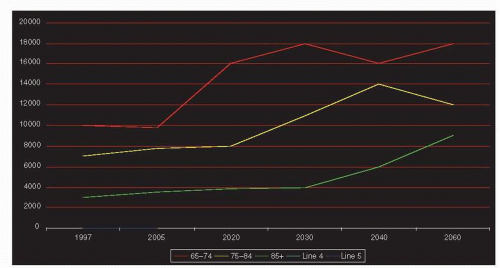
Disparities in breast cancer outcome in older women, where older is typically defined as age over 65 years, has drawn attention to the disease in this group which comprises almost one-half of all new cases. High incidence is due to the fact that age is a major risk factor for breast cancer; U.S. cancer statistics from 2004 to 2008 show that breast cancer occurred in 1 of 15 women aged 70 years and older and 1 of 28 women aged 60 to 69 years, compared to 1 of 27 women aged 40 to 49, and 1 of 203 women younger than 39 years (1). We also know that although breast-cancer-specific survival has improved over recent decades, improvements have occurred preferentially in women diagnosed at ages younger than 70 years (2). If the U.S. Census Bureau predictions hold true, by 2060 the number of older women age 65 to 84 years will nearly double and those 85 and older will nearly quadruple (Fig. 84-1A), resulting in a substantial increase in the number of breast cancer diagnoses in older women. Research thus far has only begun to determine how much of the disparity in age-related breast cancer mortality can be reduced. Epidemiologic studies have compared survival rates of older women with breast cancer to age-matched older women without breast cancer and to younger women with breast cancer. Compared to controls without breast cancer, matched for age, comorbidity, prior mammography use, and sociodemographic factors in a linked Surveillance, Epidemiology and End Results (SEER)-Medicare dataset, women with early-stage breast cancer (stage 0-I) who received standard treatment had similar mortality, while women diagnosed with stage II or greater disease had significantly greater mortality (adjusted hazard ratio for death, 1.5, 95% CI, 1.5-1.6) (3). Compared to younger women with breast cancer, survival disparities also appear to be most pronounced with higher stage, higher risk disease. In the Finnish Cancer Registry, survival rates were similar in older and younger women with node-negative disease, whereas with node-positive disease the 10-year relative survival was best for women 41 to 45 years (49%) and poorest in women over 75 years (35%) (4). Mortality trends seen between 1990 and 2003 in the Surveillance, Epidemiology, and End Results (SEER) program show that there was a decrease in mortality in younger and older women with estrogen receptor-positive disease, but, in estrogen receptor-negative disease, mortality decreased in women younger than 70 years and stayed stable in women age 70 and older (2). The detection of early-stage disease in older women, therefore, is important. For women with higher stage, higher risk tumors, the causes of differential outcomes by age is a topic of active research.
Studies of patterns of care in older breast cancer patients show that they are at risk for “less than standard” management, even after controlling for factors such as comorbidity, cognitive status, social support, and functional status. In addition, lack of receipt of standard, guideline concordant care increases the risk of poor outcomes. In a study using a SEER-Medicare linked dataset from 1992 to 2003, older women with early stage cancer who received standard treatment were significantly less likely to die within 5 years than were women who did not receive standard therapy (16% vs. 39% for stage I disease, respectively, and 33% vs. 64% for stage II disease, respectively) (3). This is true even for women over age 80 years, where 5-year breast cancer survival is 90% for standard breast conserving surgery with systemic therapy, compared to 46% with no treatment, 51% with tamoxifen alone, and 82% with mastectomy alone (5). The rate of guideline concordant care and associated lower survival reported in population studies is confounded by patient, tumor, physician, and other factors. Admittedly, delivery of standard care depends on the risk-benefit ratio, which is sometimes difficult to assess in older, possibly frail, women. The use of potentially toxic adjuvant therapies in older women is not well supported by the literature because they have traditionally been excluded from randomized clinical trials. Furthermore, as a group, older women are perceived as having more indolent breast cancers that require less aggressive therapy.
