Urinary tract infections (UTIs) in women remain an important public health problem in the United States, affecting approximately 11 million women annually at a cost of $1.6 billion. Worldwide, an estimated 150 million UTIs occur each year, with an associated cost of more than $6 billion. As a result, UTIs are the most common bacterial infection in adult women and the most common medical complication of pregnancy (Box 14.1). UTI in women are divided into five categories: (i) young women with acute uncomplicated cystitis; (ii) young women with recurrent cystitis; (iii) young women with acute uncomplicated pyelonephritis; (iv) women of any age with complicated UTI; and (v) asymptomatic bacteriuria. UTIs are also important causes of nosocomial infections.
In women, UTIs are further classified into nonpregnant and pregnant. Distinction between these categories has major implications for antimicrobial treatment, pre- and post-treatment evaluation, and need for evaluation of the urinary tract.
EPIDEMIOLOGY
UTIs in nonpregnant and pregnant women are a frequent occurrence and source of morbidity and healthcare costs throughout a woman’s lifespan. UTIs account for an estimated 7 to 8 million office visits (mostly for cystitis) and more than 100,000 hospitalizations (mostly for acute pyelonephritis) annually in the United States. Approximately 50% to 60% of adult women report that they have had at least one UTI during their life. A large prospective study of young sexually active women in an HMO and a university study population demonstrated that the incidences of cystitis ranged from 0.5 to 0.7 per person per year. Based on national surveys estimating that over 50 million women (including adolescents) are sexually active, it has been suggested that many more millions of episodes of acute UTI occur annually than are reported on the basis of data obtained from surveys of office visits.
An estimated 25% to 30% of women who experience an episode of acute UTI will go on to develop recurrent infections. UTIs remain a common issue during the postmenopausal period with approximately 10% of postmenopausal women reporting having had a UTI within the past year.
Urinary tract infections are 14 times more common in females than in males. The increased risk for UTI in women is the result of (a) the short female urethra; (b) the external one third of the urethra is continuously contaminated by pathogens from the vagina and rectum; (c) women do not empty their bladder as completely as men; and (d) massage of bacteria into the bladder with sexual intercourse.
The introduction into clinical practice of quantitative urine culture by Kass revolutionized the concepts of the etiology, pathogenesis, and treatment of UTIs. This investigative work showed that significant bacteriuria can occur in the absence of clinical symptoms or signs of urinary tract infection and established quantitative microbiology as the indispensable laboratory aid for the diagnosis, follow-up, and confirmation of cure for urinary tract infection. Kass demonstrated that urinary bacterial counts on midstream voided urine specimens distinguished between contamination and infection with a high degree of accuracy.
There is a trend for an increasing prevalence of bacteriuria with increasing age. A significant increase in the rate of asymptomatic bacteriuria occurs following the onset of sexual activity, and the prevalence of bacteriuria in females rises at a rate of approximately 1% for each decade of life. The role of sexual intercourse as a precipitating factor for urinary tract infections is well recognized. An estimated two thirds of the acute episodes of urinary tract infection in young sexually active women are attributable to coitus. Fully 75% of UTI episodes in women with a history of recurrent urinary infections occurred within 24 hours of coitus. An inverse relationship between socioeconomic status and prevalence of bacteriuria is well documented. Table 14.1 summarizes the factors associated with the development of bacteriuria in women.
In a large, prospective study of sexually active young women, the risk factors for acquiring UTI were strongly and independently associated with recent sexual intercourse, recent use of a diaphragm with spermicide, and a history of recurrent UTI.
Additional risk factors have been addressed in specific groups of patients. Host factors associated with an increased risk for recurrent UTI in young women include (i) recent 1-month intercourse frequency; (ii) 12-month spermicide use; (iii) a new sex partner during the past year; (iv) age at first UTI ≤15 years; and (v) UTI history in the mother. These latter two predictors suggest that genetic and possibly long-term environmental exposures predispose to recurrent UTI. Whereas older studies demonstrated nonsecretors of blood group antigens were more prone to recurrent UTI, more recent investigations refute such an association.
