, Joong Mo Ahn2 and Yusuhn Kang2
(1)
Department of Radiology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, South Korea
(2)
Department of Radiology, Seoul National University, Bundang Hospital, Seongnam, South Korea
Accurate radiological diagnosis of bone tumors is based on a systematic and organized analysis of the clinical and radiographic features. Factors to be considered include clinical factors such as the age and gender of the patient, and radiographic factors of the lesion including location, biological activity, matrix mineralization, periosteal and endosteal reaction, and size and number of lesions. Each of these features is discussed and illustrated in detail in this chapter.
1.1 Demographics
Age
The age of the patient is the single most important clinical data in establishing the diagnosis of a bone tumor. Certain bone tumors have a predilection for patients of certain age groups. For example, for an intramedullary osteolytic tumor involving the metaphysis and epiphysis of a long bone, chondroblastoma would be high up on the list of possible diagnoses, if the patient is 10–20 years old. However, in a patient aged 20–40 years, giant cell tumor would be moved high up on the list. Table 1.1 lists the benign and malignant tumors frequently encountered in each age group.
Table 1.1
Age predilection of bone tumors
Age | Benign | Malignant |
|---|---|---|
<20 | Chondroblastoma, chondromyxoid fibroma, osteoid osteoma, osteoblastoma, fibrous dysplasia, nonossifying fibroma, fibrous cortical defect, desmoplastic fibroma of bone, giant cell tumor of small bone, simple bone cyst, aneurysmal bone cyst, osteofibrous dysplasia, Langerhans cell histiocytosis | Osteosarcoma, Ewing’s sarcoma |
20–40 | Giant cell tumor of bone, osteoid osteoma, osteoblastoma, fibrous dysplasia | Osteosarcoma (parosteal, periosteal, low-grade central), chondrosarcoma (periosteal) adamantinoma |
>40 | Metastasis, plasma cell myeloma, solitary plasmacytoma, chondrosarcoma, osteosarcoma (secondary, >60) | |
Wide age range | Chondromas, benign fibrous histiocytoma of bone, intraosseous lipoma, hemangioma | Fibrosarcoma, angiosarcoma, primary lymphoma of bone |
Gender
Most tumors are found equally in both genders, but some show predilection for a certain gender. Table 1.2 shows the predilection of some tumors for a certain gender.
Table 1.2
Gender predilection of bone tumors
Strong male predilection | Osteoblastoma (2.5:1), High-grade surface Osteosarcoma (2:1), Chondroblastoma (2:1), Clear cell Chondrosarcoma (3:1) Solitary plasmacytoma of bone (2:1) , Simple bone cyst (3:1) |
Slight male predilection | Enostosis, Telangiectatic Osteosarcoma (1.5), Periosteal Osteosarcoma Osteochondroma, Chondromyxoid fibroma Conventional Chondrosarcoma, Dedifferentiated Chondrosarcoma Ewing’s sarcoma(1.4:1) Angiosarcoma, Lymphoma(1.5:1) |
Equally distributed | Osteoma, Chondromas (enchondroma, periosteal chondroma), Mesenchymal Chondrosarcoma, Fibrosarcoma of bone Plasma cell myeloma, Aneurysmal bone cyst, Fibrous dysplasia |
Slight female predilection | Low-grade central Osteosarcoma, Small cell Osteosarcoma, Parosteal Osteosarcoma, Hemangioma (2:3) |
Strong female predilection | Giant cell tumor of bone (1.5– 2:1) |
1.2 Lesion Location
Bone tumors, both benign and malignant, have predilection for specific bones and certain locations within a specific bone. Table 1.3 shows the predilection sites of certain tumors within the skeleton. For example, for an osteolytic intracortical lesion at the anterior tibia, the most probable diagnosis would be osteofibrous dysplasia or adamantinoma. The location of a lesion within a specific bone can be specified along the longitudinal axis (i.e., epiphysis, metaphysis, and diaphysis) and the transverse plane (i.e., central intramedullary, eccentric intramedullary, cortical, juxtacortical) (Fig. 1.1). For example, a simple bone cyst is typically a central intramedullary lesion in the metaphysis of a long bone, with the most common site being the proximal humerus (Fig. 1.2a). Chondroblastomas are characterized by its intramedullary epiphyseal location in a long bone (Fig. 1.2b). Nonossifying fibroma appears as cortical lesions of the metaphysis of a long bone (Fig. 1.2c). Parosteal osteosarcoma is an example of a juxtacortical location of lesion, and has a predilection for the posterior aspect of the distal femur (Fig. 1.2d). Recognizing these site predilections of different bone tumors will aid in the differential diagnoses of bone tumors. Table 1.4 shows the predilection sites in summary.

Table 1.3
Predilection for specific bone
Site | Common tumor |
|---|---|
Tibia anterior cortex | Osteofibrous dysplasia, adamantinoma |
Calcaneus | Simple bone cyst, intraosseous lipoma |
Posterior cortex of distal femur | Parosteal osteosarcoma, periosteal desmoid |
Distal phalangeal tuft | Epidermal inclusion cyst, glomus tumor |
Short tubular bones of hand | Enchondroma |
Great toe | Subungual exostosis |
Calvarium | Osteoma |
Mandible | Desmoplastic fibroma of bone, giant cell lesion (giant cell reparative granuloma) |
Fig. 1.1
Lesion location. (a) The location of a lesion within a specific bone can be specified along the longitudinal axis: epiphysis, metaphysis, and diaphysis. The epiphysis is the rounded end portion of a long bone, where it forms a joint with adjacent bones. The diaphysis is the tubular shaft portion of a long bone, and the metaphysis is the wide portion of a long bone located between the diaphysis and epiphysis. In the transverse plane, lesions can be either (b) central intramedullary, (c) eccentric intramedullary, (d) cortical, or (e) juxtacortical in location
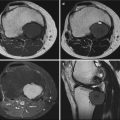
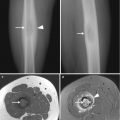
Fig. 1.2




Predilection sites of lesion. (a) Simple bone cysts are located at the metaphysis of a long bone with a central intramedullary location, and the most common site is the proximal metaphysis of humerus. (b) Chondroblastomas are located at an intramedullary epiphyseal location within a long bone. (c) Nonossifying fibromas appear as cortical lesions at the metaphysis of a long bone. (d) Parosteal osteosarcoma is a juxtacortical lesion with a strong predilection for the posterior aspect of the distal femur
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