FIGURE 84-1 Population projections for women in the United States (in thousands). (From U.S. Census Bureau, Population Projections, Last Revised: 2012-12-14T16:41:27.218-05:00.)
In older women, the rate of local recurrence of ductal carcinoma in situ (DCIS) is lower than in younger women. Pathologic features of DCIS, however, do not appear more indolent in older women (6). Some authors attributed the lower local recurrence rate to immunohistochemical and genetic differences; HER-2/neu is less often overexpressed in DCIS in older patients, whereas ER, PR, bcl-2, cyclin D1, Ki-67, and p53 expression is similar (7).
With invasive breast cancers, the incidence of biologically aggressive phenotypes is less common in older women. Infiltrating ductal cancer is the most common histologic type. The more indolent histologic types, although still rare, are seen more commonly in older than in younger women. Mucinous carcinomas represent only 1% of breast cancers in premenopausal women, but 4% to 5 % in women aged 75 to 85 years and approximately 6% in women more than 85 years old (8). Papillary cancers are very rare in all age groups: 0.3% of cancers in premenopausal women and less than 1% in older women. The vast majority of breast cancers in older women are hormone receptor-positive, HER2-negative, so-called luminal A and B tumors. Markers of lower cell proliferation are common, including lower thymidine-3H labeling index, diploidy, lower histologic grade, normal p53 expression, and less overamplification of epidermal growth factor receptor (EGF-1) and c-erb-b2 (HER-2/neu) (8). Despite the apparent less aggressive phenotype, a large report, spanning 60 years and including 2,136 elderly women treated with surgery and without adjuvant systemic therapy, showed no difference in the rate of distant metastases between women over age 70 years compared to women age 40 to 70 years (9). Some attribute this to the fact that very low estrogen levels in older women affect the expression of progesterone receptors, which are less frequently positive, and androgen receptors, increasing the metastatic potential of the cancer. More aggressive tumors, such as ER/PR negative and HER2 positive cancers, however, do occur in even the oldest old patients and pose a higher recurrence and mortality risk regardless of age. In women age 70 and older with stage I-II breast cancer, for instance, tumors expressing HER2 carried 10 times the risk of recurrence at 5 years (30 vs. 3%) and lower cancer-specific survival rates (86% vs. 98%) compared to HER2 negative tumors (10).
LIFE EXPECTANCY—THE COMPLICATED INTERDEPENDENCE OF AGE, COMORBIDITY, AND FUNCTIONAL STATUS
As age increases, life expectancy decreases (Table 84-1), but even at age 80, the average woman’s life expectancy is 9.6 years. Most patients and clinicians realize that the range of expected life expectancy varies more as we get older due to other existing illnesses (comorbidities), the presence of frailty and disability, and other factors. Geriatricians use the Comprehensive Geriatric Assessment (CGA) to assess domains of functional status, comorbidity, medication use, cognition, social support, and nutritional status. The CGA can detect treatable geriatric syndromes in cancer patients, but it is time-consuming and rarely used in medical oncology practice. Instead, its components, screening tools, and abbreviated versions are in development. There are also tools to estimate survival, using information available clinically or excerpted from a geriatric assessment, that may assist in complicated treatment decisions in older patients. Some of these tools are available online, at ePrognosis (http://www.eprognosis.org). Several groups of experts, including the International Society of Geriatric Oncology (SIOG) and the National Comprehensive Cancer Network, recommend some form of comprehensive geriatric assessment be performed in older patients with cancer (11, 12).
TABLE 84-1 Average Remaining Lifetime Expectancy for Women at Various Ages
Age (y)
Life Expectancy, Women (y)
60
25.3
65
20.9
70
16.7
75
12.9
80
9.6
85
6.8
90
4.7
95
3.2
100
2.3
Table shows average number of years of life remaining life at the given age. Calculated using the longevity calculator of the official Web Site of the U.S. Social Security Administration (http://www. ssa.gov/cgi-bin/longevity.cgi).