Increased risk for postpartum UTI has been associated with African-American, Native American, or Hispanic raceethnicity, unmarried status, Cesarean delivery, tocolysis, maternal renal disease, and preeclampsia-eclampsia. In general, maternal conditions and procedures associated with an increased risk for UTI are those associated with urethral catheterization.
Factors contributing to UTIs in postmenopausal women have also been assessed. In postmenopausal women (50-70 years) the factors associated with UTI were (i) lack of estrogen; (ii) nonsecretor status; (iii) a history of UTI in the premenopausal period; (iv) urinary incontinence; (v) presence of a cystocele; and (vi) postvoid residual urine. Among older institutionalized women (>70 years), catheterization, urinary incontinence, antimicrobial exposure, and diminished mental status were most strongly related to risk of recurrent UTI. In part the increased susceptibility of postmenopausal women to UTIs is accounted for by a lack of estrogen, which results in an increase in vaginal pH, disappearance of lactobacilli from the vaginal flora and colonization of the vagina by Enterobacteriaceae, especially Escherichia coli. On the other hand, administration of topical estrogen has been shown to prevent recurrent UTI in postmenopausal women.
BOX 14.1 ▪ URINARY TRACT INFECTION
14 times more common in women
11 million women per year affected
Most common bacterial infection in women
Most common medical complication in pregnancy
Etiology
Most of the organisms responsible for urinary tract infections are considered part of the normal fecal and/or vaginal flora. E. coli is the etiologic agent in approximately 80% to 90% of acute infections. Other Gram-negative facultative bacteria such as Klebsiella, Proteus, Enterobacter, and Pseudomonas, and Gram-positive bacteria such as Staphylococcus saprophyticus, Group B streptococcus, and the Enterococcus are responsible for the remainder. Recently S. saprophyticus has been demonstrated to be the second most common cause of UTI in young sexually active women. In addition, Gardnerella vaginalis has been recognized as a urinary pathogen in women.
In patients who have received antibiotics, undergone urologic instrumentation, or have chronic recurrent infections, the causative organism is more likely to be Klebsiella, Enterobacter, Proteus, Pseudomonas, Serratia, or the Enterococcus.
TABLE 14.1 ▪ FACTORS ASSOCIATED WITH BACTERIURIA IN WOMEN
Sex: Bacteriuria 14 times more common in women
Age: Prevalence of bacteriuria increases 1% per decade of life
Sexual Activity:
Coitus facilitates movement of uropathogens from the introitus to the urethra
Socioeconomic status:
Prevalence of bacteriuria inversely related to socioeconomic status. Indigent women 2-3 times more likely to have bacteriuria.
Sickle cell trait/disease:
Associated with twofold increase in prevalence of bacteriuria.a
Pathogenic factors of bacteria:
fimbriae or pili (adherence), K antigen (antiphagocytic), hemolysin (cytotoxic), antimicrobial resistance (survival).
Diabetes mellitus
Immunosuppression
aSome investigators question that sickle cell trait associated with increased risk of bacteriuria.
PATHOGENESIS
The association between the enteric flora and urinary pathogens has led to the hypothesis that the mechanism of acquiring UTIs is by an ascending route of infection from the bowel to the vaginal vestibule and then to the urethra and ultimately the bladder. Women with recurrent bacteriuria have a higher incidence of colonization with Enterobacteriaceae between episodes than the vestibule of women without recurrent urinary tract infection. Moreover, E. coli adheres more readily to introital epithelial cells in women with recurrent urinary tract infection.
The presence of bacterial virulence factors provide a selective advantage and facilitate those strains of bacteria containing them for colonization of the urogenital tract and infection. Persistent rectal colonization with E. coli containing the adhesions P and F (i.e., P and F fimbriated E. coli) is significantly associated with persistent vaginal E. coli colonization with these same fimbriated organisms. However, persistent colonization with such E. coli is as common in women with and without recurrent UTI. Thus, while urovirulence factors (p- and Fadhesins) provide E. coli a selective advantage once it reaches the vaginal and bladder epithelium, additional factors such as spermicide exposure, sexual intercourse, voiding behavior, bacterial composition of the vaginal flora, and local immune factors play equally important roles in determining if an E. coli isolate colonizing the vaginal mucosa is eradicated or persists and enters the bladder to initiate the infectious process.
