Introduction
Cushing’s is often considered to be the most difficult endocrine disorder to diagnose, manage, and treat. Though there are more than two dozen morbidities associated with this disorder, none is specific to Cushing’s. In fact, four of the most common initial symptoms reported by Cushing’s patients are at or near endemic levels in American adults:
-
•
Hypertension affects 48.1% [ ].
-
•
More than 42% have obesity [ ]
-
•
30%–40% report experiencing insomnia [ ]
-
•
Depression touches one out of every five [ ].
Patients often spend years ruling out more common diagnoses across multiple specialties, and they frequently report that cortisol testing is never offered. Once they themselves start to suspect Cushing’s and ask for specific testing, in many cases they are denied due to low/no suspicion or insurance issues. This is especially bitter when the Cushing’s diagnosis is ultimately confirmed and these patients must contend with the devastation of worsened symptoms caused by an average delay of five or more years. The Cushing’s Support and Research Foundation (CSRF) conducted a 2022 quality of life study in which 90% of respondents felt that “This is a disease where you must get very sick before it can be diagnosed and treated” [ ].
Undoing harm caused by gaslighting, gross health inequities, social media, and a history of appointments with biased and inexperienced providers is a lot. The role and value of an active science- and fact-based patient advocacy and support group cannot be overstated here! There are endless nuances to how Cushing’s affects each person in their lives, and the simple act of connecting at a meeting or on a face-to-face call with people who have lived your struggles is huge. Receiving the gift of actionable advice from others who have found ways to solve or ameliorate the same things that are blocking your progress is priceless. For the provider, knowing that their patient is getting trustworthy information and support can be a relief, and hopefully, it translates to better communication and progress in the clinical setting. We are a community.
The goal of this chapter is an eye-opening exploration of the patient experience. I called a committee of six “Cushies” with various backgrounds to have a conversation about high-priority topics, and you will find snippets of this conversation throughout the sections. You can learn more about these advocates in Appendix II.
Close, but no diagnosis
The lead-up to an answer
Many patients are quite ill by the time they get to the doctor who will ultimately diagnose them, but when did their Cushing’s symptoms start? Almost all patients who are diagnosed can look back months or years and identify symptoms, mysterious illnesses, cycles of infections, unexplained weight gain, and other afflictions that seemed to make no sense. At the time, these odd symptoms are often summarized as stand-alone conditions or results of poor lifestyle choices, and that can lead patients down frustrating, unsuccessful, and sometimes inappropriate paths of treatment and behavior modification ( Fig. 18.1 ).
Data from CSRF’s 2022 member quality of life study.
Reprinted with permission from CSRF.
Respondents to CSRF’s 2022 quality of life survey were nearly unanimous that we must find a way to work with and educate nonendocrine doctors who typically see us long before we get to an endocrinologist: primary and mental health care, rheumatology, dermatology, urology, pediatrics, and bariatrics are some examples of areas where an informed practitioner might consider cortisol testing.
-
Bill D: If it wasn’t for a nurse practitioner who suspected my “soft bones” might be related to hormone issues, I might never have been referred to an endocrinologist and had the imaging and testing done that confirmed my diagnosis of a rare form of Cushing’s Syndrome—primary bilateral macronodular adrenal hyperplasia (PBMAH). Debilitating and repeated back issues really impacted me before my Cushing’s diagnosis. I had always loved playing different sports. During my worst episodes, when I had to crawl to the bathroom and was on hydrocodone, I was able to use hydrotherapy at a city pool to restore my mobility. Several attacks of poison oak and another rash from cellulitis sent me to the doctor for skin issues but the issues that I wouldn’t talk to anyone about were psychological. These included extreme spikes in emotional stress, panic attacks, anxiety, insomnia, sudden mood swings, and uncontrolled scratching.
-
Sylvia T: I did not suspect anything was wrong in a serious way and only went to a doctor when a leg muscle became sore and wouldn’t heal after 3 months. That doctor instantly suspected Cushing’s syndrome, which was a shock to me. The level of cortisol in my blood gave me artificial energy and I was very active—so in the early stages it didn’t seem to be affecting my life in a detrimental way. I was diagnosed in 1987 but did not agree to surgery until 1990 when I finally had to admit that my life was significantly interrupted, I couldn’t work anymore, I was constantly exhausted, and my coping abilities were nonexistent.