Functional status is a strong and significant indicator of mortality risk. In oncology, the Eastern Cooperative Oncology Group (ECOG) and Karnofsky (KPS) Performance Status are typically used to measure functional status. These measures correlate well with cancer-related mortality, but they do not correlate as well with functional status assessed in the CGA, and may underestimate the degree of functional impairment in older patients (13). In a CGA, functional status refers to one’s ability to perform daily tasks, which allow one to care for oneself—activities of daily living (ADL)—and other tasks that allow one to live independently—instrumental activities of daily living (IADL). ADL and IADL are also strong predictors of survival. In addition, self-rated health is an independent risk factor for cancer-related and overall mortality (14). Compared to those rating themselves as “healthy,” the relative risk of cancer-related mortality for patients rating themselves as “moderately healthy” or “not healthy” was 4.2 (95% confidence interval [CI], 1.9-9.4), and the relative risk of mortality from other causes was 3.0 (95% CI, 1.2-7.8)—even after adjusting for the presence of major chronic diseases, age, medication use, smoking, alcohol consumption, physical activity, body mass index, systolic blood pressure, serum cholesterol concentration, education, marital status, and a family history of chronic diseases. Dementia, an important geriatric syndrome, and progressive functional decline are determinants of life expectancy as well (15). Related issues of poor social support and limited access to transportation may lead to delays in diagnosis with resulting increase in the likelihood of inadequate treatment of cancer in patients aged 65 and older.
The presence of comorbidity increases with increasing age and complicates management of breast cancer because as comorbidity increases, both overall mortality (16, 17) and breast-cancer-specific mortality increase. Comorbid conditions that impose functional limitations and that are expected to progress, such as diabetes with end-organ damage, steroid- or oxygen dependent chronic obstructive pulmonary disease, or a known terminal illness, definitely limit survival (18). With aging, heart and cerebrovascular diseases become increasingly more important as causes of death (Fig. 84-2). In addition, there is an interaction between comorbidity and stage of disease, such that the effect of comorbidity on survival varies by breast cancer stage (18); among patients with three or more comorbid conditions, prognosis is poor regardless of stage.
In conclusion, not only age but also geriatric indices, including functional status and comorbidity, are important in predicting overall survival, breast-cancer-related survival, and treatment tolerance. Consideration of these and other factors will ultimately help us optimize treatment strategies for older women with breast cancer.
PREVENTION
Like younger women, older women should be encouraged to maintain a healthy life style that includes exercise and weight control. Overall, available data suggest that few older women are likely to be good candidates for pharmacologic strategies of breast cancer prevention; the risk/benefit ratio is rarely favorable. (See Chapter 21 for a detailed review of breast cancer prevention strategies.)
SCREENING
Breast cancer screening, also discussed in Chapter 11, involves serial mammography, clinical breast examination, breast self-examination, and in some high-risk situations, although not typically in older patients, breast MRI. For older postmenopausal women, the higher probability of developing breast cancer as compared to younger women translates to a greater likelihood that a newly detected breast mass or mammographic abnormality is likely to be a breast cancer. In one study comparing mammographic results of women aged 50 to 64 years (n = 21,226) to women aged of 65 years and older (n = 10,914), Faulk and colleagues found that mammography had a higher positive predictive value, a higher yield of positive biopsies, and a greater cancer detection rate per 1,000 studies in older women (19). Finding an early cancer in an older woman, however, may not lengthen or improve her life and raises concern of overdiagnosis. The current questions about screening older women are, therefore: (i) Do older women who are screened live longer than those who are not screened (due to finding cancers at a more curable stage)? (ii) Do older women who are screened have a higher quality of life than women who are not screened (due to finding cancers earlier when they require less aggressive treatment)? (iii) Do older women require screening less frequently than yearly (due to slower-growing cancers)? (iv) Is there an age at which screening mammography should cease?