Colonization of the introitus with uropathogens is influenced to a large extent by the microbial ecosystem of the vagina. The normal vaginal microflora predominated by lactobacilli and the associated acidic pH of the vagina prevent establishment of prolonged colonization of the vaginal introitus with uropathogenic E. coli. Factors that can alter the normal vaginal microflora in such a manner to predispose to E. coli colonization and increase the risk of acute uncomplicated cystitis are (i) diaphragm/spermicide use; (ii) antimicrobial exposure; and (iii) lack of estrogen (e.g., postmenopausal).
The active component of spermicides, nonoxynol-9, is an active microbicide against many lactobacilli (especially hydrogenperoxide producing strains) and Gardnerella vaginalis while E. coli and other pathogens are highly resistant. In addition, nonoxynol-9 enhanced adherence of E. coli to vaginal epithelial cells. Thus, spermicidal use appears to provide a selective advantage in colonizing the vagina with uropathogens such as E. coli. Many antimicrobial agents, especially the β-lactams (penicillins and cephalosporins), have an adverse effect on the normal vaginal flora and facilitate colonization with E. coli and other uropathogens. In postmenopausal women lack of estrogen is associated with markedly reduced lactobacillus colonization, an increased vaginal pH, and an increased E. coli colonization of the vagina. As a result the risk of acute uncomplicated UTI is increased 10-fold in postmenopausal women not receiving hormone replacement therapy.
Studies have demonstrated that the E. coli strains causing acute UTIs comprise a unique group of uropathogens defined by O:K:H serotype and possessing virulence determinants that enable these microorganisms to colonize and infect the urinary tract. These virulence factors include adherence factors (P, type 1, S, Dr fimbriae), toxins (LPS, hemolysin), aerobactin, invasion factors, and serum resistance.
The most important of these virulence determinants are P. fimbriae, which mediate specific binding of E. coli to receptors on uroepithelial cells. It has been demonstrated that certain strains of E. coli, which commonly express P fimbriae are more commonly isolated from the urine of patients with acute pyelonephritis than those with acute cystitis or asymptomatic bacteriuria. In addition, while only 10% to 20% of fecal strains of E. coli possess P fimbriae approximately 50% to 60% of strains associated with acute cystitis possess P fimbriae. P fimbriae are believed to facilitate ascent of E. coli to the upper urinary tract and also enhance the inflammatory response in the urinary tract to E. coli resulting in secretion of significantly more IL-6 than seen with non-fimbriated strains.
Following spread to the urinary tract, uropathogenic clones of E. coli (and other uropathogens) overcome local host defenses such as urine flow, secreted receptor analogues, which trap fimbriated bacteria, and bactericidal molecules in the urine and mucosa. Once these defenses are bypassed, uropathogenic bacteria target the mucosa of the urinary tract where they elicit an inflammatory response in which cytokines and proinflammatory factors are produced. As a result, fever and the acute phase response may occur. Release of chemotactic cytokines (e.g., interleukin 8 [IL-8]) recruits polymorphonuclear granulocytes to the mucosal surface, which in turn clear bacteriuria. In acute pyelonephritis, approximately 30% of patients develop bacteremia secondary to bacterial invasion through the mucosa into the bloodstream. The localization and magnitude of the inflammatory response elicited determines the clinical presentation of UTIs. For instance, in acute pyelonephritis inflammation of the kidney occurs in association with generalized signs of inflammation such as fever and leukocytosis.
The pathogenesis of acute cystitis and asymptomatic bacteriuria is less well delineated. There are no bacterial virulence factors that identify strains of E. coli associated with cystitis. While asymptomatic bacteriuria (ASB) may be associated with local inflammation in the bladder, the magnitude of the inflammatory response is insufficient to produce symptoms.
