After hemostasis is established in an injured vessel, a highly orchestrated process follows to heal the vessel and to reestablish blood flow. To a large extent, this process is mediated through locally controlled fibrinolysis by activation of the plasminogen-plasmin enzyme system (see Chapters 20 and 21). Briefly, plasminogen binds to lysine residues on fibrin and is converted to plasmin by plasminogen activators (PAs) released by endothelial cells, through cleavage of the heavy chain at Arg560-Val561.1 Trace amounts of plasmin liberate an amino-terminal 76-residue portion of plasminogen,2 converting glu-plasminogen to lys-plasminogen, which binds to fibrin more efficiently3 and is more sensitive to PA activation,4,5,6 thereby promoting further conversion of plasminogen to plasmin.7,8 Just as coagulation inhibitors such as antithrombin and tissue factor pathway inhibitor limit the initial hemostatic process to the site of vessel injury, fibrinolytic inhibitors such as plasminogen activator inhibitors, α2-antiplasmin, and α2-macroglobulin contain the fibrinolytic reaction to the site of injury.
Antifibrinolytic agents (AFs) are best viewed as prohemostatic drugs that act in two situations. The first is to prevent bleeding caused by an excess of plasmin activity (see FIGURE 77.1), such as in the setting of primary menorrhagia.9,10 The second situation is to retard physiologic fibrinolysis following slow or ineffective hemostasis (see FIGURE 77.1), such as may occur in a hemophiliac.11,12 AFs may improve hemostasis in a wide variety of bleeding states, reducing blood loss and transfusion. Useful properties of AFs are ready whole body distribution following oral or intravenous administration, potent inhibition of plasmin, and no associated tachyphylaxis. When used appropriately to diminish an exuberant fibrinolytic response, these agents do not induce or potentiate coagulation. Thus, lower levels of D-dimer were present in patients treated with ε-aminocaproic acid (EACA) (vs. placebo) before, during, and after cardiac surgery, demonstrating inhibition of fibrinolysis, but levels of thrombin-antithrombin complexes and soluble fibrin were the same as in placebo-treated patients, indicating no activation of coagulation.13 However, AF agents have the potential to unmask subclinical thrombosis, such as in a patient with unrecognized, compensated, disseminated intravascular coagulation (DIC) (see Chapter 98).
There are three distinct clinical situations in which antifibrinolytic therapy has been proven to be useful: (a) systemic hyperfibrinolysis, (b) hypocoagulability, and (c) localized lesions in the absence of systemic hyperfibrinolysis or hypocoagulability.14,15,16,17 The field has undergone a sea change due to two significant circumstances:
Withdrawal of the preeminent AF agent, aprotinin, from the market due to evidence of increased mortality following its use
The expansion of the indications for AF agents to the treatment of trauma-induced hemorrhage, an indication that will likely dramatically increase the number of patients treated
MODE OF ACTION OF ANTIFIBRINOLYTIC AGENTS
The AF agents fall into three categories:
Natural plasma inhibitors of plasmin and of PAs,18,19 which are not the subject of this chapter (see Chapter 21)
Synthetic lysine analogs, such as trans-p-aminomethylcyclohexane carboxylic acid (tranexamic acid, TXA) and 6-aminohexanoic acid (EACA)21,22,23,24
Aprotinin (Trasylol, bovine pancreatic trypsin inhibitor), a 58-residue polypeptide (Mr = 6,500) isolated from bovine lung, parotid gland, or pancreas,20 is a dose-dependent inhibitor of plasmin17 and at higher concentrations of other serine proteases (trypsin, kallikrein, chymotrypsin).14,16,17 Recent studies show an increased risk for death and renal failure after treatment with aprotinin, so this drug is no longer marketed for use in the United States or Europe, although it remains available for research.