The answers to the first of these two questions are not directly available. Large randomized trials show that routine annual or biannual mammography in women aged 50 to 75 years is associated with a reduction in breast cancer- related mortality of 25% to 30% within 5 to 6 years of initiation (20). As only two of these trials included women older than 75 years, the optimal upper age limit for mammographic screening is still a matter of debate (21). The U.S. Preventive Services Task Force recommends biennial screening mammography be performed in women between the age of 50 and 74 years, but concludes that the evidence is insufficient to assess the additional benefits and harms of screening mammography in women age 75 and older (22). Population-based studies suggest that cancers detected by screening mammogram in older women may result in lower stage cancer at diagnosis, but there is no demonstrable survival benefit. The frequency of screening mammography in women older than age 75 is an area of debate. The fact that breast cancers in older women tend to have features suggesting slower growth suggests that less than annual screening is reasonable. Prospective data to support screening mammography in older women do not exist.
FIGURE 84-2 Cause of death within age-groups (percent). (Data from Yancik R, Wesley MN, Ries LAG, et al. Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. Jama 2001;285:885-892, with permission.)
An upper age limit for screening mammography does not exist. Most experts deem that screening is justifiable as long as the benefits outweigh the risks. One study claimed that, since high bone mineral density (BMD) was associated with increased risk of breast cancer, that women should first be screened with BMD and, if high, should have screening mammogram (23). After age 80, when life expectancy is most likely less than 10 years, screening mammogram can probably be discontinued. In fact, the risks of screening women over age 80 may outweigh the benefits. In a cohort study of 2011 women age 80 and older, for instance, there was no difference in breast cancer rates, stage, or death between screened and unscreened women, but among the 1,034 women screened, 11% had false-positive mammograms that led to 19 benign breast biopsies (24). The use of a framework or decision aid for guiding decision-making about screening that is based on life expectancy, risk of dying of cancer, and procedure-related complications has also been suggested (25, 26).
In 1991, Medicare made screening mammography every 2 years a covered benefit and, in 1999, annual screening was made a covered benefit. During the first years of Medicare coverage, most older women were unaware that screening was a Medicare benefit, which led the Health Care Financing Administration to publicize mammography coverage. Selfreported 2-year mammography screening rates for women more than 65 years old increased from 43% in 1990 to 64% in 1998. Even with screening mammography as a covered benefit and after several national informational campaigns, 60% of a sample of 1,000 older female Medicare beneficiaries in Michigan between 1993 and 1997 either had not undergone a mammogram or had undergone only one (27). Attention to factors associated with lower mammography use improves screening rates. The physician’s recommendation is probably the most important stimulus for obtaining screening mammography in older women. On-site mobile mammography, personalized mailings, and emphasis on the reassurance that mammography brings recipients are also helpful in improving screening rates.
The American Geriatrics Society Clinical Practice Committee published guidelines for breast cancer screening in older women (see Table 84-2) (28). The committee recommended annual or biennial mammography until age 75 years and then biennially or every 3 years thereafter in women with a life expectancy of 4 or more years. Overall, while it is less clear that mammography saves lives in women over age 75, it definitely finds cancers at an earlier stage, thus allowing less aggressive treatment and perhaps a better quality of life and survival. Longer intervals between mammograms are likely adequate and careful clinician breast exam may be beneficial. Mammography for women with a life-expectancy of at least 5 years and intact mental function and mobility makes good medical sense.
TABLE 84-2 Breast Cancer Screening Recommendations for Older Women
Technique
Recommendation
Mammography
Annual or biennial mammography until age 75 and biennial or every 3 y thereafter, with no upper age limit for women with an estimated life expectancy of 4 or more years.
Clinical breast examination
Annual
Breast self-examination
Monthly
Modified from American Geriatrics Society Clinical Practice Committee. AGS position statement: breast cancer screening in older women. J Am Geriatr Soc 2000;48:842-844, with permission.
TREATMENT OF THE PRIMARY LESION IN THE OLDER PATIENT
After the publication of the NSABP Protocol B-06 in 1985, it became accepted that women with invasive breast cancer should be offered the choice between modified radical mastectomy and breast conservation (lumpectomy, axillary dissection, and breast irradiation). Since that time, breast conservation has become the more common surgical approach, and axillary dissection has been replaced by sentinel node biopsy, with the addition of axillary dissection reserved for the highest risk cases (see Chapters 41 and 42).