It is estimated that approximately 25% to 30% of women with acute cystitis subsequently develop recurrences. In the past it was believed that over 90% of recurrences in young women were episodes of exogenous reinfection. More recently, it has been suggested that the majority of these recurrences are the result of a single infecting E. coli strain, even over a long period of time. Most likely this occurs secondary to persistent E. coli in the vagina and feces despite eradication of the organism from the urinary tract. Only rarely are anatomic or functional abnormalities of the urinary tract responsible for recurrent UTIs. The E. coli strains causing recurrent UTI do not have urovirulence determinants that differ from those associated with acute episodes of cystitis. Similarly, no host defense differences have been demonstrated in patients with recurrent vs. acute UTI. On the other hand genetic differences among patients may play a role in the pathogenesis of recurrent UTI.
Table 14.2 lists the antimicrobial host defenses in the urinary tract of women. Normal urine contains several components that are inhibitory for bacteria, including urea, organic acids, high pH, and low osmolality. On the other hand, the growth of E. coli is facilitated by glucosuria and the lower urine pH during pregnancy. Micturition and efficient bladder emptying are major defense mechanisms against developing UTI. Bladder mucosa contains intrinsic antibacterial activity, probably secondary to production of bactericidal molecules by epithelial cells (defensins). Sig A diminishes attachment of bacteria to uroepithelial cells. In addition, urine contains several molecules that are soluble receptor analogs that act as competitive inhibitors of adherence of uropathogens to epithelial cells. These molecules include (i) Tamm-Horsfall Protein (THP); (ii) mucopolysaccharide lining the bladder plays an important role in preventing bacterial attachment to the bladder mucosa; and (iii) a variety of low molecular weight oligosaccharides that are potent inhibitors of E. coli adherence.
TABLE 14.2 ▪ ANTIBACTERIAL HOST DEFENSES IN THE URINARY TRACT OF WOMEN
Similar to other anatomic sites, bacteria cause an inflammatory response in the urinary tract, which is site-specific. Thus, in acute cystitis a localized inflammatory response occurs, whereas in acute pyelonephritis both localized and systemic inflammatory responses are seen. Following adherence to uroepithelial cells, bacteria induce a mucosal inflammatory response in which PMNs infiltrate into the mucosa and ultimately the urine. The primary role of these PMNs is to limit tissue invasion. As part of the inflammatory response cytokines are elaborated in response to bacterial adhesion by uroepithelial cells. IL-6 production is most prominent, but IL-1 and IL-1B are also present.
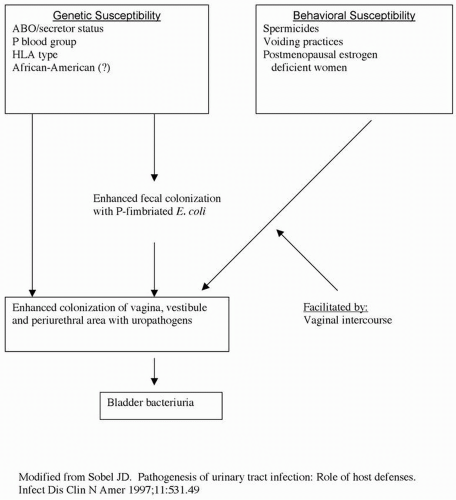
Certain host factors have been identified that predispose to UTIs. These include obstruction to urine flow, diabetes mellitus, and aging. However, most symptomatic lower (cystitis) and upper (pyelonephritis) UTIs in healthy adult women occur in the absence of structural or functional abnormalities of the urinary tract. A model based on these host factors provides a concept of the pathogenesis of UTI in women (Fig. 14.1). In this model, genetic factors lead to increased susceptibility for fecal colonization with P-fimbriated E. coli. In turn this results in enhanced colonization of the vagina, vestibule, and periurethral area with uropathogens. Behavioral risk factors (e.g., spermicide use, infrequent voiding, estrogen deficiency) also enhance uropathogen colonization of the vagina, vestibule, and periurethral areas. Last, vaginal intercourse facilitates the ascension of uropathogens to cause bladder bacteriuria.
DIAGNOSIS
While molecular diagnostic tests have been widely used in the diagnosis of many infections, the approach to the diagnosis of UTIs still relies on urine culture. Thus, the absolute criterion for the diagnosis of UTI is microbiologic confirmation of pathogenic bacteria in the urinary tract. The presence of pyuria suggests infection but is not diagnostic of UTI.