Biochemistry
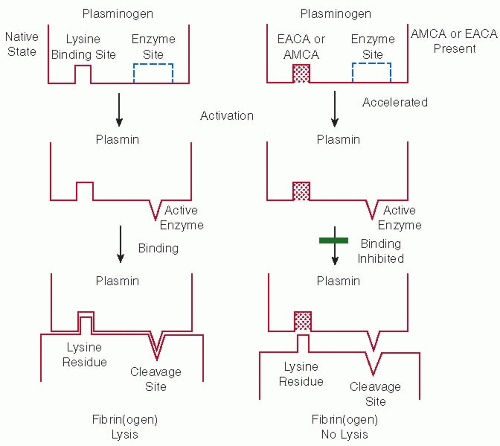
The lysine analogs (TXA and EACA) prevent excessive plasmin formation by occupying plasminogen’s lysine-binding site (LBS) for fibrin, thereby precluding plasminogen localization to fibrin for activation by PA (see FIGURE 77.2). Lysine analogs also bind to tissue plasminogen activator (tPA) kringles, interfering with plasminogen activation.18,21In vitro, these agents bind to the LBS of plasminogen, resulting in a conformational change that may actually accelerate activation,19,21,22,25 and binding to plasmin kringles reduces the binding by plasmin inhibitors, which could theoretically increase fibrinolytic activity.26,27 Yet, the major action of these compounds in vivo is antifibrinolytic, primarily by blocking the association of plasminogen and tPA on the fibrin surface.28,29 Although plasmin may still be generated, fibrinolysis is prevented.
The seemingly disparate effects may be explained by the two-step process required for binding of plasminogen to fibrin (see FIGURE 77.2). Plasminogen is activated by proteolytic cleavage that exposes the serine-histidine catalytic site, a cleavage that also promotes binding to fibrin30 between LBSs on plasminogen and lysine residues on fibrin. Without proper binding, proteolysis cannot proceed. This two-step requirement explains the seeming discrepancy of in vivo inhibition29,31,32,33,34,35,36 and in vitro activation.22,25,26,27,28,29,30,31,32,33,34,35,36,37,38In vitro, EACA and TXA accelerate plasminogen activation by altering plasminogen’s conformation and making it more susceptible to proteolytic action by activators. However, lysis of a fibrin substrate is inhibited because the same binding phenomenon also blocks the LBS. Therefore, plasmin may be produced, even rapidly, but without binding to fibrin; there is no proteolytic fibrinolysis by the serine enzyme site.
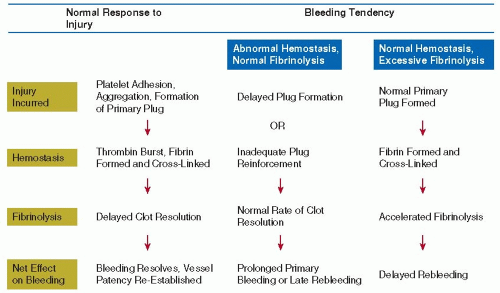
FIGURE 77.1 Schematic of body’s hemostatic response to vascular injury and effect of imbalances between hemostasis and fibrinolysis. Under physiologic conditions, when an injury is incurred, hemostasis proceeds culminating in fibrin generation and reinforcement of the platelet plug, followed by delayed clot resolution through fibrinolysis. A bleeding tendency arises when either arm is disrupted. If hemostasis is inadequate, normal fibrinolysis will occur and cause premature clot resolution with bleeding. As well, if hemostasis is normal, yet balanced by enhanced fibrinolysis, a clot will dissolve prematurely and result in bleeding.
FIGURE 77.2 Schematic diagram of the in vitro mode of action of synthetic lysine analogs on plasminogen activation and plasmin proteolysis of fibrin(ogen). ε-aminocaproic acid (EACA) and trans-p-aminomethyl-cyclohe×ane carboly×ic acid (T×A) accelerate plasminogen activation by inducing a conformational change in the molecule; however, they inhibit fibrinolysis by blocking the lysine binding site necessary for the binding of plasmin(ogen) to its substrate. Therefore, even though plasmin may be rapidly formed, it cannot reach the fibrin substrate because its binding site is occupied by the synthetic inhibitor. The accelerated activation as shown in the figure is from the in vitro experiments; it remains to be demonstrated in vivo.
