52 Under normal circumstances blood is most easily taken from a vein in the antecubital fossa; the median cubital vein is preferred (Figs 52.1 and 52.2). It is considerate to ask whether the patient is left- or right-handed and then to choose the non-dominant arm. A tourniquet is applied well proximal to the site. This should cause distension of the veins but not discomfort. Gentle palpation is the best method of identifying a vein and checking its patency. If a suitable vein proves elusive it may help to gently tap the area or to warm the arm in water. The skin over the chosen vein is thoroughly cleaned with antiseptic solution. Usually a 21- or 22-gauge needle is used but a smaller size (e.g. 23) can be used where the veins are fragile, or in children. The syringe should be adequate for the sample – where larger blood samples necessitate more than one syringe a ‘butterfly needle’ may be preferred to a conventional venepuncture needle. The needle is inserted bevel uppermost along the line of the vein at an angle of around 20°. There is a distinctive ‘give’ as the vein is entered. Blood is aspirated into the syringe slowly to avoid haemolysis. The tourniquet is released and the needle withdrawn after a dry swab has been held to the site. Pressure should be applied by the patient or an assistant with the arm held straight or slightly elevated. The needle is removed from the syringe – not resheathed – and placed directly into a sharps container. The specimen is expelled gently from the syringe into the relevant bottles. Mixing with anticoagulant is best achieved by gently inverting the bottle several times – violent shaking will damage the sample. An adhesive plaster can be applied to the venepuncture site (check for allergy) when bleeding has stopped. Fig 52.1 Veins at the antecubital fossa.
Venepuncture and venous access
Taking a venous blood specimen (venepuncture)
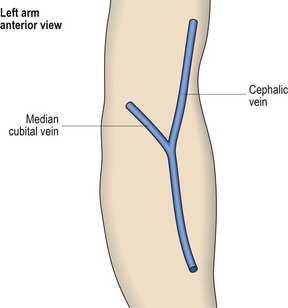
The median cubital vein is preferred for routine venepuncture.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Oncohema Key
Fastest Oncology & Hematology Insight Engine