Asymptomatic bacteriuria is diagnosed on the basis of quantitative cultures in midstream clean-voided urine specimens obtained from asymptomatic patients. Bacteriuria was traditionally defined as the presence of ≥105 colony forming units per milliliter of urine from two consecutive first void clean-catch urine specimens. In clinical practice a single positive culture suffices. Less stringent diagnostic criteria have more recently been proposed for uncomplicated UTI in acutely dysuric females (acute cystitis). Approximately 30% to 50% of patients with acute lower tract infection characterized by dysuria, urgency, and frequency do not meet the ≥105 bacteria/ml criterion for infection but have pathogenic aerobic Gram-negative bacilli present with suprapubic taps. A diagnostic criterion of ≥102 bacteria per ml has a sensitivity of 95%, specificity of 85%, and a high positive predictive value of 88% among symptomatic women. It has been suggested that the most efficient approach for the diagnosis of symptomatic UTIs is to use rapid screening tests for pyuria to guide dual culturing method to detect 102 CFU/mL plus standard culture for specimens without pyuria. Alternatively, The Infectious Diseases Society of America provided consensus definitions for use in antimicrobial treatment studies. For acute cystitis they recommended ≥103 CFU per mL (sensitivity 80% and specificity 90%) and for pyelonephritis ≥104 CFU/mL (sensitivity, 90%-95%). These concentrations were chosen over ≥102 CFU/ml because the greater concentrations can be identified by standard microbiologic techniques in most clinical laboratories.
FIGURE 14.1 Host factors in the pathogenesis of UTI in women.
Once a sample of urine is obtained to confirm a diagnosis of UTI, the specimen must be rapidly brought to the microbiology laboratory or refrigerated. A delay of greater than 2 hours will result in an erroneous high bacterial count. The urine should be cultured on blood agar as well as deoxycholate, eosin-methylene, or MacConkey agar for Gram-negative rods. Quantitation of bacteria can be accomplished by means of standard dilutions, using either the pour plate or the streak spread plate techniques.
Many clinicians have been reluctant to test all symptomatic patients or to screen all pregnant patients for bacteriuria by culture methods because of the cost. As a result, office-based screening for bacteriuria has been suggested as an alternative to using quantitative urine cultures. However, when compared with quantitative cultures, such office screening systems correctly predicted only 62.5% to 87.5% of bacteriuria. Moreover, in pregnant women, these tests are associated with unacceptably high false-positive and false-negative results.
In symptomatic patients, frequency, urgency, dysuria are usually associated with cystitis, whereas fever, chills, and flank pain are additionally associated with pyelonephritis. However, these signs and symptoms are not specific for the localizing site of infection (i.e., bladder or kidney). Comparison of the clinical features of asymptomatic and symptomatic UTIs is presented in Table 14.3.
While classic teaching described the ascending route as the most frequent for UTIs, it has also been shown that the upper urinary tract may be the source of bacteriuria in many women. Various methodologies have been used in the localization of UTIs. Direct methods include ureteric catheterization for culture. However, most investigators have relied on indirect methods to detect a renal source. The role of antibody-coated bacteria in localization of urinary tract infection site has received the most attention. Bacteria from the kidney are coated with antibody, whereas organisms limited to the bladder or urethra are not. In general, 40% to 50% of bacteriuria is believed to be of renal origin. However, use of the antibodycoated test has not received widespread clinical use and is chiefly utilized in research studies.