EACA and TXA are structurally similar to lysine and inhibit the interaction between fibrinogen lysine residues and plasminogen LBSs, especially those located on kringle 1.39,40,41,42 Subtle differences in the synthetic analogs markedly affect their inhibitory potential, as exemplified by the approximately 6- to 10-fold higher molar potency of TXA in comparison with EACA43 and the ineffectiveness of the cis form of TXA in comparison with the trans form.43 Other active analogs of lysine include p-amino methylbenzoic acid and 4-amino ethylbicyclo-[2.2.2]-octane-1-carboxylic acid, which are 5- to 10-fold and 100-fold, respectively, more potent than EACA.44
Aprotinin is a nonspecific serine protease inhibitor of the Kunitz family. Its active residue, 15-lysine, binds reversibly to its target’s catalytic site and inhibits numerous serine proteases, including trypsin, plasmin, chymotrypsin, kallikrein, elastase, urokinase, and thrombin.17In vivo, aprotinin binds directly to plasmin at 137 kallikrein inhibitor units (KIU) per mL, whereas it binds to kallikrein at >250 KIU per mL. Side chain Lys15 of aprotinin binds to the aspartate side chain in the specificity pocket of plasmin. Aprotinin blocks activation of protease-activated receptor-1 on platelets, preventing thrombin-induced platelet aggregation, a mechanism thought to be particularly important in the platelet dysfunction acquired during exposure to cardiopulmonary bypass circuits.45 Aprotinin inhibits the inflammatory cascade at multiple levels, protects against kallikrein-induced generation of bradykinin, decreases neutrophil degranulation and extravasation at inflammatory sites, decreases expression of proinflammatory glycoproteins (CD11b) on neutrophils, and attenuates complement generation.46,47
Pharmacology
TXA and EACA are rapidly absorbed from the gastrointestinal (GI) tract, allowing oral or intravenous administration,48,49,50 with peak plasma levels at 1 to 2 hours after oral dosing. Elimination is primarily via renal excretion and metabolism, approximately 65% excreted in the urine unchanged and 10% as an inactive metabolite, adipic acid. Approximately 85% of an intravenous dose is cleared within 3 hours, but because EACA penetrates the entire extravascular space, urinary excretion may be detected for 12 to 36 hours.49 The drugs cross the blood-brain barrier,51 enter joint fluid and synovial membranes,52 are excreted at low levels into breast milk, and pass through the placenta.53
The recommended dose for EACA has been derived from in vitro studies and shown to be effective for the treatment of hyperfibrinolytic states; however, the minimal dose required to inhibit normal or enhanced local fibrinolysis is not known. EACA is usually administered as an intravenous priming dose of 0.1 g/kg over 20 to 30 minutes, followed by a continuous infusion of 0.5 to 1 g/h or an equivalent intermittent dose every 1, 2, or 4 hours, generally until acute bleeding is controlled.35 Continuous intravenous infusion of 0.5 g/h may be a useful regimen for serious acute bleeding (personal observation). Plasma levels of at least 0.001 M (13 mg/100 mL) are adequate to inhibit in vivo fibrinolysis.29,33,43,54 Urinary concentration is generally 75- to 100-fold higher than plasma49; therefore, much lower doses may be used to control urinary tract bleeding (3 g EACA per day). As renal clearance approximates endogenous creatinine clearance,48 patients with renal insufficiency should have their doses reduced according to creatinine clearance.
The serum half-life of TXA is similar to EACA, 1 to 2 hours, and it is also rapidly excreted unchanged in the urine, more than 90% in 24 hours.50,55 Compared with EACA, TXA is much more potent, inhibiting fibrinolysis at much lower plasma concentrations, with inhibitory effect lasting for 7 to 8 hours. The recommended oral dose is 25 mg/kg, three times daily. Intravenous infusion is delivered at a dose of 10 mg/kg, three times per day, or if used for surgical prophylaxis of bleeding, 10 mg/kg loading dose followed by continuous infusion of 1 mg/kg/h. Although studies with aprotinin have demonstrated a clear dose-response curve with regard to reduction in fibrinolytic bleeding, assessment of a dose response among lysine analogs is limited by a lack of randomized, placebo-controlled trials.56
Unlike the orally bioavailable lysine analogs, aprotinin must be administered parenterally. Following its distribution phase, the plasma half-life of aprotinin is 150 minutes, and its terminal half-life is 5 to 10 hours. Aprotinin is primarily reabsorbed in the proximal tubules, with only approximately 10% excreted unchanged in the urine. Ultimately, the drug is taken up by tubular endothelium, stored in phagolysosomes, and slowly degraded by lysosomal enzymes.20 Aprotinin dosing is measured as KIU, or the amount of aprotinin to decrease two biologic units of kallikrein activity by 50%. Aprotinin is associated with a risk for anaphylaxis, so an intravenous test dose of 10,000 KIU must be given to exclude hypersensitivity at least 10 minutes prior to the loading dose.20 Clinically significant decreases in surgical blood loss and transfusion requirements correlate with higher doses of aprotinin.57,58,59,60
Side Effects and Complications
EACA and TXA are associated with nasal stuffiness, conjunctival injection, skin rash, and dose-related GI discomfort, including nausea, vomiting, and diarrhea.35,50 A literature review of EACA use between 1972 and 199561 found 33 cases of clinically significant myopathy, notably with prolonged administration of high doses (16 to 36 g/d for >28 days) and that patients recovered after discontinuing the medication.
