Fig. 50.1
(a) Manual lymphatic drainage of the upper limb; (b) treatment of posterior lymphatic alternative ways
Sequential compression (today mostly confined to the self-therapy at home), in which the partial local (lymphangitis, dermohypodermitis, varicophlebitis) and systemic (arterial hypertension and congestive heart failure) contraindication criteria are adhered to; unlike the lymphatic drainage that essentially drains the protein component of edema, this contributes to removing the water component in a short time (Fig. 50.2).

Fig. 50.2
Pressotherapy of the lower limb
Isotonic gymnastics with stimulation, through special exercises that activate the muscle pumps of the limbs, both the suprafascial lymphatic pathways and the subfascial to be carried out in groups as well within the structure or on outdoor paths during hospitalization (Figs. 50.3 and 50.4).


Fig. 50.3
Physical exercise during bandaging for activation of muscular pumps of the upper limb
Fig. 50.4
Treadmill under elasto-compression of the lower limbs for specific muscular activation
Personalized elasto-compression with multilayer inelastic bandages on the wound using the “herringbone” or “figure-of-eight” technique in subjects who are able to perform adequate muscle exercise during the various phases of the day; stretch fabric as the first layer and inelastic in the subsequent 2–3 layers in patients able to perform discrete muscle exercise during the day, two-way stretch in a single layer for bedridden, disabled, or elderly patients. After intensive treatment during hospitalization, the operators are in a position to prescribe the definitive elastic garment (standard or “custom-made”), which will provide the primary means of maintaining and consolidating the results obtained with the intensive therapeutic regime (Figs. 50.5 and 50.6).

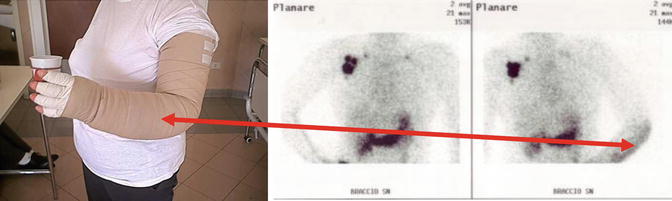
Fig. 50.5
Phases of bandaging of the lower limb
Fig. 50.6
Bandaging in the forearm area increases consistency of the tissue (demonstrated by the lymphoscintigraphy)
Ultrasound, used with a power of 2 W/cm, with good clinical success, is mainly employed, even for prolonged periods of time (30–40 min), in the fibrotic areas (Fig. 50.7). The radial shock waves have important effect on the fibrotic component of the edema and any tissue calcification that is an expression of past acute lymphatic episodes [3, 9] (Fig. 50.8). In some areas (in case of edema of the face), the only possible physical therapies are the manual lymphatic drainage and the vacuum therapy (Fig. 50.9). In secondary lymphedema, physical protocol must include (above all in some clinical cases) occupational therapy (Fig. 50.10) [10].