-
Anonymous: As a woman in her 40s, there were many ailments that I was aware of, but did not bring up with my physician because I just thought “I’m getting older.” I was losing hair, not sleeping well, gaining weight, and growing ugly chin and chest hairs. Finally, at my annual physical, I asked my GP to test my cortisol and she agreed. I’ve come to understand that this is somewhat unusual to find a nonendocrinologist willing to screen for high cortisol so I feel very lucky that she did not delay this testing.
Around this time I had already been thinking about changing careers because what I was doing had become too stressful and I was no longer feeling effective in my role. I took some time off to explore my options, and when the pandemic hit in 2020, my forgetfulness, fatigue, and other symptoms I came to know were from Cushing’s were full-time in my life. There was no way I could have kept up with any type of job while in active Cushing’s, and I was glad to not still be working when my cortisol testing came back elevated and ultimately lead to my diagnosis.
-
Maja N: I was normally athletic and skinny, but at some point I began to notice that I was terribly out of breath, feeling like my legs were lined with concrete. Within a couple of years, I no longer recognized myself in the mirror. Until then I had only ever done thyroid and basic blood tests. No one suspected Cushing’s syndrome, and it would take between five and 7 years until the real diagnosis. The last trigger was the sudden appearance of hypertension, terrible chest pains, shortness of breath, weakness, and always waking up around 3:00 a.m. As it was the time of COVID-19, I made an appointment with pulmonology because of the breathing and blood pressure difficulties. This was fate, because from a large number of doctors I passed, I came into the hands of an extraordinary internist, a pulmonologist who urgently sent me for extensive laboratory examinations including a CT where my adrenal tumor was found.
-
Nina B: About 5 years prior to my diagnosis and despite the fact that I was working out on a regular basis, I gained more than 50 pounds, and it was in the most awkward places: my face was fuller, I no longer had collarbones, and I experienced truncal obesity. I went from being the pretty girl in the family to being socially awkward and uncomfortable in public places. I began to experience headaches, blurred vision, and cystic acne, among other symptoms. During my annual physical, it was revealed that I was becoming diabetic and hypertensive. At that point in my life, I was only 34 years old and had never had any significant medical problems, so when my doctor discovered the elevated blood sugar, he made an appointment for me to see endocrinology. As a practicing nurse, I went home and googled endocrine disorders and typed in some of my symptoms. This led me to discover that I had every physical symptom of Cushing’s Syndrome. I recall telling my physician that I believed I had Cushing’s, and he told me that it was too rare of a disorder for African Americans , which made me second guess what I believed was true in my heart.
Until my diagnosis, it was difficult for me to be around anyone outside of my son and dog for long periods of time. I was committed to getting better for them. I am very close to my family but I couldn’t face them because I felt like a monster. During this time, I had to quit my part-time job as a bedside nurse and took a leave of absence from my teaching job. I sought help immediately. I would say from the time that I first started having symptoms and noticing that something was different to the time of diagnosis was 12–18 months.
-
Sonia F: One year after my second pregnancy (2013) I was diagnosed with a prolactinoma and had surgery to remove it. Because of this, I had regular MRIs and visits with my endocrinologist. About 5 years later I started to have sleep problems, and after persistent hip pain developed, I was diagnosed with a stress fracture. My endocrinologist ordered a bone density test, and turns out I had osteopenia at 43 years old. After a 24 hours urine test, my calcium was high; they thought that my kidneys were not working properly and put me on medication to stop the calcium release. That worked, but after resuming sport I kept gaining weight. I was eventually diagnosed with Cushing’s Disease and put on a medication, and though my MRI was negative, an IPSS confirmed a pituitary source. Later I switched to a different medication but had to stop it because it gave me edema. This was a really difficult period of my life, I didn’t recognize myself physically and mentally, and I couldn’t see the end of the tunnel. I looked for support and joined CSRF. Through CSRF I was recommended a surgeon who could perform an advanced technique and underwent surgery with him, but I did not experience the expected cortisol crash afterward. I had a second surgery 2 weeks later. Still no crash. It was very hard for me and my family. I couldn’t be cured. I started yet another medication and it took 4 months to find the right dosing. Although I am not cured, I can now sleep, I lost 12 kg, no more bruises, no more buffalo hump. When I look in the mirror I finally recognize myself.