Aprotinin, a bovine-derived protein, is associated with hypersensitivity reactions, including skin eruption, pruritus, dyspnea, and fatal anaphylactic shock in 0.3% to 0.6%.56 Although exceedingly rare with first exposure, the incidence of anaphylaxis may be as high as 2.7% upon second exposure.62 A pretreatment test dose must be given to exclude those at risk for hypersensitivity, although anaphylaxis has occurred following a nonreactive test dose.62 Efforts to decrease incidence of anaphylactic shock have not proven effective. Aprotinin is associated with dose-related renal dysfunction and increased need for dialysis,63,64 with higher risks in patients with baseline renal impairment or those taking renal toxic medications. When combined with off-pump bypass surgery and angiotensin converting enzyme inhibitor (ACEI) use, aprotinin nearly tripled the risk for postoperative renal dysfunction.65 Additional side effects of aprotinin include vasodilation, generally transient and preventable with slow drug administration, and prolongation of the partial thromboplastin time and activated clotting time due to inhibition of the intrinsic clotting cascade.
Serious systemic thrombotic complications have been reported following the use of antifibrinolytic therapy, although these complications are most clearly associated with a concurrent thrombogenic stimulus, and case reports of devastating, systemic thrombotic episodes following antifibrinolytic therapy are reported,61,62,63,64,65,66,67,68,69,70,71,72,73 generally in association with conditions predisposing to coagulopathy. Central venous catheter thrombosis may occur more commonly following antifibrinolytic therapy,74,75,76,77 and prophylactic antifibrinolytic therapy used during joint replacement or prostate surgery is associated with an increased risk of venous thrombosis.60,78,79 Lysine analogs have been used successfully to treat postpartum hemorrhage and hemorrhage associated with abruptio placentae, and a retrospective analysis of 2,102 pregnant women showed only 2 of 256 TXA-treated patients versus 4 of 1,846 matched controls developed thrombotic complications,80 and the authors concluded that there was no thrombogenic effect of TXA in this high-risk group. Clots in the urinary tract have been noted following AF therapy in hemophilic and hemoglobinopathy patients with active genitourinary bleeding, explained as inhibition of urokinase allowing the generation of lysis-resistant clots.81,82,83,84,85,86,87,88,89,90,91,92,93 AF therapy is best reserved for patients with excessive, protracted genitourinary bleeding for whom surgical intervention is contemplated.
Recent retrospective analyses of over 60,000 patients treated with AF agents during cardiac surgery suggest an increased risk of all-cause mortality associated with aprotinin use,81,82,83 (relative risk 1.32 to 1.64 versus lysine analog or placebo), although thrombotic disease has not been clearly implicated to explain the mortality excess. Five studies evaluating cardiac graft patency after cardiopulmonary bypass grafting surgery, comparing aprotinin-treated patients with controls, included more than 1,300 patients and demonstrated no increased rate of graft occlusion among those treated with aprotinin.84,85,86,87,88 Secondary thrombotic outcomes following treatment with AF agents during cardiac surgery show variable results. In the Cochrane Systematic Review of 2007, aprotinin use did not affect the incidence of myocardial infarction, stroke, or renal dysfunction following cardiac surgery,89 and there was no association between treatment with TXA or EACA and increased thromboembolic events. An observational study of more than 4,000 patients comparing adverse outcomes following exposure to aprotinin or the lysine analogs suggests a significantly increased incidence of myocardial infarction (55% increase), stroke (181% increase), and renal failure requiring dialysis (more than 200% increase).83 In contrast, the meta-analysis by Brown et al. reported no difference between aprotinin, TXA or EACA, or placebo in the risk of myocardial infarction or stroke.94 More recent trials utilizing aprotinin have reserved the drug for patients with higher risk of bleeding, limiting the retrospective comparison to patients treated without the drug.95 These observational studies led to the randomized blood conservation using antifibrinolytics in a randomized trial (BART) comparing aprotinin to TXA and EACA, which found a 50% increase in death at 30 days among aprotinin-treated patients.96 The data suggest that among patients undergoing cardiac surgery without concurrent thrombogenic stimulus, aprotinin confers a greater risk for adverse outcomes compared with the lysine analogs, and although no definitive evidence exists, suggests a greater tendency to thrombosis.