Older women should be offered the option of breast preservation, because body image and the loss of a breast are important issues regardless of age. In addition, breast preservation is a much less morbid procedure, mostly done as an outpatient procedure, and is thus preferable to mastectomy in the older individual with comorbidities. There should be a low threshold for the use of preoperative endocrine therapy to increase the rate of lumpectomy or decrease the extent of surgery as discussed elsewhere in this chapter (adjuvant therapy). In fact, women aged 70 and older are more likely to prefer breast conservation than mastectomy. Individualization of treatment is appropriate, and decisions should be made based on patient preference, overall health, tumor stage, and biology.
Today, most older patients can receive effective surgical treatment with minimal mortality risk and morbidity. Operative mortality rates for breast surgery are very low, at 1% to 2%. The main factor influencing surgical morbidity is not age but the presence of comorbidity and frailty. There may be at least a short-term decrease in cognitive function after general anesthesia in elderly patients, and even a slight decrease in cognition in an older frail patient may mean the difference between independence and consignment to assisted or total care. Attention should be paid to functional status and comorbid illnesses in making decisions about surgical management.
MANAGEMENT OF THE AXILLA IN OLDER PATIENTS
In the management of invasive breast cancer, sentinel node biopsy is preferred in the patient with clinically node-negative disease. Axillary dissection may also be omitted in women who have breast conserving surgery and pathologically involved nodes, as long as surgical margins are negative, the tumor is less than 5 cm, there are fewer than three involved nodes and the nodes are not matted, there is no extranodal extension of tumor, and in the absence of neoadjuvant endocrine or chemotherapy; these recommendations are based on the eligibility criteria for the Z11 trial (see Chapters 37 and 38). In the elderly woman with clinically benign preoperative nodal exam, however, axillary evaluation may not always be necessary.
Axillary lymph node dissection may lead to arm morbidity and other complications, especially in the elderly. In a longitudinal cohort study of 571 patients with stage I and II breast carcinoma who were 67 years of age and older, the risk of arm dysfunction during the 2 years after initial treatment was more than four times higher for women who underwent axillary dissection compared with women without axillary dissection (83% vs. 17%; p = .0001) (29). In a study that randomized women age 60 and older to axillary clearance or not, however, after the first postoperative visit (at which point the physician and patient assessment of quality of life related to arm symptoms was worse for women who had the axillary dissection), disruptions in quality of life disappeared within 6 to 12 months and there was no long-term difference in arm movement or pain (30). Thus, despite the potential morbidity, for elderly women with clinically positive axillary lymph nodes who can tolerate surgery and do not meet the Z11 criteria noted above, axillary dissection represents the best treatment. Alternative treatments, such as irradiation and tamoxifen (if the tumor is ER- or PR-positive) may play a role in controlling disease for a short time in patients too ill to have surgical treatment.
For older women with clinically negative nodes and a hormone receptor-positive tumor, in whom chemotherapy is unlikely to be used, axillary evaluation by sentinel node biopsy may be superfluous and add morbidity without benefit. A retrospective study of patients treated with lumpectomy plus tamoxifen, but without irradiation or axillary dissection, for instance, found low rates of recurrence in the ipsilateral axilla at 5 and 10 years; axillary relapse rates were 4.3% and 5.9%, respectively (31). Axillary recurrence was also low among older women who did not have axillary surgery in the Cancer and Leukemia Group B (CALGB 9343) trial (32). This trial, done in conjunction with RTOG and ECOG, included women age 70 and older with small (≤2 cm), clinically or pathologically node-negative, ER-positive or PR-positive primary breast cancers treated by lumpectomy plus tamoxifen who were then randomized to receive breast irradiation or not. Axillary surgery was not a requirement for study entry. In the radiation arm none of the 200 women who did not undergo axillary dissection had an axillary recurrence, whereas 2.9% (6 of 204) who did not undergo axillary clearance or have breast radiation had axillary recurrence. Finally, the International Breast Cancer Study Group (IBCSG) trial 10-93 randomized women age 60 and older with clinically node-negative, operable breast cancer, in whom adjuvant tamoxifen was indicated, to axillary clearance or not (30). Of participants in this trial, 80% had hormone receptor-positive breast cancer. At a median follow-up of 6.6 years, axillary recurrence (∽2% overall), disease-free survival (67% vs. 66%. HR 1.06; p = .69), and overall survival (75% vs. 73%, HR 1.05; p = .77) were not significantly affected by axillary surgery. Even in the absence of axillary evaluation or treatment, therefore, axillary recurrence is rare in older women with small, ER-positive tumors treated with tamoxifen, radiation, or both.