What does it feel like?
Symptoms and experiences
Cushing’s Syndrome can produce around 30 symptoms, with no two patients showing the same set of symptoms. There’s historically been heavy reliance on overt physical symptoms like dark stretch marks, a moon face, the buffalo hump, truncal obesity, and supraclavicular fat pads to build pretest suspicion and support diagnosis, but it cannot be stressed enough that not everyone experiences classic visible symptoms . Some mild cases present with little or no physical symptoms and only reveal themselves in certain labs. Non-Caucasian skin looks different from and changes in ways that are not well-represented in literature, if at all.
Things get complicated if you consider secondary symptoms of Cushing’s:
-
–
family dysfunction that results from one parent suddenly being unable to fulfill their traditional role, stay awake, avoid rage, or find the energy to participate in recreational activities
-
–
crippling anxiety and insecurity for a young adult who’s rapidly gaining weight and whose facial features are being distorted into a hirsute dinner plate
-
–
divorce that comes from the ill partner’s loss of libido or fertility.
Sometimes these secondary effects can resolve or improve when hypercortisolism is put into remission, but years of conversations with patients suggest a greater likelihood of unhealthy internalization, traumatization, and chronic unmet needs.
I delayed my own diagnosis because of a lifetime of being fat. It gets old, always hearing about it. For years I refused to allow doctors to weigh me when I had an appointment. But at some point, “fat” started to become something else. I frequently miscalculated spaces I walked through and ran into doorways and table edges. I no longer fit into booths. I only fit the largest size from the plus-size store, and it had to have elastic. Walking up stairs was nearly impossible in the most bizarre way, like my legs were made of cement. I fell any time I increased my pace to a light jog or more, and getting up off the ground was a Herculean feat.
I woke up around 3:00 a.m. every night, I was hot and sweaty all the time, and I had horrible acne on my face, neck, shoulders, back, and abdomen. And the rage! I caused so much damage to my relationship with my teenage daughter, I am grateful that we have reconnected and have a good relationship now. I frequently felt as though I was going a little bit crazy and needed to hide that from everyone. I developed unhealthy coping mechanisms in desperation for any type of relief. After some hurtful name-calling while out in public 1 day, I stopped going out unless absolutely necessary. My ankles and feet were always so swollen, and I only had one pair of slip-on shoes that fit.
-
Bill D: I experienced a bewildering variety of symptoms for years before getting my diagnosis. This included everything from severe back pain (from extruding discs and spinal stenosis) to hypertension, ventricular tachycardia, panic attacks, saliva gland stones, skin rashes, muscle wasting (arms, legs and buttocks), insomnia and anxiety, repeated cracking of ribs, and even an untreated heart attack that was diagnosed years later from CT imaging (it turned out my LAD artery was over 99% obstructed). My cluster of physical symptoms shared none of the classic Cushing’s signs. I had no purple striations, no hump back, no obesity.
-
Sonia F: My sleep pattern was bad, waking up at 3:00 a.m. in the morning and impossible to get back to sleep. I developed osteopenia, and the buffalo hump. All the bruises, the thin hair (I cut them short), the hair on my face, and then gaining weight. Also during that period my blood tests were abnormal and I was followed by a hematologist. We never realized that the abnormal results were because of Cushing’s.
-
Nina B: My symptoms included weight gain, moon face, truncal obesity, hair loss, hair growth in awkward places, headaches, severe acne, visual changes, anxiety, depression, fatigue, memory loss, and confusion. I believe I was the textbook image of what a clinical Cushing’s patient looks like.
-
Maja N: My symptoms included anxiety, hypertension, brain fog, shortness of breath, a few extra pounds, anemia, high cholesterol, night awakenings always around 3:00 a.m., loss of muscle mass, pain of small joints, puffiness of the face, chronic stress, sluggishness as if I did not have enough strength, intense hair loss … but also anemia, nervousness, and shortness of breath.
-
Anonymous: The first symptoms I remember talking about were my head hair falling out, not being tired at night, and hair growing on my chin and chest. I also developed frantic thinking and a feeling of short-term memory loss.
