time between viral infection and the development of the detectable antibody response.
peptide it requires twice-daily subcutaneous dosing and is used uncommonly. Raltegravir (RAL) and elvitegravir (EVG) inhibits the viral-specific enzyme HIV integrase that inserts the viral DNA into the host cell DNA.
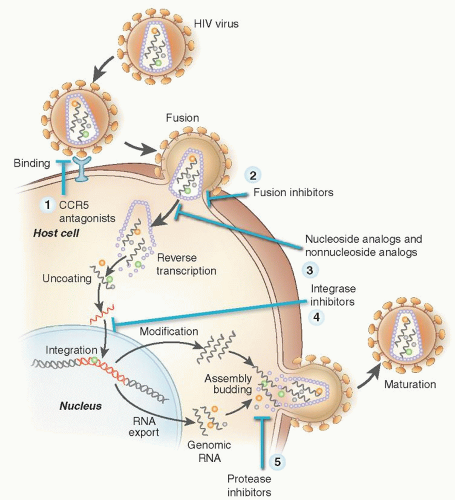 FIGURE 64.1. The human immunodeficiency virus (HIV) life cycle, deciphered with the help of genomic analyses, is unusually complex in its details, but all viruses undergo the same basic steps to infect cells and reproduce. Points at which antiretrovirals act are marked. |
analogs, have little or no effect on hematopoiesis.31, 48 It is important to note that HAART itself improves anemia as shown in a single center retrospective series in the HAART era. HAART was associated with hemoglobin levels >140 g/L in 42% of patients, irrespective of use of zidovudine as part of HAART regimen, compared with 31% of patients who did not use HAART.49
TABLE 64.1 HEMATOLOGIC TOXICITIES OF ANTIRETROVIRAL DRUGS | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
Related posts:
 The Diagnostic and Therapeutic Approach to Hematologic Problems
Mast Cells and Basophils: Ontogeny, Characteristics, and Functional Diversity
Platelet Structure and Function in Hemostasis and Thrombosis
Hemochromatosis
Sickle Cell Anemia and Other Sickling Syndromes
Anemias Secondary to Chronic Disease and Systemic Disorders
The Diagnostic and Therapeutic Approach to Hematologic Problems
Mast Cells and Basophils: Ontogeny, Characteristics, and Functional Diversity
Platelet Structure and Function in Hemostasis and Thrombosis
Hemochromatosis
Sickle Cell Anemia and Other Sickling Syndromes
Anemias Secondary to Chronic Disease and Systemic Disorders
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