In summary, for older women with ER-positive or PR-positive cancers that are 2 cm or less who undergo breast conservation therapy, for whom chemotherapy is unlikely to be beneficial regardless of node status, axillary evaluation, even with sentinel node biopsy, has little utility. For tumors greater than 2 cm, or ER-negative and PR-negative tumors, sentinel node biopsy has utility for determining who might best benefit from adjuvant chemotherapy or axillary treatment. For the node-positive patient who does not meet the Z11 criteria, axillary dissection remains the standard for those who can tolerate the procedure.
BREAST RADIATION AFTER LUMPECTOMY
Older women tolerate breast irradiation as well as younger women, but consigning an older person to 4 to 6 weeks of radiation therapy may be exhausting and be detrimental to her quality of life. Thus, the schedule and duration of adjuvant breast radiation may be obstacles for older patients. One approach to this problem has been the development of radiation therapy schedules that are more tolerable for older patients. Two retrospective analyses examined the use of once-weekly radiation schedules. Rostom et al. reported the use of once-weekly irradiation for 84 older patients with breast cancer (stages I to IV) (33). Treatment was well tolerated. Reactive fibrosis, skin thickening, or both occurred in 25 patients; symptomatic pneumonitis was reported in 4 patients; and brachial plexopathy occurred in 1 patient. Among patients with stage I and II tumors, local tumor control and cosmetic results were encouraging. Maher et al. (34) evaluated a regimen that included once-weekly radiation therapy for a total of seven fractions and concurrent tamoxifen in a group of older women with a mean age of 81 years (range, 64 to 91 years). At a median follow-up of 36 months, the overall survival rate was 87%, the disease-specific survival rate was 88%, and the local recurrence rate was 14%. With the high dose per fraction, 39% of patients experienced moderate fibrosis at the primary site. No rib fractures, radiation pneumonitis, or brachial plexopathy were seen.
Another approach to decreasing the inconvenience of radiation therapy is accelerated partial breast irradiation (APBI) using external beam radiation or intracavitary balloon brachytherapy, and which treats only the affected area of the breast and requires about 1 week for completion (35). This usually requires two treatments per day, obviating some of the convenience gain hoped for in the elderly. APBI is discussed in great detail elsewhere in this text (see Chapter 35), but there are some data specific to the elderly. Smith et al. (36), using the National Medicare Data set for women age 67 or older, identified that brachytherapy produced significantly greater morbidity than whole breast radiation (WBRT) at 5 years (fat necrosis 8.26% vs. 4.05% and breast pain 14.55% vs. 11.92%). They also found a significant difference in ultimate mastectomy rates in favor of WBRT (3.95% APBI vs. 2.53% WBRT), although we would be hard pressed to call this difference clinically relevant. However, another report by Khan et al. found no difference in local recurrence, cosmesis or toxicity when comparing women over 70 versus women 70 or younger treated with brachytherapy (37). Finally, targeted intraoperative radiotherapy (IORT) offers the option of radiation given as a single dose intraoperatively, markedly decreasing inconvenience for the patient. Initial reports suggest a low rate of in breast recurrence (38).
While shorter courses of radiation seem feasible and likely effective in older women, the question remains whether older women need radiation after breast preservation at all. Standard local treatment for breast cancer has similar disease-free and overall survival benefits in older and younger women, but older women have more deaths from illnesses other than breast cancer (11% vs. 2%; p = .0006) (39, 40). In CALGB 9343, only 3% of all study patients died of breast cancer while 47% died of other causes and survival was the same with or without radiation (32).
Only gold members can continue reading. Log In or Register to continue