults in tropical areas and Southeast Asia.
TABLE 8.5 ▪ NOMENCLATURE OF HEPATITIS B VIRUS ANTIGENS AND ANTIBODIES
Description
Antigen
Antibody
Comments
Dane particle; 42-nm size
Hepatitis B surface antigen (HbsAg)
Anti-HBs
DNA virus
Represents intact virus (surface and core)
Hepatitis B core antigen (HBcAg)
Anti-HBc
Hepatitis B e antigen (HBeAg)
Anti-HBe
Core of Dane particle; 27-nm size
HBcAg
Anti-HBC
Contains DNA polymerase in hepatocytes
Spherical and filamentous forms 22-nm size; have same antigen properties as surface of Dane particle
HbsAg
Anti-HBs
HbsAg denotes HBV infection; anti-HBs antibody is protective antibody
The incidence of acute hepatitis B infection varies in different populations in the United States. Persons at greatest risk include injecting drug users, hemodialysis patients, laboratory personnel working with human blood or blood products, men having sex with men, persons with multiple sexual partners, and medical/dental personnel with frequent contact with blood. Approximately 25% of the sexual contacts of infected persons become infected. While HBsAg screening has nearly eliminated blood transfusion as a source of HBV infection, it does not prevent 100% of the time. During childbearing age, 70% of women in the United States are susceptible to hepatitis B. The frequencies of acute hepatitis B and chronic hepatitis B in pregnant women are 1 to 2 in 1,000 and 5 to 15 in 1,000, respectively.
Asymptomatic carriers of hepatitis B are estimated to number about 1 to 1.25 million in the United States, and 350 million worldwide are believed to serve as an epidemiologic reservoir for hepatitis B infection. A large portion of these are in the populations of Southeast Asia and sub-Saharan Africa where the prevalence of chronic HBV infection is high and associated cirrhosis and liver cancer are major health problems. In the United States, approximately 4,000 to 5,000 persons die each year from chronic HBV infection (3,000 to 4,000 with cirrhosis and 600 to 1,000 with liver cancer). The medical and work-loss costs of HBV related disease in the United States is estimated to be at least $700 million. Worldwide, the HBsAg carrier rate varies from 0.1% to 20% in different populations, with up to 20% of the population in highly endemic areas such as sub-Saharan Africa, Southeast Asia, and Oceania are HBsAg carriers and almost all HBsAg negative adults have serologic evidence of past HBV infection (anti-HBs and/or anti-HBc).
BOX 8.3 ▪ MAJOR RISK FACTORS FOR HBV
Persons of S.E. Asian, sub-Saharan Africa, or Alaska Eskimo descent
Injection drug use
Multiple sex partners/history of STDs
Delivery to a HBsAg-positive mother
Healthcare/public safety worker
Household contact HBV carrier
Clinical Manifestations
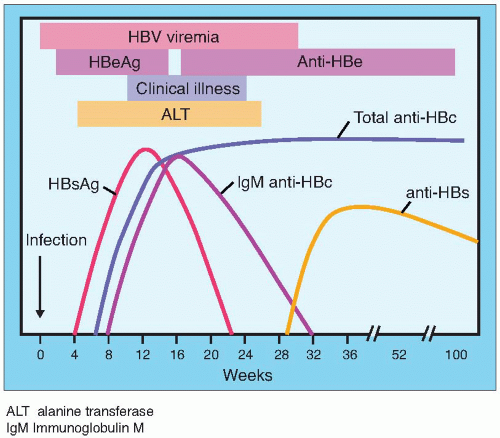
Clinical manifestations of acute hepatitis B are similar to those described for hepatitis A (also see Table 8.4). The incubation period for hepatitis B ranges from 45 to 160 days. Fulminant hepatitis and death occur uncommonly (<1%) following acute hepatitis B. In 85% to 90% of patients complete resolution of hepatitis B occurs with development of protective levels of antibody (Fig. 8.3). The remaining 10% to 15% of individuals became chronically infected (chronic carriers) with HBV (Fig. 8.4). Among these chronic carriers (HBsAg positive) 15% to 30% develop chronic active or persistent hepatitis or cirrhosis. Thus, approximately 1.5% to 4.5% of hepatitis B cases will develop chronic liver disease. Hepatocellular carcinoma occurs in a small percentage of these chronic cases. The persons who remain seropositive for the hepatitis B e antigen and/or become superinfected with hepatitis D and are at particular risk to develop chronic liver diseases. The hepatitis B virus is suspected to be oncogenic, and recently the integration of viral DNA with cellular DNA of human hepatocellular carcinoma has been demonstrated.