CLINICAL APPLICATION
Indications for AF therapy include interventions for ongoing hemorrhage or prophylactic administration to prevent bleeding, for which systemic or local fibrinolysis plays a contributory role (Table 77.1).
Fibrinolytic Hemorrhage
Systemic Hyperfibrinolysis
Many pathologic states may generate hyperplasminemia through the release of endothelial stores of tPA in sufficient quantities to overcome fibrinolytic inhibitors and convert plasminogen to plasmin (see Chapters 77 and 98). Plasmin, in turn, degrades fibrinogen and fibrin, and previously stable or new hemostatic sites are at risk of bleeding. Acute conditions that may induce systemic hyperfibrinolysis include heat stroke, hypoxia, hypotension, cardiothoracic surgery, and treatment with thrombolytic agents. Chronic diseases (neoplasm, cirrhosis) may be associated with a systemic hyperfibrinolytic and hemorrhagic state characterized by a shortened euglobulin lysis time, elevated levels of plasma tPA, decreased plasminogen and fibrinogen, and elevated D-dimer. In most cases, tPA release is of limited duration, and an essential therapeutic consideration is directed to the underlying condition.
Acute, systemic hyperfibrin(ogen)olytic states responding dramatically to EACA have been reported in portal hypertension following bowel surgery, a plasminogen-activator-secreting tumor, and with amyloidosis.97,98,99 Chronic hyperfibrinolysis may exist with some neoplasms and with the rare congenital α2-antiplasmin deficiency, and is manifest as a bleeding tendency effectively controlled with chronic antifibrinolytic therapy.100 Acquired α2-antiplasmin deficiency may be seen in acute promyelocytic leukemia, systemic amyloidosis, and metastatic adenocarcinoma, and hemorrhagic complications may be successfully controlled by treatment with AF agents101,102,103,104 Bleeding may accompany treatment with systemic thrombolytic therapy. Because the lysine analogs inhibit plasminogen-activator-mediated fibrinolysis, these agents are reasonable antidotes for acute bleeding attendant PA treatment, although efficacy has not been documented by clinical trial.
Cardiac Surgery
Cardiopulmonary bypass is associated with significant perioperative bleeding, on average ranging from 750 to 1,250 mL and requiring median transfusion of 1.5 to 2.2 U of packed red blood cells.105 The extracorporeal bypass circuit and the surgical wound both induce thrombin and plasmin generation, continuing for up to 24 hours postoperatively.106 Laboratory findings of thrombosis and fibrinolysis, namely, high prothrombin fragment 1 + 2, high plasma D-dimer, shortened clot lysis time, and increased tPA levels,107,108 are demonstrated in blood collected from the chest wound109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125 helping to explain the significant blood loss. Perioperative bleeding leads to a high rate of cardiac reoperations126 and patients requiring blood transfusion during cardiac surgery have a significantly decreased life expectancy.127,128 Concern for the morbidity of significant bleeding and laboratory evidence supportive of a state of hyperfibrinolysis, have led to the extensive prophylactic use of AFs during cardiac operations to block the physiologic manifestations of hyperfibrinolysis and thereby minimize perioperative blood product transfusions.109
Table 77.1 Clinical application of antifibrinolytic therapy
Bleeding State
Clinical Association
Use of Antifibrinolytic Therapy
Comment
Systemic hyperfibrinolysis
Spontaneous plasminemia or following therapeutic thrombolysis
Rare, since hyperfibrinolytic state usually self-limited
If DIC present, AF therapy is contraindicated
Cardiac surgery, with or without cardiopulmonary bypass
Prophylactic administration indicated to lessen blood loss, particularly in high risk circumstance, for example, repeat sternotomy, prolonged pump time, preoperative aspirin use
TXA, EACA decrease blood loss and transfusions vs. placebo. Aprotinin is modestly more effective than TXA/EACA in decreasing transfusions, but increases all-cause mortality
Liver transplant
Prophylaxis useful prior to graft reperfusion to reduce perioperative bleeding and transfusion requirements
Adults with hepatocellular dysfunction more prone to hyperfibrinolytic bleeding; case reports of thrombotic events suggest use may be best guided by coagulation testing
α2-antiplasmin deficiency
Lysine analogs indicated for acute bleeding and prophylaxis
Chronic administration controls lifelong bleeding state in congenital deficiency
Defective hemostasis, followed by normal fibrinolysis
Hemophilia, von Willebrand disease
Indicated to control mucosal bleeding and as adjunctive prohemostatic treatment postoperatively or following acute bleed