-
Sylvia T: The first symptom that bothered me was a pot belly that I could not get rid of. I had lots of other symptoms that I ignored—oily hair, some facial hair, eating excessively, and anxiety. I also started to notice that I had decreased muscle strength when I couldn’t keep up during swimming training. I was diagnosed because of leg muscle soreness!
Navigating unpredictable territory
Treatment options, difficult surgeries, preparing for the unknown
Patients experience barriers to access for myriad reasons, and in a perfect world, their doctor would not be one of them. It is overwhelming to learn you have a complex, dangerous disease whose first line of treatment is almost always invasive surgery. A healthy part of coming to terms with this new reality would be the opportunity to make truly informed, consensual decisions about your healthcare. A challenge can be that some of us do not arrive at a Cushing’s diagnosis with a full understanding of the endocrine system, how hormones work together, or even where precisely the adrenal glands or pituitary are located in the body.
At the time of this writing, in the United States we have nine medications available that block/lower cortisol: five are FDA-approved, three are generic, and one is from Europe but you can get it if you jump through a few extra hoops. For a rare disease, that’s pretty amazing! There are promising clinical trials running for new therapies, there are several surgical options including more than one type of radiation, and in worst-case scenarios it’s possible to remove your adrenal glands and/or your pituitary gland and keep living. Insurance is there throughout your journey trying to play way too much of a decision-making role, but otherwise, it sounds like we’re all set!
Except that we also have …
-
•
doctors who do not feel comfortable prescribing one or more medications, and do not tell their patients about the ones they don’t like
-
•
recurrence rates of pituitary Cushing’s that can reach 50% if tracked long enough
-
•
average delays of three or more months to get an appointment with an endocrinologist
-
•
mind-boggling health inequity even in the “richest country on earth”
-
•
nonuniform adherence to society guidelines that lead to alternative interpretations of what makes a diagnosis
-
•
unscrupulous players sharing misinformation in populous Cushing’s social media groups
Reaching remission doesn’t seem to happen easily for most patients, and many consider true remission and recovery to start when cortisol is normalized either after the postsurgery hydrocortisone taper, or once permanent adrenal insufficiency is diagnosed and the patient is stabilized on their daily dose. Remission doesn’t mean back to normal, though. In our 2022 study [ ], half of respondents shared that one or more autoimmune disorders were unmasked or new after resolution of their high cortisol, and more than half reported that they were unable to fully return to work ( Figs. 18.2 and 18.3 ).
-
Bill D: Although my team of three surgeons were able to remove both adrenal glands and confirmed there were 10 tumors on each, their laparoscopic instruments nicked my jejunum in three places. They were able to make repairs with sutures by running the small bowel to the terminal ileum, but unfortunately, the surgeons didn’t realize they’d also nicked an adrenal artery while working on the second adrenal gland. By the time this was noticed and I was rushed into another surgery, about 1.5 L of coagulated blood had accumulated in my abdomen after 3 days of internal bleeding. They were only able to locate the small arterial nick after removing my spleen.
Data from CSRF’s 2022 member quality of life study.
Reprinted with permission from CSRF.
Data from CSRF’s 2022 member quality of life study.
Reprinted with permission from CSRF.
The doctors explained to my wife later that my nonclassic Cushing’s physique had proved challenging. They had found they had less space in my abdomen to maneuver than with traditional Cushing’s patients.
-
Sylvia T: I was not given any information about how I would feel after the operation, but I was given information about how they would perform the pituitary surgery. I didn’t realize how serious it was as I had nothing to compare it to. I was very naïve—I even asked the doctor if it was minor or major surgery! I faced financial barriers to accessing therapeutic treatments such as massage and counseling to ease my suffering after surgery. I also feel that once my biochemical remission was confirmed, my medical team dropped me like a hot cake. I couldn’t understand why the doctors were so interested in me before surgery and completely disinterested in me after surgery.
Another barrier I faced was that I could not advocate for myself. The doctors told me I was cured so I blamed myself for feeling constantly, extremely ill after the operation.
-
Anonymous: I was just told the best treatment was surgery. To this day I get very emotional when talking about being unprepared for treatment. I brought a list of symptoms with me to my first and only appointment with my surgeon before going into surgery. He said about 80% of them would resolve and I’d be feeling “so much better after a few days.”