Two major diseases are associated with chronic HBV infection. Persistent HBV infection may result in chronic persistent hepatitis or chronic active hepatitis. Factors that correlate with the severity of both acute and chronic hepatitis B include inoculum of virus and young age.
HBV is not directly cytotoxic to hepatic cells. Rather, the host immune responses to HBV antigens displayed on infected hepatocytes are the principal source of the hepatocellular injury. In acute, self-limited hepatitis B infection there are strong T-cell responses to many HBV antigens present in peripheral blood. In contrast, these HBV-specific T-cell responses are substantially diminished in chronic carriers of HBV. Thus, T-cell responses, especially those of cytotoxic T lymphocytes, play a primary role in clearance of HBV.
Hepatocellular carcinoma is a second disease associated with chronic HBV infection. While rare in most areas of the world, hepatocellular carcinoma is common in sub-Saharan Africa, Southeast Asia, Japan, Oceania, Greece, and Italy. The areas where heptocellular carcinoma are common are those where HBV infection is common and persistent HBV infection is at a high prevalence. The incidence of hepatocellular carcinoma is 100 times higher in the HBsAg-positive group compared with the HBsAg-negative group. Although the association of HBV infection with hepatocellular carcinoma is strong, a viral hepatocarcinogenic mechanism has not yet been elucidated.
Several other syndromes of extrahepatic disease are also associated with HBV infection. A serum-sickness-like syndrome with fever, urticarial rash, arthralgias, and sometimes acute arthritis occurs in 10% to 20% of patients during the incubation period of acute hepatitis B. HBsAg-anti-HBs complexes appear to play a role in the pathogenesis of this entity. One-third to one-half of patients with polyarteritis nodosa have had persistent HBV infection. Similarly, many cases of membranous glomerulonephritis have been associated with chronic active hepatitis and persistent HBV infection. Some cases of essential mixed cryoglobulinemia have also been ascribed to HBV infection, but this association has been disputed.
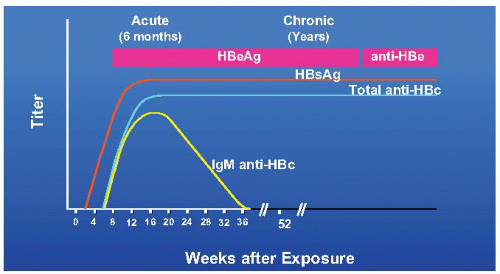
FIGURE 8.4 Progression to chronic hepatitis B virus (HBV) infection: typical serologic course.
Pregnancy and HBV Infection
Acute hepatitis B occurs in 1 to 2 of every 1,000 pregnancies, with an additional 0.5% to 1.5% of pregnant women being chronic carriers of HBV (i.e., HBsAg positive). Prior to routine vaccination of newborns, an estimated 20,000 infants were born to HBsAg positive mothers annually in the United States, resulting in approximately 6,000 infants who become chronic carriers of HBV. Transmission of HBV from mother to infant during pregnancy (predominantly intrapartum) is one of the most efficient modes of HBV spread and often results in long-term sequelae such as cirrhosis and hepatocellular carcinoma. Maternal-infant transmission of HBV can occur via four routes. These include (a) transplacental (probably rare); (b) intrapartum; (c) postpartum; and (d) in breast milk or colostrum. The predominant route for perinatal transmission of HBV is intrapartum via exposure to blood, genital secretions, and feces.
Approximately 80% to 90% of newborns of mothers with acute hepatitis B during the third trimester of pregnancy will become HBsAg-positive (Table 8.6). In contrast, when maternal hepatitis occurs in early pregnancy, transmission of HBV to the neonate occurs in 10% of cases. A crucial determinant of vertical transmission from mother to newborn is the presence of an e antigen (Table 8.6). HBeAg-positive mothers have high levels of virus and are more likely to transmit it to their offspring. Nearly all babies born to HBeAg-positive mothers became infected with HBV during the 1st year of life, and 85% become chronic HBsAg carriers. However, infants of mothers who are HBsAg-positive but HBeAg negative may also become infected (estimated risk 5% to 10%) and develop chronic hepatitis.
Only gold members can continue reading. Log In or Register to continue