TABLE 14.3 ▪ CLINICAL MANIFESTATIONS AND LABORATORY ABNORMALITIES IN URINARY TRACT INFECTIONS
UTI
Clinical Manifestations
Pyuria
Bacteriuria
White Blood Cell Casts
Leukocytosis
Urine Culture (CFU/mL)
Asymptomatic Bacteriuria
None
+
+
−
−
>105 (clean catch)
Acute cystitis
Frequency, urgency, dysuria
+
+
−
−
>102 (catheterized) or >105 (clean catch)
Acute pyelonephritis
Frequency, urgency, dysuria plus fever, chills, flank pain, CVA tenderness
+
+
+
+
>102 (catheterized) or >105 (clean catch)
SYMPTOMATIC UTIs IN NONPREGNANT WOMEN
Acute Uncomplicated Cystitis in Young Women
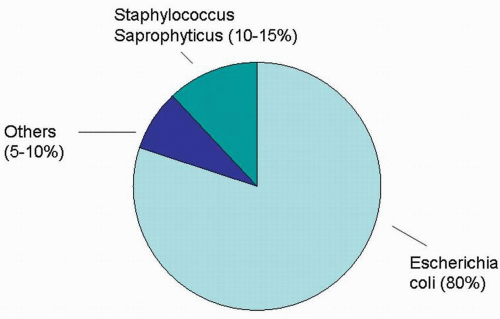
A narrow spectrum of microorganisms are involved in the etiology of acute uncomplicated cystitis (Fig. 14.2).E. coli accounts for 80%, Staphylococcus saprophyticus for 10% to 15%, and other organisms such as Klebsiella species and Proteus mirabilis 5% to 10%. In addition, these etiologic agents have reasonably predictable antimicrobial susceptibility profiles. Risk factors for the development of acute uncomplicated UTI have been identified, including sexual intercourse, use of a diaphragm and spermicide, spermicide alone, delayed post coital micturition, history of recent urinary infection, and use of selected antimicrobials that alter the normal vaginal flora (Table 14.4).
FIGURE 14.2 Etiology of acute uncomplicated cystitis in young women.
DIAGNOSIS
Women with acute uncomplicated cystitis typically present with dysuria. However, acute dysuria may be caused by three different types of infection: (i) acute cystitis caused by Enterobacteriaceae, especially E. coli; (ii) acute urethritis caused by Chlamydia trachomatis or Neisseria gonorrhoeae; and (iii) Vaginitis caused by Candida or Trichomonas vaginalis. Table 14.5 summarizes the approach to differentiating these causes of dysuria based on presenting symptoms, signs, and urinalysis results.
Traditionally, the diagnosis of acute uncomplicated cystitis was based on detecting 102 to ≥105 colonies per ml of a uropathogen in a clean catch midstream urine specimen. However, current recommendations advocate establishing the diagnosis of acute uncomplicated cystitis with an abbreviated laboratory workup. In young women with typical symptoms (dysuria, urgency, and frequency), a diagnosis of acute cystitis is presumed if pyuria is present on leukocyte esterase dip stick testing or microscopy and urine culture is not necessary (Box 14.2). The presence of dysuria and frequency in the absence of vaginal discharge or irritation is associated with a UTI in >90% of instances. Evaluating a midstream urine specimen for pyuria is the single most important laboratory test for acute cystitis. Pyuria is present in nearly all women with acute cystitis. While examination of an unspun urine specimen is the most acute method for detecting pyuria (≥10 leukocytes per mL), use of dipstick testing for leukocyte esterase is the most frequent method used clinically. The leukocyte esterase test has a sensitivity of 75% to 96% and specificity of 94% to 98% in detecting >10 leukocytes per HPF. Another commercially available dipstick test is the nitrite test, which is fairly sensitive and specific for detecting ≥105 CFU of Enterobacteriaceae per mL. However, it does not detect Gram-positive pathogens nor low count UTIs. In general, microscopy to detect bacteriuria is not recommended because ≤104 CFU/mL of bacteria are difficult to see even on a spun specimen. An alternative approach is to exclude any laboratory testing and treat empirically for acute cystitis based only on the presence of typical symptoms.
TABLE 14.4 ▪ RISK FACTORS FOR ACUTE UNCOMPLICATED CYSTITIS IN WOMEN
Sexual intercourse
Diaphragm and spermicide use
Spermicide alone
Delayed post coital micturition
History of recent UTI
Use of selected antimicrobial agents
TABLE 14.5 ▪ DIFFERENTIAL DIAGNOSIS OF ACUTE DYSURIA IN YOUNG WOMENa
Diagnosis
Pathogens
Pyuria
Hematuria
Urine Culture (CFU/mL)