When you don’t know what you don’t know, things seem overly simple in hindsight. I’d just have the surgery, have a period of adjustment, and wouldn’t even need a medical alert id bracelet. I was diagnosed fairly quickly compared with other stories I hear, and I didn’t even get around to trying to find a support group before surgery was scheduled. I just trusted that things would go well because I had no concept of things going wrong. My surgeon spoke with confidence, and I knew he knew a lot about the pituitary gland. Looking back, we were so poorly prepared for what came after surgery. My spouse only took a few days off of work, and I started thinking about getting back to work myself after a couple of months. Feels like a joke now.
-
Maja N: I feel that I was often not given enough information about treatments. No discussion of medications, I was given one option, surgical removal of the adrenal gland and then hydrocortisone replacement therapy. I wish they had explained to me and pointed out that the recovery was long-lasting and that the real fight began after the operation.
-
Nina B: The one thing that I regret not being told about is the road to recovery and what that journey will look like. I had a belief that I was going to wake up after surgery and feel like myself again. That could not be further from the truth. You never really feel like yourself again. You just slowly begin to embrace your new normal, whatever that is.
-
Sonia F: My first attempt at treatment failed, then I could not tolerate a medication due to the side effects. After the failed pharmacological attempts my tumor was located and I could undergo surgery. This second time, they placed patches in the nose which made breathing difficult for the first 10 days. Then, I was a bit afraid of the cortisol crash since it didn’t happen in the hospital and could happen any time (sometimes it can be delayed) but it never happened to me.
I was then recommended to try yet another cortisol-lowering medication. I am a scientist, so I read a lot of scientific articles on various treatments for Cushing’s disease. It was a slow process to get this final medication to the right dose, so morale was not always there, but it finally worked. Sleep was already improved after the surgery, but the weight loss happened after the cortisol was completely controlled and it was very gradual, one or 2 kg lost per month. Patience is needed.
The drop off
Support after surgery
This personal account from patient advocate Bill D describes a complicated onboarding of Addison’s Disease after surgery:
Post-surgery, the best support that I’ve found has been through research and education opportunities and patient groups like CSRF and the National Adrenal Disease Foundation (NADF). It’s been invaluable to connect with fellow patients and share stories and advice and to participate in more research studies.
Most Cushing’s patients struggle with their postsurgery steroid replacement therapy, and it’s hard to find endocrinologists who are knowledgeable and committed to quality of life issues. It’s remarkable that blood tests are not always done to assess the effective dosing levels for fludrocortisone and hydrocortisone that can help patients avoid daily fatigue and adrenal crises. My first cortisol blood testing after the initial follow-up tests done postsurgery didn’t come until 5 years later when I joined the national MyAI Registry [ ] and was accepted into a clinical study looking at hydrocortisone absorption. I learned that I am functioning with next to zero cortisol for many hours of the day.
Years ago, at a patient education day at the NIH, Dr. Stratakis offered this succinct information about quality of life for long-term survivors:
In brief, we know that life for patients with CS is not easy with or without a cure. Children with CS suffer through deterioration of academic performance from CS for the first few years post-operatively. Most children find it difficult to cope, even when they are young adults; we described a few of these patients that attempted suicide, despite being cured from CS for many years. Adults with CS suffer similarly and there are several recent publications on this issue. Adults report fatigue and executive dysfunction even after cure. Although other patients with pituitary tumors experience similar problems, the issues of patients with CS stand out … Of course, a lot of questions remain: now that we know the quality of life is impaired in patients even after complete cure of their hypercortisolemia, we do not know why this is the case.
On a practical level, I found the patient education I received about “Adrenal Insufficiency” (also known as Addison’s Disease) following and in advance of my Cushing’s surgery was poor in comparison with the education I got following my vascular surgery and a resulting DVT. There was no comparison between the way doctors addressed the administering of an intramuscular emergency shot of 100 mg hydrocortisone in the event of an adrenal crisis, and the instruction and physical demonstration I received on how to do daily self-injections of blood thinner subcutaneously in the abdomen by my vascular surgeon. It was like experiencing two different medical cultures. According to the 2015 findings of the Endocrine Society’s own task force on the diagnosis and treatment of primary adrenal insufficiency (PAI), nearly 50% of PAI patients are not sufficiently skilled in stress dosing and only 12% of patients reported giving themselves an injection during an adrenal crisis [ ]. Both medical fields are dealing with potentially deadly consequences.