Reduces blood loss and use of factor concentrates after dental extraction, synovectomy, joint replacement; likely useful in all postoperative settings
Chronic anticoagulation
Indicated to prevent interruption of therapeutic anticoagulation during dental procedures
May be useful in treatment of minor bleeding episodes in chronically anticoagulated patients
Thrombocytopenia or qualitative platelet dysfunction
Indicated for acute bleeding episodes to reduce platelet transfusions
Less effective if platelet count <10,000/µL
Normal hemostasis, followed by enhanced local fibrinolysis
Upper urinary tract
Indicated to control bleeding from essential hematuria, renal disease postrenal biopsy, and prolonged, spontaneous hematuria in sickle cell disease or hemophilias
Higher risk for obstructive clot formation in hemophiliacs treated simultaneously with factor replacement
Lower urinary tract
May be useful in patients undergoing prostatectomy who have high risk of bleeding
Studies with lysine analogs demonstrate reduced blood loss, without effect on transfusion rate
Dysfunctional uterine bleeding
Indicated for treatment of essential menorrhagia, menorrhagia due to IUD use or cervical conization
Underlying uterine pathology must be excluded
Role in treatment of postpartum hemorrhage undergoing study
Subarachnoid hemorrhage
Reduces incidence of rebleeding, but currently, AF treatment not indicated
Treatment associated with higher rate of vasospasm and ischemic events
Gl bleeding
Indicated to treat acute bleeding episodes from gastric erosions, ulcers, varices
Proven to decrease rate of rebleeding, need for surgical intervention, and mortality
Traumatic hyphema
Indicated in patients with high risk for rebleeding (e.g., aspirin use)
Lysine analogs decrease rate of rebleeding without vision improvement
Mucous membranes
Indicated for recurrent epistaxis; may be useful for excessive bleeding following tonsillectomy or sinus surgery
May be given orally or topically as packing component
Cavernous hemangioma
Used to reverse consumptive coagulopathy prevalent in large lesions
Lysine analog therapy leads to tumor shrinkage and improved symptoms
Chronic urticaria
Indicated for cases resistant to standard therapy
Effective in subset with enhanced local fibrinolysis; elevated D-dimer may predict response to AF treatment
Hereditary angioedema
Long-term prophylaxis against attacks
No effect on symptoms during acute episode
Blood conservation
Orthopedic surgery
Indicated to reduce blood loss in total knee replacement and total hip arthroplasty
Reduces total blood loss and blood transfusion requirements
Neurosurgery
Indicated for multilevel spinal surgery and meningeal procedures with systemic bleeding
AF therapy reduces blood loss and transfusion
Trauma
Indicated in patients presenting after traumatic events with significant bleeding
Associated with decreased mortality and decreased death due to bleeding
Prior to 2006, aprotinin was the most widely used AF agent for cardiac surgery. Its use was first described in 1987 in a trial of 22 patients undergoing repeat sternotomy.110 A Cochrane Database Systematic Review in 2001 evaluated 61 trials of aprotinin in cardiac surgery involving over 7,000 patients and concluded that aprotinin use decreased the rate of red blood cell transfusion by 30% and decreased the need for reoperation due to bleeding by 60%.89 However, the risk of hypersensitivity reactions led the American College of Cardiology and the American Heart Association to restrict the use of aprotinin in primary cardiac surgery for patients at high risk of blood loss,111 but as aprotinin showed greater benefit in patients undergoing repeat sternotomy procedures,112,113 its use was routinely recommended for these patients.114 Although less well studied, two randomized trials of aprotinin in patients undergoing lung resections, who were deemed at high risk for bleeding, demonstrated significantly reduced blood loss, need for transfusion, and need for re-exploration due to bleeding in the treated group versus placebo.115,116 A randomized, double-blind, placebo-controlled trial of 70 patients undergoing myocardial revascularization by total arterial grafting showed that aprotinin reduced the proportion of patients requiring transfusion (39% vs. 77%) and significantly decreased the number of units transfused (0.8 vs. 2.6).117