Symptoms
Signs
Cystitis
E. coli S. saprophyticus Proteus spp. Klebsiella spp.
+
±
102 to ≥105
Abrupt onset, severe multiple symptoms (dysuria, frequency and urgency), suprapubic or low back pain
Suprapubic tenderness
Urethritis
C. trachomatis N. gonorrhoeae Herpes simplex
+
−
<102
Gradual onset, mild symptoms, vaginal discharge or bleeding, lower abdominal pain, new sex partner
Cervicitis or vulvovaginal herpetic lesions
Vaginitis
Candida spp. Trichomonas vaginalis
−
−
<102
Vaginal discharge or odor, pruritus, dyspareunia, external dysuria, no frequency or urgency
Vulvovaginitis on exam
aModified from Reference 1, Table 1.
If pyuria is absent in the face of typical symptoms suggestive of acute cystitis or mitigating clinical circumstances (Table 14.6) are present, a culture should be obtained (Box 14.3). Of note for providers of maternity care, pregnant women are among those in whom culture is recommended.
TREATMENT
Identification of the optimal treatment for uncomplicated acute cystitis in young women has been a controversial issue. The traditional approach of a 7- to 10-day antimicrobial regimen was challenged and subsequently single dose therapy also has been challenged. Current recommendations focus on use of a 3-day regimen of antimicrobial therapy for treatment of acute uncomplicated cystitis in young nonpregnant women. The advantages and disadvantages of varying lengths of antimicrobial treatment for acute uncomplicated cystitis are summarized in Table 14.7. For most antimicrobial agents, a 3-day regimen appears to be optimal with efficacy similar to 7-day regimens and fewer side effects and lower cost. Singledose therapy results in lower cure rates and more frequent recurrences, especially with amoxicillin or oral cephalosporins, while 7-day regimens are no more effective than 3-day courses and increase cost and side effects.
BOX 14.2 ▪ DIAGNOSIS OF ACUTE UNCOMPLICATED CYSTITIS
Presence of typical symptoms (dysuria, frequency, and urgency)
Pyuria detected by leukocyte esterase dipstick or microscopy
A recent large meta-analysis demonstrated that antibiotic therapy for 3 days is similar to prolonged therapy in achieving symptomatic cure for acute cystitis. However, prolonged treatment was more effective in obtaining bacteriologic cure. Adverse events were more common in the prolonged therapy group. Seven-day regimens should be reserved for use in patients with mitigating factors that are associated with lower cure rates when 3-day regimens are used (Table 14.8). Of note, pregnancy is one of these factors.
In the United States increasing resistance to some of the antimicrobial agents frequently used for the treatment of acute uncomplicated cystitis has occurred (Fig. 14.3). One third of bacterial strains causing community acquired acute uncomplicated cystitis are resistant to amoxicillin and sulfonamides. While the prevalence of resistance to nitrofurantoin among E. coli is <5%, approximately 15% to 20% of other uropathogens are resistant to nitrofurantoin. An increasing prevalence of resistance to uropathogens is being seen with trimethoprim and/or trimethoprim-sulfamethoxazole (TMPSMX); this varies geographically and ranges from 10% to 22%. The increase in resistance to TMP-SMX is cause for great concern. The most important risk factor for TMP-SMX resistance in women is the use of TMP-SMX within the last 3 months or the use of any other antimicrobial agent. On the other hand, resistance to fluoroquinolones generally is low and remains <5%. In general, S. saprophyticus is much less resistant to antimicrobial agents recommended for the treatment of acute uncomplicated cystitis. Approximately 3% are resistant to TMP-SMX, 0% to nitrofurantoin, and <0.5% to ciprofloxacin. However, 15% of S. saprophyticus are resistant to ampicillin.
