inconsistency between studies may be partially attributed to small sample sizes, different time points of blood collection, different types of coagulation tests used, and different patient populations.
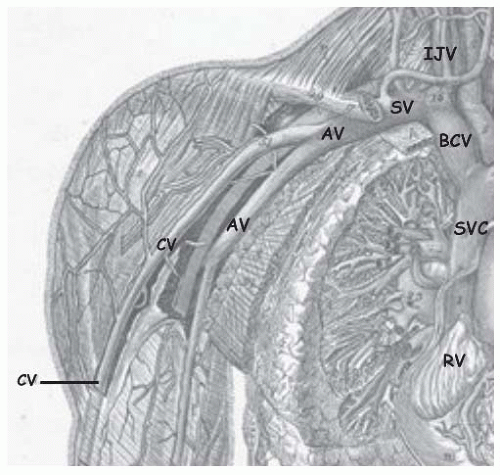 FIGURE 84.1 Veins of the upper extremity. The axillary vein (AV) extends to the outer border of the first rib where it becomes the subclavian vein (SV). The subclavian vein joins the internal jugular vein (IJV) at the inner end of the clavicle to form the brachiocephalic vein (BCV), which merges with the contralateral BCV to form the superior vena cava (SVC). RV, right ventricle. (Copyright protected material from Anatomy Atlases used with permission of the authors and Dr. Michael P. D’Alessandro, http://www.anatomyatlases.org/atlasofanatomy/plate19/04overview.shtml.) |
Table 84.1 Risk factors for UEDVT | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 84.2 Prevalence (%) of acquired and inherited thrombophilia in patients with UEDVT | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
usual symptoms of UEDVT are extremity edema, discomfort, and erythema.13 Patients with coexisting PE may also have dyspnea, chest pain, or cough.33
Table 84.3 Advantages and disadvantages of imaging modalities used to diagnose UEDVT | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Low-molecular-weight heparin (LMWH) is a safe and effective alternative and may reduce the duration of hospitalization.91 Typically, heparin is used as a “bridge” to warfarin therapy, which is continued for a minimum of 3 months with an international normalized ratio of 2.0 to 3.0.9,59,92 A longer duration of anticoagulation may be appropriate if there is an underlying hypercoagulable state.63,93,94
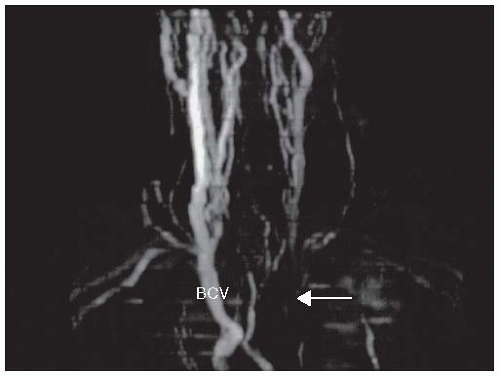 FIGURE 84.2 MRA demonstrating left BCV (arrow). (Adapted from Joffe HV, Goldhaber SZ. Upper-extremity deep vein thrombosis. Circulation 2002;106(14):1874-1880.) |
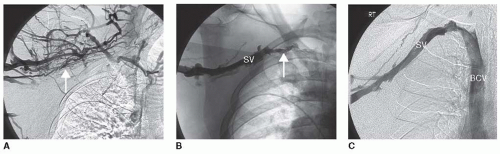 FIGURE 84.3 Multimodal therapy for UEDVT: 51-year-old weight lifter complaining of right arm pain. Initial venogram (A) shows occluded right axillary and subclavian veins with flow through collateral vessels (arrow). After percutaneous thrombectomy (B), there is persistent occlusion of the proximal subclavian vein (arrow). After thrombolysis (C), the subclavian vein (SV) is fully patent with flow into the brachiocephalic vein (BCV). (Adapted from Joffe HV, Goldhaber SZ. Upper-extremity deep vein thrombosis. Circulation 2002;106(14):1874-1880.) |
followed by prompt surgical correction, such as resection of bone or lysis of dense, perivascular adhesions.12,17,59,104,114,115,116,117,118 Persistent strictures after surgery could be treated with venoplasty and possibly vein stenting.119,120 This multimodal approach can successfully achieve long-term vessel patency.7,16,17,99,120,121,122,123 Although surgical thrombectomy restores venous patency, this approach is considered as a last resort because it is invasive, requires general anesthesia, and may be complicated by pneumothorax and brachial plexus damage.59 Conservative therapy rather than prompt surgical intervention may be preferable for selected patients with the thoracic outlet syndrome because physical therapy, weight loss, and nonsteroidal anti-inflammatory medications may avert the need for surgery.15