A study of 56 patients undergoing cardiac surgery found lower blood loss over the first 24 hours postoperatively among patients treated with EACA, an effect that was more marked in patients with cyanotic heart disease or on cardiopulmonary bypass for longer than 1 hour.118 The largest trial of EACA prophylaxis randomized 350 patients undergoing elective cardiac surgery to EACA or placebo and found that patients treated with EACA had significantly less postoperative blood loss, fewer red blood cell transfusions (2.8 U vs. 4.2 U), and fewer reoperations for bleeding,119 without an increase in thrombotic complications. Early reports exploring the use of EACA reported rare adverse events, including DIC unmasked by therapy,67 and significant intracavitary bleeding with the formation of lysis-resistant clots.11,107
Toward finding the optimal dosing schedule, one trial of 90 patients undergoing primary cardiopulmonary bypass surgery randomized three groups: TXA administered prior to bypass, TXA after bypass, or saline placebo. The number of units of transfused blood was significantly less in the TXA prebypass group versus control (0 vs. 4.5).120 A larger trial of 210 randomized patients undergoing primary or repeat sternotomy procedures or valve operations to prophylactic treatment with high-dose TXA prior to initiation of bypass or saline placebo, and found a smaller proportion of patients treated with TXA required blood product transfusion support (13% vs. 31%),121 without an increase in thrombotic events. In two similar trials of prophylactic TXA in pediatric cardiac surgery, one trial of 41 patients undergoing repeat sternotomy treated with high-dose TXA had significantly decreased transfusion support,122 whereas another study of 85 patients showed decreased blood loss without a difference in transfusion versus placebo.123 A trial that compared patients with on-pump (n = 51) versus off-pump (n = 51) procedures, randomized to prophylactic treatment with high-dose TXA or placebo found reduced perioperative blood loss in both on- and off-pump groups, greater with on-pump procedures, with TXA use.124 Prior to elective cardiac surgery, aspirin use is typically discontinued to prevent excessive bleeding, but continuing aspirin may be beneficial by improving survival.129 A meta-analysis by Mcllroy et al.130 of trials of prophylactic AF agents in patients receiving aspirin within 7 days of cardiac surgery found no effect of aspirin coadministration on the benefit of AF agents to reduce bleeding.
Topically applied AF therapy has been utilized as a prophylactic measure to reduce postoperative bleeding following cardiac surgery, the hypothesis being that the pericardium is an important site of fibrinolytic activity131 and that the pericardium is a barrier to absorption of medications.132,133 In a meta-analysis of topical AFs134 administered directly into the sternal wound and into the pericardial cavity, the data suggest that topical AF agents reduce postoperative chest tube drainage (by a mean of 220 mL) and postoperative red blood cell transfusions (by 1 unit per patient), compared with placebo. These data are similar to results after systemic antifibrinolytic therapy.94
The trials cited above all utilized blood loss and transfusion requirements as the primary study outcomes. Head to head trials comparing aprotinin with the synthetic lysine analogs in cardiac surgery show a modest hemostatic advantage for aprotinin,96 and a meta-analysis of 211 trials (21,000 patients) showed a small reduction in red blood cell transfusion (relative risk 0.83).135 Although aprotinin was widely adopted for its slight superiority over the synthetic lysine analogs in terms of blood loss and blood transfusions, recent trials have found aprotinin use to come at a substantial cost in increased mortality and postoperative renal insufficiency136 (see Table 77.2). Three observational cohort studies published between 2007 and 2008 suggested a higher risk of mortality associated with aprotinin exposure during cardiac surgery.81,82,83 From prospectively collected observational data on more than 4,300 patients, Mangano et al.83 found a 48% increased risk of mortality at 5 years in aprotininversus placebo-treated patients, with no such effect on mortality associated with TXA or EACA (vs. placebo). Schneeweiss et al.81 analyzed a European database including patients undergoing cardiac surgery and receiving prophylactic treatment with aprotinin (n = 33,517) or EACA (n = 44,682), and found a 64% increase in the risk for death following treatment with aprotinin. The BART trial of 2,331 high-risk patients undergoing cardiac surgery found aprotinin was associated with a lower rate of massive hemorrhage (9.5% vs. 12.1% for EACA or TXA), but there was a 6% risk of death at 30 days versus 3.9% and 4% amongst patients treated with EACA or TXA (relative risk = 1.53).96 The conclusion of the study was that the modest benefit of aprotinin in terms of bleeding was offset by increased mortality and that aprotinin should not be used in high-risk cardiac surgery.