TABLE 14.6 ▪ CLINICAL CIRCUMSTANCES THAT WARRANT INITIAL URINE CULTURE IN PATIENTS WITH SYMPTOMS OF ACUTE CYSTITIS
Pregnancy
Diabetes
Symptoms >7 days
Recent urinary tract infection
Age >65 years
BOX 14.3 ▪ URINE CULTURE INDICATED IN WOMEN
With Apparent Acute Cystitis if:
Patient is suspected of having a complicated infection
Symptoms are not characteristic of UTI
Patient has persistent symptoms of UTI following treatment and a new antibiotic regimen is to be started
UTI symptoms recur <1 month after treatment of previous UTI for which no culture was performed and a new antibiotic regimen is to be started
The impact of antimicrobial therapy on the vaginal flora also plays a role in eradicating bacteriuria. Trimethoprimsulfamethoxazole is present in vaginal secretions in high concentrations, which eradicate E. coli but have minimal effect on the normal vaginal flora, especially lactobacilli and anaerobic bacteria. When used in multiday regimens, β-lactams have a high likelihood of altering the vaginal flora by eradicating lactobacilli and predisposing patients to recurrent UTIs. Shown in Table 14.9 are the relative benefits and drawbacks to varying durations of antimicrobial therapy for acute cystitis. Clearly the 3-day regimen maximizes the efficacy and minimizes adverse effects.
In 1999, the Infectious Diseases Society of America (IDSA) published evidence-based guidelines for antimicrobial treatment of uncomplicated acute bacterial cystitis (Box 14.4). In summary they noted that in otherwise healthy adult nonpregnant women with acute uncomplicated cystitis, single-dose therapy is generally less effective than the same antimicrobial used for longer durations (A, I.). Most antimicrobials given for 3 days are as effective as the same antimicrobial given for a longer duration (A, I.). Trimethoprim-sulfamethoxazole for 3 days is considered the current standard therapy (A, I) (Box 14.5). Trimethoprim alone (A, II) and Ofloxacin (A, I) are equivalent to trimethoprim-sulfamethoxazole; other fluoroquinolones (e.g. norfloxacin, Ciprofloxacin, fleroxacin) are probably of similar effectiveness (A, II). However, because fluoroquinolones are more expensive and to postpone emergence of resistance to these drugs, fluoroquinolones are not recommended as initial empirical therapy for acute uncomplicated cystitis except in communities with high rates or resistance (> 10%-20%) to trimethoprim-sulfamethoxazole among uropathogens (Box 14.6). When given for 3 days, β-lactam antimicrobials are less effective than trimethoprim-sulfamethoxazole or fluoroquinolones (E, I). Nitrofurantoin and fosfomycin may become more useful as resistance to other agents increase (B, I). Nitrofurantoin generally demonstrates a low level of resistance among E. coli, Gram-positive cocci (including Enterococcus faecalis) and many Gram-negative bacteria. However, nitrofurantoin is not active against Proteus species, and some Enterobacter and Klebsiella strains. Table 14.10 provides the recommended 3-day regimens for the treatment of acute uncomplicated cystitis. A recent analysis assessing how often the 1999 IDSA guidelines’ recommended treatment regimen (i.e., the use of TMP-SMX) was followed, showed that TMP-SMX was not the agent preferred by healthcare providers overall and its use did not increase following publication of the guidelines. Rather, ciprofloxacin was used more often for the treatment of acute uncomplicated cystitis.
TABLE 14.7 ▪ COMPARISON OF ANTIMICROBIAL REGIMENS OF VARYING LENGTH FOR TREATMENT OF ACUTE UNCOMPLICATED CYSTITIS IN YOUNG WOMEN
bPregnancy, diabetes, symptoms >7 days, recent UTI, or age >65 years.
TABLE 14.8 ▪ PATIENTS IN WHOM SEVEN-DAY REGIMENS OF ANTIMICROBIAL THERAPY ARE RECOMMENDED FOR THE TREATMENT OF ACUTE CYSTITIS
Pregnancy
Diabetes
Symptoms for >7 days
Recent UTI
Diaphragm/spermicide use
Age >65 years
Routine post-treatment test of cure culture is not recommended with acute uncomplicated cystitis. The costs to detect cases of asymptomatic bacteriuria are considerable and the benefit of detecting and treating ASB in healthy women has only been demonstrated in pregnancy and prior to urologic surgery or instrumentation. When symptoms do not resolve or recur within 2 weeks of treatment a urine culture and susceptibility testing should be performed. Retreatment is based on the results and a 7-day course of therapy initiated.
Only gold members can continue reading. Log In or Register to continue