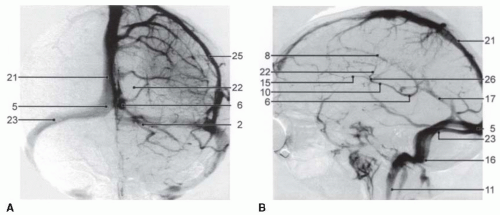 FIGURE 84.4 Venous phase of carotid angiography in the anteroposterior (left panel) and lateral (right panel) projections. The superior sagittal sinus (21), confluence of sinuses (5), transverse sinus (23), sigmoid sinus (16), and IJV (11) are as indicated. (Reproduced from the Encyclopedia of Medical Imaging [Medcyclopaedia], with permission.) |
have no identifiable cause or are associated with head trauma, oral contraceptive (OC) usage, pregnancy or the puerperium, cachexia, dehydration, local malignancy, arteriovenous malformations, or other causes of generalized hypercoagulability. CVST is a well-recognized manifestation of the inherited and acquired thrombophilias, complicating virtually all of the known causes.142,143,144,145,146 Of note is the danger of cerebral vein thrombosis in patients with a hereditary predisposition who have been prescribed OC agents8 and in patients with paroxysmal nocturnal hemoglobinuria (PNH), antiphospholipid syndrome, and myeloproliferative disorders.147,148,149,150 Following thrombus formation in a venous sinus, increased venous pressure leads to cerebral edema and even hemorrhage (FIGURE 84.5), a process that may progress to the development of large and/or multiple venous infarctions, which cross the normal boundaries of arterial supply.151
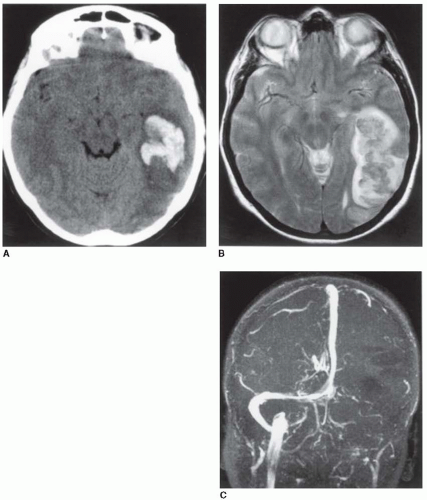 FIGURE 84.5 Intracerebral venous sinus thrombosis. A: Shows an axial CT scan with hemorrhagic infarction of the left temporal lobe. B: Shows the MR, T2-weighted axial image, with an isointense area of recent hemorrhage and a hyperintense area surrounding the infarcted edematous zone. C: Shows an angiographic MR study with occlusion of the left transverse sinus, the sigmoid sinus, and the internal jugular vein. (Reproduced from the Encyclopedia of Medical Imaging [Medcyclopaedia], with permission.) |
seizure as an early manifestation, associated with supratentorial thrombotic lesions (OR = 3.0). Headache in combination with papilledema and absent focal neurologic signs can simulate brain tumor (“pseudotumor cerebri”).155 Nausea, vomiting, and mental confusion develop over hours to days, followed in the most severe cases by stupor and coma, but focal sensory or motor losses are not dominant features, and the cerebrospinal fluid and the electroencephalogram may show only nonspecific findings. Fever will usually accompany sinusitis or other infection that leads to direct extension of the process into a contiguous (e.g., cavernous) sinus. Diagnosis is established by magnetic resonance (MR) or computerized tomography (CT) venography,141,156,157,158,159 which documents the important contribution of “cytotoxic edema” in the pathogenesis of cerebral venous infarction.160 D-Dimer levels have been noted to be elevated, in correlation with the degree of thrombosis, and it is unlikely that an acute thrombotic event exists in the face of a normal D-dimer value.161 Predictors of adverse outcomes (death, dependency) are age >37 years, coma, intracranial hemorrhage, central nervous system infection, or malignant disease.162
Related posts:
 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