Robert Frost has a famous poem about the depths and darkness of depression described as walking in the rain and going beyond “the furthest city lights” ( Fig. 18.4 ):
“Acquainted With The Night” (1928) Robert Frost.
Public Domain.
Too often, the Cushing’s experience, like many challenging chronic health issues, can involve depression and a slow disintegration of relationships and emotional support. My wife and children witnessed a lot of heightened cortisol behavior over the years, behavior that I didn’t even understand, but they still had the patience to put up with me. After my surgeries, they gave me the time and space to rebuild and reconnect with them, something no Cushing’s survivor can take for granted. The psychiatrist who saw me at the NIH prescribed an antidepressant to help regain my appetite and cope with PTSD, but I stopped taking it a few months after returning home because of its side effects.
The reality of postsurgery Cushing’s is that physical activity often remains more limited. That’s often the result of Cushing’s comorbidities and the cumulative damage done to the body over many years. Heart and bone issues continue to slow me down. Fatigue still comes in daily waves. Chronic back pain and an incisional hernia make exercise more challenging. Although not every day is a good day, the smallest pleasures can be enough to keep one going and feeling grateful.”
Patient Advocate Sylvia T had a different experience, a contrast with Bill on many points:
I did not receive support through treatment and recovery from my endocrinologist or physician. I suffered alone, possibly because no one understood the aftermath of surgery. I felt I had to fight for my life. Without having any prior knowledge of what to expect, all the aftereffects of surgery induced extreme fear in me. I thought I would have to spend the rest of my life with migraine, joint and muscle pain, extreme weakness and feeling nauseous constantly. I was so frightened every day- I did not know how I could survive like this- this fear lasted for two years until my adrenals started to work and I began to improve. Even now, I still experience fear when I am in a state of fatigue or exhaustion.
One exception was in the year after my surgery, by a lucky fluke I happened to come across a program called the Commonwealth Rehabilitation Scheme in my hometown of Perth, Western Australia. I enrolled and got to see a psychologist, a dietitian, and a physiotherapist through government support. I feel that at the time it kept me alive because I could focus on my next appointment—one every 2 weeks—something that kept me going when I had nothing else in my life but struggle.
I wish I was given education on how I would feel after surgery, and that recovery would be slow. I should have been given information on steroid withdrawal syndrome, muscle and joint pain, anorexia, nausea and vomiting, migraine, depression, loneliness, extreme weakness, and fatigue. I wish I was given a timeline of physical recovery and been informed that I would feel worse before getting better.
I wish I had been told that I will have very little energy after surgery and that I needed to have complete rest and to not feel guilty about resting. I should have been told to rest as much as possible and to not undertake anything that is physically, emotionally, or mentally stressful for at least the first 6 months after surgery.
I wish I had been informed on how to explain to family and friends that recovery is extremely slow and that I need extended rest and I am not being lazy. When they see you look better after surgery, they expect you to be back to normal. I wish I had been informed on how to respond to accusations of laziness which were very hurtful, and how to not blame myself when I couldn’t get back to my normal life and achieve the things I wanted to do. I wish I had been told that it was not my fault that my body has been damaged by cortisol.”
Related posts:
 Endogenous Cushing’s syndrome: Causes and genetics
Endogenous Cushing’s syndrome: Causes and genetics
 Identification of Cushing’s syndrome (CS) and its history from Harvey Cushing to today
Identification of Cushing’s syndrome (CS) and its history from Harvey Cushing to today
 All about dexamethasone testing in Cushing’s syndrome
All about dexamethasone testing in Cushing’s syndrome
 Cushing syndrome in pediatrics: From molecular pathogenesis to therapeutic management
Cushing syndrome in pediatrics: From molecular pathogenesis to therapeutic management
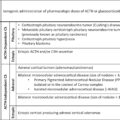
 Ectopic ACTH- or CRH-producing tumors and Cushing’s syndrome
Ectopic ACTH- or CRH-producing tumors and Cushing’s syndrome
 Adrenal tumors causing Cushing syndrome: Genetics, molecular advances, diagnosis, and treatment
Adrenal tumors causing Cushing syndrome: Genetics, molecular advances, diagnosis, and treatment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