Given the discordance between hemostatic effectiveness and survival outcomes, future trials of AFs must address clinical endpoints, not just blood loss and transfusion requirements. Although specific patients may derive benefit from aprotinin, at present, this agent is not used in the United States, Canada, or Europe. Concerns remain regarding the safety of the synthetic lysine analogs, for example, TXA is associated with more seizures compared with aprotinin.137
Table 77.2 Antifibrinolytic therapy in cardiac surgery and effect of mortality
Many coagulation defects are present in the setting of endstage liver disease, including increased fibrinolytic activity due to impaired hepatic clearance as well as enhanced endothelial release of tPA. The central role played by the liver in clearing circulating tPA was demonstrated by Illig et al. in a study of patients undergoing aortic clamping during repair of abdominal aortic aneurysms.138 Patients who underwent supraceliac clamping of the aorta compared to those requiring infrarenal clamping experienced a reversible primary fibrinolytic state manifest by a shortened euglobulin lysis time, increased circulating tPA, and decreased α2-antiplasmin concentration, likely caused by hepatic hypoperfusion. Orthotopic liver transplantation is associated with still increased fibrinolytic activity related to ischemic insult to the mesenteric vascular bed and release of activators from the transplanted graft during the anhepatic and reperfusion phases of transplantation.139 To reduce hemorrhage associated with hyperfibrinolysis, an AF agent is commonly administered just prior to graft reperfusion.140 In the study by Segal et al.,141 patients treated with aprotinin during liver transplantation had a blunted increase in circulating tPA, prolonged euglobulin lysis time, decreased peak D-dimer levels, and increased circulating α2-antiplasmin concentration during the reperfusion phase compared with control subjects, consistent with reduced systemic fibrinolytic activity.
Prophylactic treatment with AF agents during orthotopic liver transplantation shows variable results. The European Multicenter Study on the Use of Aprotinin in Liver Transplantation trial, a randomized, double-blind, placebo-controlled study of 137 patients undergoing liver transplantation, demonstrated lower intraoperative blood loss as well as considerably reduced transfusion requirements in patients treated with aprotinin versus placebo, although no differences occurred in 30-day mortality or incidence of thrombotic events.142 Low-dose (2 mg/kg/h), continuous TXA during transplantation demonstrated decreased laboratory parameters of fibrinolysis, but no effect on blood loss or transfusion requirement versus placebo.143 A prospective, placebo-controlled study of 132 patients comparing prophylactic treatment with high-dose TXA (10 mg/kg/h) and EACA (16 mg/kg/h) to placebo demonstrated significantly reduced transfusion requirements for patients treated with TXA, but not for EACA, versus placebo.144 Blinded comparison of TXA and aprotinin in 127 patients showed no difference in blood loss, transfusion requirements, mortality, or thrombotic events between groups.145 Prophylactic AF agents may not be useful in all clinical situations, and may even lead to adverse events.114,140 Coagulation changes and excessive intraoperative bleeding due to hyperfibrinolysis are less common in children undergoing liver transplant, possibly because most are being treated for cholestatic rather than hepatocellular liver failure,146 and adults with primary biliary cirrhosis have less laboratory evidence of hyperfibrinolysis than patients with cirrhosis due to hepatocellular disease.147 A meta-analysis of 23 studies including 1,400 patients undergoing liver transplantation and treated with aprotinin or TXA found that both drugs significantly decreased the transfusion rate with no difference in rate of hepatic artery thrombosis, venous thrombotic events, or 30-day mortality.148 Retrospective analysis of nearly 1,500 patients transplanted for liver disease who were exposed to aprotinin or no AF agent showed an increased risk for reversible renal dysfunction with no difference in the rates of hepatic artery
thrombosis, venous thrombosis, or long-term mortality.149,150 A review of prophylactic administration of AFs during orthotopic liver transplantation reviewed by the Cochrane Database in 2009 concluded that there is no effect on perioperative morbidity or long-term mortality, although the review cautioned that its findings are not robust.151
Only gold members can continue reading. Log In or Register to continue
 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient



